You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5814)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (844)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
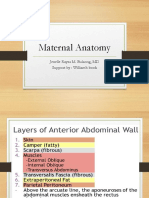
- Maternal Anatomy WilliamsDocument60 pagesMaternal Anatomy WilliamsZari Novela100% (2)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Indwelling Urinary Catheterization 1Document5 pagesIndwelling Urinary Catheterization 1Mercy Anne EcatNo ratings yet
- Urinary Tract Infection: Notre Dame of Marbel UniversityDocument4 pagesUrinary Tract Infection: Notre Dame of Marbel Universityspain michaelisNo ratings yet
- Urinary System DisordersDocument14 pagesUrinary System DisordersGideon P. CasasNo ratings yet
- Catatan Kode IcdDocument10 pagesCatatan Kode IcdAlifvia PramasariNo ratings yet
- Module 17 - Urinary SystemDocument18 pagesModule 17 - Urinary SystemSam TagardaNo ratings yet
- Ncbi - Nlm.nih - Gov-Post-Op Urinary RetentionDocument9 pagesNcbi - Nlm.nih - Gov-Post-Op Urinary RetentiondadupipaNo ratings yet
- What Is The Urinary System and How Does It Work?: KidneysDocument10 pagesWhat Is The Urinary System and How Does It Work?: KidneysAbdelrhman AboodaNo ratings yet
- Uterine ProlapseDocument76 pagesUterine ProlapseRendy Adhitya Pratama75% (4)
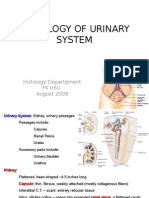
- K2 - Histology of Urinary SystemDocument46 pagesK2 - Histology of Urinary SystemAnonymous EzxZg4uQ63100% (2)
- Chapter 48 Urine EliminationDocument10 pagesChapter 48 Urine EliminationKathleen FrugalidadNo ratings yet
- Catheterization: NCM 107 LabDocument4 pagesCatheterization: NCM 107 LabCatherine PradoNo ratings yet
- Endocrine Function of The Kidney: by Dr. Isam Eldin Mohamed Abd AllaDocument20 pagesEndocrine Function of The Kidney: by Dr. Isam Eldin Mohamed Abd AllaSiddigNo ratings yet
- IPHS For 31 To 50 Bedded With Comments of Sub Group PDFDocument84 pagesIPHS For 31 To 50 Bedded With Comments of Sub Group PDFsaketNo ratings yet
- GENITO URINARY SYSTEM 2nd Year BSC NursingDocument8 pagesGENITO URINARY SYSTEM 2nd Year BSC NursingShreyas WalvekarNo ratings yet
- Flash On: English For NursingDocument16 pagesFlash On: English For NursingNarcisaNo ratings yet
- Medical Student Career Paths BookDocument124 pagesMedical Student Career Paths BookMindi WindmillNo ratings yet
- High-Energy Fractures of The Pelvis and Acetabulum in Pediatric PatientsDocument10 pagesHigh-Energy Fractures of The Pelvis and Acetabulum in Pediatric PatientsFauzan KurniawanNo ratings yet
- Glutathione in The Human Male: Prostate ProblemsDocument11 pagesGlutathione in The Human Male: Prostate Problemsapi-26034055No ratings yet
- Pelvis of RuminantsDocument5 pagesPelvis of RuminantsRachel HayonNo ratings yet
- Intermittent Catheterization and LoFricDocument32 pagesIntermittent Catheterization and LoFricmokilpoNo ratings yet
- Between The Backbone and The Ribs AL QURAN PHENOMENON PDFDocument3 pagesBetween The Backbone and The Ribs AL QURAN PHENOMENON PDFAnonymous SQNcItqXQnNo ratings yet
- Acute Urinary RetentionDocument4 pagesAcute Urinary RetentionRobert DanielNo ratings yet
- Goh 2004Document3 pagesGoh 2004Brendan DiasNo ratings yet
- Imaging of Urethral Stricture Disease: Conrad Maciejewski, Keith RourkeDocument8 pagesImaging of Urethral Stricture Disease: Conrad Maciejewski, Keith RourkeGd SuarantaNo ratings yet
- Urine Cytology: Christine BadilloDocument21 pagesUrine Cytology: Christine BadilloChristine BadilloNo ratings yet
- Hypospadias Epispadias and Bladder Exstrophy: Khalid Abdella (MD) OCTOBER - 11 - 2006Document64 pagesHypospadias Epispadias and Bladder Exstrophy: Khalid Abdella (MD) OCTOBER - 11 - 2006Worku KifleNo ratings yet
- Renal Physiology: Structure & Function of Kidneys and Urinary System, Renal Processes and MicturitionDocument21 pagesRenal Physiology: Structure & Function of Kidneys and Urinary System, Renal Processes and MicturitionSufyan MirzaNo ratings yet
- Elimination: Bowel and UrineDocument27 pagesElimination: Bowel and UrineYuliana Nur KolifahNo ratings yet
- Anatomy of Urinary SystemDocument34 pagesAnatomy of Urinary Systemhana100% (1)