You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5806)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (842)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Concepts of Industrial ManagementDocument9 pagesConcepts of Industrial ManagementSandeep Shrivastava50% (2)
- The Good News About Nuclear Destruction!Document7 pagesThe Good News About Nuclear Destruction!Ven GeanciaNo ratings yet
- Nestle AnalysisDocument20 pagesNestle AnalysisDiv Kabra100% (1)
- Formula, Good or Not For The Babies ?: Written By: Rakhmah Sari Indah C. - XII P7 /28Document4 pagesFormula, Good or Not For The Babies ?: Written By: Rakhmah Sari Indah C. - XII P7 /28Inda KecilNo ratings yet
- Module 14 Review QuestionsDocument3 pagesModule 14 Review QuestionsUnnamed homosapienNo ratings yet
- 2 AnticholinesterasesDocument55 pages2 AnticholinesterasesSudhakar LakavathNo ratings yet
- Self Inspection of Quality AssuranceDocument5 pagesSelf Inspection of Quality Assuranceanoushia alviNo ratings yet
- Presentasi Xario SeriesDocument38 pagesPresentasi Xario SeriesRSBM Yanmed100% (1)
- Folio Kajian Kes WawaDocument11 pagesFolio Kajian Kes Wawanur syahkinaNo ratings yet
- To 1 Bahasa Inggris 2020 2021Document13 pagesTo 1 Bahasa Inggris 2020 2021ana bornengNo ratings yet
- BIOBASE SCSJ-V Series User ManualDocument25 pagesBIOBASE SCSJ-V Series User Manualsoporte03No ratings yet
- The Ladli Scheme in India ReportDocument26 pagesThe Ladli Scheme in India ReportManoj BhalaniNo ratings yet
- Understanding The Psycho-Social and Health Problems Faced by Homeless Population in Visakhapatnam CityDocument8 pagesUnderstanding The Psycho-Social and Health Problems Faced by Homeless Population in Visakhapatnam CityMutluri AbrahamNo ratings yet
- Synerquest 2014 Annual Calendar of DOLE-prescribed CoursesDocument3 pagesSynerquest 2014 Annual Calendar of DOLE-prescribed CoursesrobinrubinaNo ratings yet
- Arntz 1999 Childhood Imagery Rescripting Paper PDFDocument26 pagesArntz 1999 Childhood Imagery Rescripting Paper PDFelliotNo ratings yet
- Intern TicklerDocument10 pagesIntern TicklerRem AlfelorNo ratings yet
- Dengue Fever 2Document5 pagesDengue Fever 2Gayitiri MenonNo ratings yet
- What Do We Know About The Food We Eat?: Teaching and Learning Activities, Including Assessment OpportunitiesDocument14 pagesWhat Do We Know About The Food We Eat?: Teaching and Learning Activities, Including Assessment OpportunitiesaravindyellowNo ratings yet
- ABCDEFGHI Systematic Approach To Wound Assessment and ManagementDocument36 pagesABCDEFGHI Systematic Approach To Wound Assessment and ManagementsaerodinNo ratings yet
- Simple Magazine #17Document5 pagesSimple Magazine #17tôn thất minh khangNo ratings yet
- Define Hospital ManagementDocument4 pagesDefine Hospital ManagementRenit AntoNo ratings yet
- Intraoperative CholangiogramDocument3 pagesIntraoperative CholangiogramPauline Jimenea100% (2)
- Neonatology Short Case History Taking Format by SPKathankar 1Document5 pagesNeonatology Short Case History Taking Format by SPKathankar 1HkNo ratings yet
- Head and NeckDocument21 pagesHead and NeckUday PrabhuNo ratings yet
- Faradic: Reference ManualDocument19 pagesFaradic: Reference ManualrobertNo ratings yet
- Inclusivness AssignmentDocument17 pagesInclusivness AssignmentEphrem ChernetNo ratings yet
- Carestream Quantum Medical Imaging QS 550 Tubestand DC30 034 RH 201506Document50 pagesCarestream Quantum Medical Imaging QS 550 Tubestand DC30 034 RH 201506D “DAKHobby” KNo ratings yet
- 12 - DEMONSTRATION INSTRUCTION FOR THE TRAINEE AND THE TRAINER Rev01Document2 pages12 - DEMONSTRATION INSTRUCTION FOR THE TRAINEE AND THE TRAINER Rev01Crisostomo MateoNo ratings yet
- Provide First AidDocument3 pagesProvide First AidluviumNo ratings yet
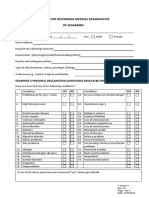
- Format For Recording Medical Examinatios of SeafarersDocument4 pagesFormat For Recording Medical Examinatios of SeafarersАлексNo ratings yet