You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- "God's Hotel: A Doctor A Hospital, and A Pilgrimage Into The Heart of Medicine" by Victoria SweetDocument43 pages"God's Hotel: A Doctor A Hospital, and A Pilgrimage Into The Heart of Medicine" by Victoria Sweetwamu885No ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Glenn's Urologic Surgery PDFDocument992 pagesGlenn's Urologic Surgery PDFPol Pol100% (1)
- Perioperative Nursing Surgical ScrubbingDocument6 pagesPerioperative Nursing Surgical ScrubbingGabrielle EvangelistaNo ratings yet
- Dekker V Weida Amicus Brief by 17 AGsDocument35 pagesDekker V Weida Amicus Brief by 17 AGsSarah WeaverNo ratings yet
- Endoscopy of GI TractDocument358 pagesEndoscopy of GI TractEngin UçarNo ratings yet
- Da Vinci Xi System User Manual (551400-11)Document302 pagesDa Vinci Xi System User Manual (551400-11)Juan Ramirez93% (15)
- Doctors List at Icf HospitalDocument4 pagesDoctors List at Icf HospitalMunusamy RajiNo ratings yet
- 1684 - Hemal Patel PPT 7 - 845Document6 pages1684 - Hemal Patel PPT 7 - 845jdchandrapal4980No ratings yet
- 3325-Ulcer Unoperated PDFDocument2 pages3325-Ulcer Unoperated PDFjdchandrapal4980No ratings yet
- 680 DGHDocument4 pages680 DGHjdchandrapal4980No ratings yet
- 1684 - Hemal Patel PPT 7 - 845Document6 pages1684 - Hemal Patel PPT 7 - 845jdchandrapal4980No ratings yet
- LIC Jeevan Umang plan analysis for Hemal PatelDocument6 pagesLIC Jeevan Umang plan analysis for Hemal Pateljdchandrapal4980No ratings yet
- 1888 - Harsh - Pro-MixDocument5 pages1888 - Harsh - Pro-Mixjdchandrapal4980No ratings yet
- Nidhi Investment Consultant: Magic Mix Illustration For Mr. AB Prafulbhai (Age 18)Document2 pagesNidhi Investment Consultant: Magic Mix Illustration For Mr. AB Prafulbhai (Age 18)jdchandrapal4980No ratings yet
- Nidhi Investment Consultant: Magic Mix Illustration For Mr. AB Prafulbhai (Age 18)Document2 pagesNidhi Investment Consultant: Magic Mix Illustration For Mr. AB Prafulbhai (Age 18)jdchandrapal4980No ratings yet
- 1888 - Mast ABCDocument6 pages1888 - Mast ABCjdchandrapal4980No ratings yet
- 1384 - Jitendra P Jain - 814-35 - 845-15Document5 pages1384 - Jitendra P Jain - 814-35 - 845-15jdchandrapal4980No ratings yet
- 1384 - Bhagvatilal V JainDocument4 pages1384 - Bhagvatilal V Jainjdchandrapal4980No ratings yet
- 1202 - Dhairya - 1Document5 pages1202 - Dhairya - 1jdchandrapal4980No ratings yet
- Nidhi Investment Consultant: Magic Mix Illustration For Mr. Nirmal Saremal Surat (Age 47)Document3 pagesNidhi Investment Consultant: Magic Mix Illustration For Mr. Nirmal Saremal Surat (Age 47)jdchandrapal4980No ratings yet
- 1384 - Nirmal M Jain - 814Document3 pages1384 - Nirmal M Jain - 814jdchandrapal4980No ratings yet
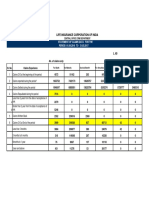
- Periodic Disclosures: FORM L-38 Business Acquisition Through Different Channels (Individuals)Document1 pagePeriodic Disclosures: FORM L-38 Business Acquisition Through Different Channels (Individuals)jdchandrapal4980No ratings yet
- Nidhi Investment Consultant: Magic Mix Illustration For Mr. Nirmal Saremal Surat (Age 47)Document3 pagesNidhi Investment Consultant: Magic Mix Illustration For Mr. Nirmal Saremal Surat (Age 47)jdchandrapal4980No ratings yet
- LIFE INSURANCE CORP OF INDIA PERIODIC DISCLOSURESDocument1 pageLIFE INSURANCE CORP OF INDIA PERIODIC DISCLOSURESjdchandrapal4980No ratings yet
- LIC India periodic disclosures form for premium and number of lives by policy typeDocument2 pagesLIC India periodic disclosures form for premium and number of lives by policy typejdchandrapal4980No ratings yet
- LIC - 39 Agening of Claims Statement - 31 03 2017 PDFDocument1 pageLIC - 39 Agening of Claims Statement - 31 03 2017 PDFjdchandrapal4980No ratings yet
- "Insure & Be Secure": Mr. Hitendra MakwanaDocument3 pages"Insure & Be Secure": Mr. Hitendra Makwanajdchandrapal4980No ratings yet
- LIC - 40 - Statements of Claims Data - 31 .3 2017 PDFDocument1 pageLIC - 40 - Statements of Claims Data - 31 .3 2017 PDFjdchandrapal4980No ratings yet
- Lic 4 Prem&comm 31-03-2017 PDFDocument1 pageLic 4 Prem&comm 31-03-2017 PDFjdchandrapal4980No ratings yet
- IRDA Public Disclosure on LIC's Solvency MarginDocument1 pageIRDA Public Disclosure on LIC's Solvency Marginjdchandrapal4980No ratings yet
- Lic - 6 - Op Exp&ben Paid - 31 03 2017 PDFDocument2 pagesLic - 6 - Op Exp&ben Paid - 31 03 2017 PDFjdchandrapal4980No ratings yet
- L 25 - Individualr Dec14 PDFDocument1 pageL 25 - Individualr Dec14 PDFKarlosNo ratings yet
- Lic 2 P&L 31-03-2017 PDFDocument1 pageLic 2 P&L 31-03-2017 PDFjdchandrapal4980No ratings yet
- Lic 3 BS 31-03-2017 PDFDocument2 pagesLic 3 BS 31-03-2017 PDFjdchandrapal4980No ratings yet
- Lic 1 Ra 31-03-2017Document1 pageLic 1 Ra 31-03-2017jdchandrapal4980No ratings yet
- 00 Marketing Research - Process - Design - 2Document31 pages00 Marketing Research - Process - Design - 2jdchandrapal4980No ratings yet
- Resume CourtneyDocument1 pageResume Courtneyapi-508129555No ratings yet
- Program en Icad 2018Document16 pagesProgram en Icad 2018huyenthanh1807No ratings yet
- Healthcare Investor Licensing GuideDocument35 pagesHealthcare Investor Licensing GuideShankar SanyalNo ratings yet
- Tugas Bahasa Inggris " Communicating With Patients ": Oleh: Putu Mika Wahyuni C1118011 V A KeperawatanDocument4 pagesTugas Bahasa Inggris " Communicating With Patients ": Oleh: Putu Mika Wahyuni C1118011 V A KeperawatanMika WahyuniNo ratings yet
- Screw Versus Cement For Implant Prosthesis Installation.: Part 1: The Logic Behind The ArgumentsDocument47 pagesScrew Versus Cement For Implant Prosthesis Installation.: Part 1: The Logic Behind The ArgumentsAya Ibrahim YassinNo ratings yet
- Skin Substitutes and Extracellular Matrix Scaffolds - Musculoskeletal KeyDocument15 pagesSkin Substitutes and Extracellular Matrix Scaffolds - Musculoskeletal KeyPerusend EirlNo ratings yet
- Case Scenario/Situation Answer/Explanation: NCM 101 RLE - Health AssessmentDocument2 pagesCase Scenario/Situation Answer/Explanation: NCM 101 RLE - Health AssessmentmaryNo ratings yet
- Evolution of Internal Fixation in Long Bone FracturesDocument18 pagesEvolution of Internal Fixation in Long Bone FracturesTraumatologia HEBANo ratings yet
- Redundant: A Case of Complicated Dolichocolon in A NeonateDocument4 pagesRedundant: A Case of Complicated Dolichocolon in A NeonateCassNo ratings yet
- Professional Negligence and Res Ipsa LoquiturDocument7 pagesProfessional Negligence and Res Ipsa LoquiturAlthea AlcalaNo ratings yet
- LEEP 1000 Workstation Operating Manual 220vDocument24 pagesLEEP 1000 Workstation Operating Manual 220vpatrickNo ratings yet
- Specimen Crib SheetDocument5 pagesSpecimen Crib SheetMario QuinteroNo ratings yet
- Hernia - Femoral Hernia, Epigastric Hernia, Paraumbilical Hernia, Incisional HerniaDocument29 pagesHernia - Femoral Hernia, Epigastric Hernia, Paraumbilical Hernia, Incisional HerniaKuruNo ratings yet
- PVIDDocument4 pagesPVIDNandan.m.pNo ratings yet
- Case Study: Alano Vs Magud-Logmao (G.R. NO. 175540, April 7, 2014)Document2 pagesCase Study: Alano Vs Magud-Logmao (G.R. NO. 175540, April 7, 2014)ROLAND BRIONESNo ratings yet
- Runner's Knee (Patellofemoral Pain) : CausesDocument4 pagesRunner's Knee (Patellofemoral Pain) : CausesBarath KannanNo ratings yet
- Long Span Ridge With Precision AttachmentDocument6 pagesLong Span Ridge With Precision AttachmentSHAILJA KATIYARNo ratings yet
- 17 - 2022 Advt VaranasiDocument3 pages17 - 2022 Advt VaranasiNamita SinhaNo ratings yet
- SC Overturns PRC Revocation of Doctor's LicenseDocument3 pagesSC Overturns PRC Revocation of Doctor's LicenseEloisa SalitreroNo ratings yet
- CH1 - Medical Tourism and Wellness Tourism CH 1Document23 pagesCH1 - Medical Tourism and Wellness Tourism CH 1Dianara FernandezNo ratings yet
- AO Trauma India Course Calendar 2023Document4 pagesAO Trauma India Course Calendar 2023Aravind RaviNo ratings yet
- Dynamic Tendon Transfer For The Treatment of Palmar Midcarpal Instability: A Case ReportDocument4 pagesDynamic Tendon Transfer For The Treatment of Palmar Midcarpal Instability: A Case ReportasclepiuspdfsNo ratings yet
- Office Memorandum Dated 17.10Document21 pagesOffice Memorandum Dated 17.10Pradeep SaxenaNo ratings yet