You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (842)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5806)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Risk Assessment Backfilling Around Foul Sewer and Storm Warter ManholesDocument8 pagesRisk Assessment Backfilling Around Foul Sewer and Storm Warter ManholesMidhunRameshThuvasseryNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Externalities & Public GoodsDocument13 pagesExternalities & Public GoodsAkshay ModakNo ratings yet
- I Love You But I M Not in Love With YouDocument31 pagesI Love You But I M Not in Love With YouRaluca CotetiuNo ratings yet
- Skin CareDocument5 pagesSkin Carejoseph100% (1)
- Co2 Laser CatalogueDocument24 pagesCo2 Laser CatalogueBlin RodsNo ratings yet
- Auricular Causative Diagnosis-Finding The Roots of Diseases: A Study of Clinical CasesDocument11 pagesAuricular Causative Diagnosis-Finding The Roots of Diseases: A Study of Clinical Casesyan92120No ratings yet
- Quality of Service of The School Canteen: Part I. Socio-Demographic Profile QuestionnaireDocument2 pagesQuality of Service of The School Canteen: Part I. Socio-Demographic Profile QuestionnaireKB Salandores50% (2)
- Book 1Document50 pagesBook 1Varudhini PatkiNo ratings yet
- Cleaning Validation Guidelines - Health CanadaDocument7 pagesCleaning Validation Guidelines - Health Canadahafeez50No ratings yet
- Department of Pharmaceutical ChemistryDocument13 pagesDepartment of Pharmaceutical ChemistrySuvarna KiniNo ratings yet
- Teva AR 2017 - PharmaceuticalIndustriesLtdDocument805 pagesTeva AR 2017 - PharmaceuticalIndustriesLtdBhushanNo ratings yet
- Lack of SleepDocument14 pagesLack of SleepBrigitta VianneyNo ratings yet
- (Comprehensive Geriatric Assessment) Experiencia Com Idosos de Colombia E BrasilDocument27 pages(Comprehensive Geriatric Assessment) Experiencia Com Idosos de Colombia E BrasilBrisa NarvaezNo ratings yet
- Full Length Research Article: ISSN: 2230-9926Document5 pagesFull Length Research Article: ISSN: 2230-9926Nisarg SutharNo ratings yet
- Analytical Exposition ExerciseDocument7 pagesAnalytical Exposition ExerciseECC SMAN 1 BaleendahNo ratings yet
- Synerquest 2014 Annual Calendar of DOLE-prescribed CoursesDocument3 pagesSynerquest 2014 Annual Calendar of DOLE-prescribed CoursesrobinrubinaNo ratings yet
- Level 6 Passage 2Document4 pagesLevel 6 Passage 2Osvaldo Soto RodeNo ratings yet
- Npi NCMHDocument6 pagesNpi NCMHJoshua DauzNo ratings yet
- Final ArticleDocument28 pagesFinal Articlesummaiya RizwanNo ratings yet
- Notification No.19151 - Revised Guidelines MUKTADocument22 pagesNotification No.19151 - Revised Guidelines MUKTADeepak PeraNo ratings yet
- Organisational Development Strategy - 2011-12-2015-16Document33 pagesOrganisational Development Strategy - 2011-12-2015-16grisNo ratings yet
- Water Intoxication - Is It Possible To Drink Too Much Water???Document11 pagesWater Intoxication - Is It Possible To Drink Too Much Water???NoraNo ratings yet
- What Has Psychotherapy Inherited From Carl RogersDocument4 pagesWhat Has Psychotherapy Inherited From Carl Rogerscris kalitoNo ratings yet
- AnaPhy Skin Cancer Case Study-BASCODocument6 pagesAnaPhy Skin Cancer Case Study-BASCOChristine Jane BascoNo ratings yet
- HIV and YogaDocument3 pagesHIV and YogaAbhaya Raj UpadhayaNo ratings yet
- Tennessee Hazard Mitigation Plan 2018 FINALDocument388 pagesTennessee Hazard Mitigation Plan 2018 FINALAnonymous GF8PPILW5100% (1)
- Monouso Ge Healthcare, Catalogo Prodotti GE HealthcareDocument263 pagesMonouso Ge Healthcare, Catalogo Prodotti GE HealthcareAlessandro ArmaroliNo ratings yet
- ABCDEFGHI Systematic Approach To Wound Assessment and ManagementDocument36 pagesABCDEFGHI Systematic Approach To Wound Assessment and ManagementsaerodinNo ratings yet
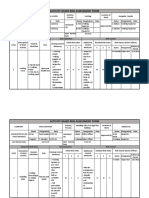
- Activity-Based Risk Assessment Form: Wearing InspectorDocument3 pagesActivity-Based Risk Assessment Form: Wearing InspectorSherly MagatNo ratings yet
- Hostel Rules and RegulationsDocument11 pagesHostel Rules and RegulationsAkshet PatelNo ratings yet