You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5795)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- 300 EDIT Dental Facts NBDE - WITH PICTURESDocument39 pages300 EDIT Dental Facts NBDE - WITH PICTURESCamellia ShahmoradiNo ratings yet
- センタロイシリーズDocument4 pagesセンタロイシリーズcmmbNo ratings yet
- Kamatuday Appliance (Triple-Banded Space Regainer) : An Innovative ApplianceDocument3 pagesKamatuday Appliance (Triple-Banded Space Regainer) : An Innovative ApplianceIJAR JOURNALNo ratings yet
- Cementum - A Dynamic Structure UdayDocument85 pagesCementum - A Dynamic Structure UdayVishali Rayapudi100% (1)
- The Butterfly Effect: An Investigation of Sectioned Roots: Basic Research - BiologyDocument3 pagesThe Butterfly Effect: An Investigation of Sectioned Roots: Basic Research - BiologyOmar TalibNo ratings yet
- J Clinic Periodontology 2019 Tonetti Implementation of The New Classification of Periodontal DiseasesDocument8 pagesJ Clinic Periodontology 2019 Tonetti Implementation of The New Classification of Periodontal DiseasesMuhammad Hassan memonNo ratings yet
- Occlusion. Static Occlusion, Dynamic Occlusion and Guidance - Verifiable CPD Online - DentistryDocument5 pagesOcclusion. Static Occlusion, Dynamic Occlusion and Guidance - Verifiable CPD Online - Dentistryaziz2007No ratings yet
- Abutment Options For The Restoration of The Malalinged Implant 2016 PDFDocument5 pagesAbutment Options For The Restoration of The Malalinged Implant 2016 PDFmarwa100% (1)
- Daftar Pustaka: Universitas Sumatera UtaraDocument3 pagesDaftar Pustaka: Universitas Sumatera UtaraMegaRafikaBarorohNo ratings yet
- SurveyorDocument33 pagesSurveyorChittan Mac Maisnam100% (1)
- Nancy Saghian PDFDocument3 pagesNancy Saghian PDFBeverlyHillsWeeklyNo ratings yet
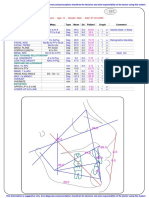
- Ricketts Analysis: Max. PositionDocument1 pageRicketts Analysis: Max. Positionmonwarul azizNo ratings yet
- Working Length DeterminationDocument26 pagesWorking Length DeterminationanmolNo ratings yet
- A To Z Orthodontics Vol 10 Removable Orthodontic ApplianceDocument34 pagesA To Z Orthodontics Vol 10 Removable Orthodontic ApplianceMa Lyn GabayeronNo ratings yet
- Manual de Endodoncia Basica V6Document6 pagesManual de Endodoncia Basica V6evripidis tziokasNo ratings yet
- Adolescent Oral Health Care: Latest RevisionDocument10 pagesAdolescent Oral Health Care: Latest Revisionnona aryanNo ratings yet
- Nano DentistryDocument6 pagesNano DentistryanugrasNo ratings yet
- Orthodontic Cyber Journal Year 2001 Issue 6Document35 pagesOrthodontic Cyber Journal Year 2001 Issue 6Sankhya100% (1)
- Moh IcdasDocument32 pagesMoh Icdasana raihana0% (1)
- Vital Pulp Therapy 1Document6 pagesVital Pulp Therapy 1Mostafa Afifi Ali100% (1)
- L4 - All Ceramic PreparationsDocument41 pagesL4 - All Ceramic Preparationstalal_11100% (1)
- Lec 10 Technology of OperativeDocument8 pagesLec 10 Technology of OperativeHassan TantawyNo ratings yet
- Tetric N-Bond UniversalDocument13 pagesTetric N-Bond UniversalchimedbatorNo ratings yet
- Performantele MTADocument5 pagesPerformantele MTAana aNo ratings yet
- Section 010 Centric RelationDocument21 pagesSection 010 Centric RelationSummer Flowers100% (1)
- Department of Fixed Prosthodontics: (Only One Answer Is Allowed)Document11 pagesDepartment of Fixed Prosthodontics: (Only One Answer Is Allowed)Hassan TantawyNo ratings yet
- Integrating Conventional and CAD/CAM Digital Techniques For Establishing Canine Protected Articulation: A Clinical ReportDocument5 pagesIntegrating Conventional and CAD/CAM Digital Techniques For Establishing Canine Protected Articulation: A Clinical ReportDragos CiongaruNo ratings yet
- Midterm Surgery PYQsDocument77 pagesMidterm Surgery PYQs6vqk4z8wnhNo ratings yet
- Partial Coverage PPT FinalDocument83 pagesPartial Coverage PPT FinalTotta Ayman50% (2)
- An Impression Technique For Patients With Fixed Orthodontic AppliancesDocument2 pagesAn Impression Technique For Patients With Fixed Orthodontic Appliancesmoji_puiNo ratings yet