You might also like
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Dialogue Confined To Two Speakers:: Nama: Lyfa Zulianna Nim: 181030100198 Kelas: 6 F KeperawatanDocument2 pagesDialogue Confined To Two Speakers:: Nama: Lyfa Zulianna Nim: 181030100198 Kelas: 6 F Keperawatanlyfia zuliannaNo ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Exercise Pertemuan 9Document4 pagesExercise Pertemuan 9lyfia zuliannaNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Tugas Bing PTM 8 - LyfiaDocument5 pagesTugas Bing PTM 8 - Lyfialyfia zuliannaNo ratings yet
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Tugas Bing PTM 14 - Lyfia Z.Document4 pagesTugas Bing PTM 14 - Lyfia Z.lyfia zuliannaNo ratings yet
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Komunitas Internasional 2Document5 pagesKomunitas Internasional 2lyfia zuliannaNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- PTM 5 Bhs Inggris, Lyfia 5FDocument2 pagesPTM 5 Bhs Inggris, Lyfia 5Flyfia zuliannaNo ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Bing PTM 7 - LyfiaDocument2 pagesBing PTM 7 - Lyfialyfia zuliannaNo ratings yet
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Bing PTM 7 - LyfiaDocument2 pagesBing PTM 7 - Lyfialyfia zuliannaNo ratings yet
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Translation ExerciseDocument2 pagesTranslation Exerciselyfia zuliannaNo ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Tugas English For Nurses Iv, April 6. 2020 (Edit)Document3 pagesTugas English For Nurses Iv, April 6. 2020 (Edit)lyfia zuliannaNo ratings yet
- THE EXERCISE OF CONDITIONAL SENTENCE FOR 4th STUDENTSDocument2 pagesTHE EXERCISE OF CONDITIONAL SENTENCE FOR 4th STUDENTSlyfia zuliannaNo ratings yet
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Material of The 5TH Meeting. March 30, 2020Document3 pagesThe Material of The 5TH Meeting. March 30, 2020lyfia zuliannaNo ratings yet
- Translation ExerciseDocument2 pagesTranslation Exerciselyfia zuliannaNo ratings yet
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Translation ExerciseDocument2 pagesTranslation Exerciselyfia zuliannaNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Makalah PKN - OdtDocument2 pagesMakalah PKN - Odtlyfia zuliannaNo ratings yet
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Tugas 2Document3 pagesTugas 2lyfia zuliannaNo ratings yet
- Lights UpDocument1 pageLights Uplyfia zuliannaNo ratings yet
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Makalah Konsul Komunikasi Keperawatan Jean WatsonDocument2 pagesMakalah Konsul Komunikasi Keperawatan Jean Watsonlyfia zuliannaNo ratings yet
- Makalah PKNDocument2 pagesMakalah PKNlyfia zuliannaNo ratings yet
- Of The Month Is Live. 100+ Subjects. Participate Now!: Sanfoundry Certification ContestDocument4 pagesOf The Month Is Live. 100+ Subjects. Participate Now!: Sanfoundry Certification ContestBaydaa QaidyNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Modern Myth and Magical Face Shifting Technology in Girish Karnad Hayavadana and NagamandalaDocument2 pagesModern Myth and Magical Face Shifting Technology in Girish Karnad Hayavadana and NagamandalaKumar KumarNo ratings yet
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
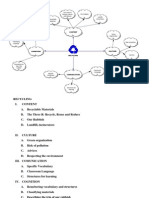
- Recycling Mind MapDocument2 pagesRecycling Mind Mapmsole124100% (1)
- Siprotec 7ut82 ProfileDocument2 pagesSiprotec 7ut82 ProfileOliver Atahuichi TorrezNo ratings yet
- Plato: Epistemology: Nicholas WhiteDocument2 pagesPlato: Epistemology: Nicholas WhiteAnonymous HCqIYNvNo ratings yet
- Chapter 1 (PLC)Document9 pagesChapter 1 (PLC)Kibria PrangonNo ratings yet
- Mullā Ṣadrā and Causation - Rethinking A Problem in Later Islamic Philosophy AuthorDocument15 pagesMullā Ṣadrā and Causation - Rethinking A Problem in Later Islamic Philosophy AuthorKadag LhundrupNo ratings yet
- Academic Reading: All Answers Must Be Written On The Answer SheetDocument21 pagesAcademic Reading: All Answers Must Be Written On The Answer SheetLemon MahamudNo ratings yet
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- LJ-V7080 DatasheetDocument2 pagesLJ-V7080 DatasheetOrhan DenizliNo ratings yet
- Iron Ore ProcessDocument52 pagesIron Ore Processjafary448067% (3)
- Dell W2306C LCD Monitor Service ManualDocument104 pagesDell W2306C LCD Monitor Service ManualIsrael B ChavezNo ratings yet
- DEEP ECOLOGY - An Intro - McLaughlinDocument5 pagesDEEP ECOLOGY - An Intro - McLaughlinCarlo MagcamitNo ratings yet
- Ventricular Septal DefectDocument9 pagesVentricular Septal DefectpepotchNo ratings yet
- Generalized Anxiety DisorderDocument24 pagesGeneralized Anxiety DisorderEula Angelica OcoNo ratings yet
- Thermoplastic Tubing: Catalogue 5210/UKDocument15 pagesThermoplastic Tubing: Catalogue 5210/UKGeo BuzatuNo ratings yet
- Electrical Power System Device Function NumberDocument2 pagesElectrical Power System Device Function Numberdan_teegardenNo ratings yet
- How To Eat WellDocument68 pagesHow To Eat WelleledidiNo ratings yet
- Stanley B. Alpern - Amazons of Black Sparta - The Women Warriors of Dahomey-New York University Press (2011)Document308 pagesStanley B. Alpern - Amazons of Black Sparta - The Women Warriors of Dahomey-New York University Press (2011)georgemultiplusNo ratings yet
- Manufacuring EngineeringDocument3 pagesManufacuring Engineeringapi-79207659No ratings yet
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Wild T1 TheodoliteDocument61 pagesThe Wild T1 TheodoliteCJLara100% (1)
- John Sisler CISSP Study GuideDocument126 pagesJohn Sisler CISSP Study GuideAnthonyNo ratings yet
- Greater Occipital Nerve Block: Pain ManagementDocument3 pagesGreater Occipital Nerve Block: Pain Managementkillingeyes177No ratings yet
- Sample Dilapidation ReportDocument8 pagesSample Dilapidation ReportczarusNo ratings yet
- Bolt Action Italian Painting GuideDocument7 pagesBolt Action Italian Painting GuideTirmcdhol100% (2)
- Simple Roll-Type: A Loud SpeakerDocument1 pageSimple Roll-Type: A Loud SpeakerEudes SilvaNo ratings yet
- DCS YokogawaDocument17 pagesDCS Yokogawasswahyudi100% (1)
- Raspberry Pi 3 and BeagleBone Black For Engineers - UpSkill Learning 124Document124 pagesRaspberry Pi 3 and BeagleBone Black For Engineers - UpSkill Learning 124Dragan IvanovNo ratings yet
- Donna Hay Magazine 2014-10-11 PDFDocument172 pagesDonna Hay Magazine 2014-10-11 PDFlekovic_tanjaNo ratings yet
- Table 1 Minimum Separation DistancesDocument123 pagesTable 1 Minimum Separation DistancesjhonNo ratings yet
- Product Lifecycle Management and Sustainable Development in The Context of Industry 4.0: A Systematic Literature ReviewDocument10 pagesProduct Lifecycle Management and Sustainable Development in The Context of Industry 4.0: A Systematic Literature ReviewJosip StjepandicNo ratings yet
- Workin' Our Way Home: The Incredible True Story of a Homeless Ex-Con and a Grieving Millionaire Thrown Together to Save Each OtherFrom EverandWorkin' Our Way Home: The Incredible True Story of a Homeless Ex-Con and a Grieving Millionaire Thrown Together to Save Each OtherNo ratings yet
- Do You Believe in Magic?: The Sense and Nonsense of Alternative MedicineFrom EverandDo You Believe in Magic?: The Sense and Nonsense of Alternative MedicineNo ratings yet
- When Helping Hurts: How to Alleviate Poverty Without Hurting the Poor . . . and YourselfFrom EverandWhen Helping Hurts: How to Alleviate Poverty Without Hurting the Poor . . . and YourselfRating: 5 out of 5 stars5/5 (36)