You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- DietDocument1 pageDietFrei MagsinoNo ratings yet
- Integrative Engineering A: Algebra and Advance AlgebraDocument40 pagesIntegrative Engineering A: Algebra and Advance Algebralynser chuaNo ratings yet
- Laplace Table PDFDocument2 pagesLaplace Table PDFFrei MagsinoNo ratings yet
- Elements LiteratureDocument25 pagesElements LiteratureFrei MagsinoNo ratings yet
- Acquired Books Prof ENGG. 2012 2016 RevDocument27 pagesAcquired Books Prof ENGG. 2012 2016 RevFrei Magsino100% (1)
- Character: The Seven Key Elements of FictionDocument5 pagesCharacter: The Seven Key Elements of FictionKlint VanNo ratings yet
- Power and Industrial Plant Engineering TerminologiesDocument10 pagesPower and Industrial Plant Engineering TerminologiesFrei MagsinoNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (120)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- 58 Drug Information ResourcesDocument2 pages58 Drug Information Resourcesagent2catNo ratings yet
- Pharmaceutical Health Care IndustryDocument120 pagesPharmaceutical Health Care IndustryJanella Garcia50% (2)
- GATE 2000 Que PaperDocument10 pagesGATE 2000 Que PaperSHRIKANTNo ratings yet
- Roll No - 24201916089Document69 pagesRoll No - 24201916089Rambo FeverNo ratings yet
- Pharmacology Test 1Document39 pagesPharmacology Test 1Niki BolinNo ratings yet
- Farmacognosia Molecular, Lu-Qi Huang PDFDocument233 pagesFarmacognosia Molecular, Lu-Qi Huang PDFdavidNo ratings yet
- Pediatric Drug ReferenceDocument86 pagesPediatric Drug Referenceromaine_as100% (1)
- Drug Interactions and Drug Interaction CDocument6 pagesDrug Interactions and Drug Interaction CYağmur SoysalNo ratings yet
- Roquette Pharma Oral Dosage BROCHURE LYCATAB Pregelatinised Maize StarchDocument26 pagesRoquette Pharma Oral Dosage BROCHURE LYCATAB Pregelatinised Maize StarchRong ZhaoNo ratings yet
- BODYTECH Price-1Document1 pageBODYTECH Price-1nk4xp5ds6rNo ratings yet
- PP Topic 3 PDFDocument4 pagesPP Topic 3 PDFMatNo ratings yet
- PEP Practice QuestionsDocument8 pagesPEP Practice QuestionsCynthia ObiNo ratings yet
- Drug Related Problems: A Systemic Literature ReviewDocument7 pagesDrug Related Problems: A Systemic Literature ReviewBaru Chandrasekhar RaoNo ratings yet
- Pharmacokinetics and PharmacodynamicsDocument23 pagesPharmacokinetics and PharmacodynamicsFahmi NoorNo ratings yet
- Why Is This Medication Prescribed?: Before Taking ProtriptylineDocument5 pagesWhy Is This Medication Prescribed?: Before Taking ProtriptylineAnthony LopezNo ratings yet
- Laporan Kendali Barang - 31 Dec 2022Document33 pagesLaporan Kendali Barang - 31 Dec 2022Alfred OctavianusNo ratings yet
- Nausea and Vomiting in Palliative Care Audit PresentationDocument68 pagesNausea and Vomiting in Palliative Care Audit PresentationGonzalo MaldonadoNo ratings yet
- LED-Face-Mask-Consultation-Form - 2Document2 pagesLED-Face-Mask-Consultation-Form - 2Hanan AnsariNo ratings yet
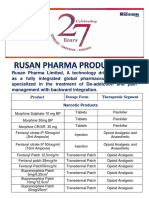
- Rusan Pharma Product ListDocument4 pagesRusan Pharma Product ListSanjay SharmaNo ratings yet
- Drug CompilationDocument39 pagesDrug CompilationANa AntonioNo ratings yet
- Modul-2 Pengobatan TBDocument180 pagesModul-2 Pengobatan TBJane BiringanNo ratings yet
- Bioavailability and BioequivalenceDocument28 pagesBioavailability and Bioequivalencekulbhushan singhNo ratings yet
- Daftar Obat Norum/Look Alike Sound AlikeDocument3 pagesDaftar Obat Norum/Look Alike Sound Alikewidia annisaNo ratings yet
- Morepen Laboratories Press Release Q1Document5 pagesMorepen Laboratories Press Release Q1gaurav chaudharyNo ratings yet
- General Dispensing ProcedureDocument1 pageGeneral Dispensing ProcedureHaroon RahimNo ratings yet
- 6 135Document6 pages6 135Ashok LenkaNo ratings yet
- Vadsp Human Product List 2021Document31 pagesVadsp Human Product List 2021Nirmal JainNo ratings yet
- Harga Promo BidanDocument31 pagesHarga Promo BidanDeden Arditia100% (1)
- Fall 2017FINALSyllabus Cottrell ALH 130Document8 pagesFall 2017FINALSyllabus Cottrell ALH 130vinhson65-1No ratings yet
- Anxiolytic Activity of Fennel Fruit Soxhlet in MiceDocument3 pagesAnxiolytic Activity of Fennel Fruit Soxhlet in MiceOthman JerbiNo ratings yet