You might also like
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Headache Disorders: Key FactsDocument1 pageHeadache Disorders: Key FactsJeremy EvansNo ratings yet
- Request for Determination of Possible Loss of U.S. NationalityDocument8 pagesRequest for Determination of Possible Loss of U.S. NationalityAfzal Imam100% (1)
- Case Week 5 Tutorial 1Document4 pagesCase Week 5 Tutorial 1Jeremy EvansNo ratings yet
- Week 2 Tropmed Tutorial 1-3Document8 pagesWeek 2 Tropmed Tutorial 1-3Jeremy EvansNo ratings yet
- Too Fast or Too Curious: A Confusing Case of Acute Myocardial Infarct or Vasospastic AnginaDocument1 pageToo Fast or Too Curious: A Confusing Case of Acute Myocardial Infarct or Vasospastic AnginaJeremy EvansNo ratings yet
- Carbohydrate digestion and glucose metabolism pathwaysDocument4 pagesCarbohydrate digestion and glucose metabolism pathwaysJeremy EvansNo ratings yet
- My Genius Is Almost Frightening Meme - Google SearchDocument1 pageMy Genius Is Almost Frightening Meme - Google SearchJeremy EvansNo ratings yet
- Fneur 12 636474Document9 pagesFneur 12 636474Jeremy EvansNo ratings yet
- MCQ MSK 2017Document12 pagesMCQ MSK 2017Jeremy EvansNo ratings yet
- Sclera Contains A ProteinDocument5 pagesSclera Contains A ProteinJeremy EvansNo ratings yet
- Developing & Testing: Davin, Darren, William, JuanDocument4 pagesDeveloping & Testing: Davin, Darren, William, JuanJeremy EvansNo ratings yet
- DinoDocument4 pagesDinoJeremy EvansNo ratings yet
- Differential Diagnoses for Pediatric Jaundice and Liver TestsDocument2 pagesDifferential Diagnoses for Pediatric Jaundice and Liver TestsJeremy EvansNo ratings yet
- Lesson 4: 1 Corinthians 12:27Document2 pagesLesson 4: 1 Corinthians 12:27Jeremy EvansNo ratings yet
- Lo Kidney Week 5Document10 pagesLo Kidney Week 5Jeremy EvansNo ratings yet
- Week 1 - Jeremy Evans Darmawan 01071180101Document12 pagesWeek 1 - Jeremy Evans Darmawan 01071180101Jeremy EvansNo ratings yet
- Laboratory Reference Ranges in Healthy AdultsDocument11 pagesLaboratory Reference Ranges in Healthy AdultsJeremy EvansNo ratings yet
- 10 Communications SoftwareDocument12 pages10 Communications SoftwareJeremy EvansNo ratings yet
- Laboratory Reference Ranges in Healthy AdultsDocument10 pagesLaboratory Reference Ranges in Healthy AdultsJeremy EvansNo ratings yet
- LO GalactosemiaDocument2 pagesLO GalactosemiaJeremy EvansNo ratings yet
- Alkanes MCQDocument2 pagesAlkanes MCQJeremy EvansNo ratings yet
- 7 Layer OSIDocument4 pages7 Layer OSIJeremy EvansNo ratings yet
- LO Trisomy 21Document4 pagesLO Trisomy 21Jeremy EvansNo ratings yet
- Physical Network TopologyDocument6 pagesPhysical Network TopologyJeremy EvansNo ratings yet
- ChromeDocument3 pagesChromeJeremy EvansNo ratings yet
- List of SpicesDocument8 pagesList of SpicesJeremy EvansNo ratings yet
- SumoDocument3 pagesSumoJeremy EvansNo ratings yet
- Fat Media Cooking MethodDocument3 pagesFat Media Cooking MethodJeremy EvansNo ratings yet
- ProtistsDocument3 pagesProtistsJeremy EvansNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- A Case Study In:: Hirschsprung DiseaseDocument18 pagesA Case Study In:: Hirschsprung DiseaseJaimie La PenaNo ratings yet
- Oral CandidiasisDocument4 pagesOral CandidiasisAnish RajNo ratings yet
- Daily Lesson Plan in English Grade 7 (Quarter 3-Module 5)Document2 pagesDaily Lesson Plan in English Grade 7 (Quarter 3-Module 5)Ramil60% (5)
- TB Management Final1Document23 pagesTB Management Final1Aanchal JainNo ratings yet
- Allergic RhinitisDocument27 pagesAllergic Rhinitispaningbatan.kristine.bNo ratings yet
- Thesis Statement About Drug UseDocument4 pagesThesis Statement About Drug Usepwqlnolkd100% (2)
- Antisense Drug TechnologyDocument12 pagesAntisense Drug TechnologyARAFAT MIAHNo ratings yet
- Aproach To Patient With FeverDocument61 pagesAproach To Patient With Feverfatima fatima92% (12)
- Pterygium - EyeWikiDocument1 pagePterygium - EyeWikiPaudel SujanNo ratings yet
- Med-Surg Exam #2 Study GuideDocument33 pagesMed-Surg Exam #2 Study GuideCaitlyn BilbaoNo ratings yet
- FDAR For Urinary Tract InfectionDocument2 pagesFDAR For Urinary Tract InfectionElle Monge100% (1)
- Lung Volumes and CapacitiesDocument16 pagesLung Volumes and CapacitiesMoses DumbuyaNo ratings yet
- Atrial FibrillationDocument28 pagesAtrial FibrillationKrisianne Mae Lorenzo FranciscoNo ratings yet
- Head Circumference For Age ChartDocument1 pageHead Circumference For Age ChartKaran TripathiNo ratings yet
- Kisi 2 B Ing - 230604 - 173816Document3 pagesKisi 2 B Ing - 230604 - 173816izzatul afifahNo ratings yet
- Instructors Manual 6th EditionDocument120 pagesInstructors Manual 6th EditionSean BokelmannNo ratings yet
- Pankaj Naram - CuresDocument14 pagesPankaj Naram - CuresArtlife1No ratings yet
- Uttaranchal PG College of Biomedical Sciences and HospitalDocument14 pagesUttaranchal PG College of Biomedical Sciences and HospitalpawanNo ratings yet
- Cell Injury, Cell Death, and Adaptations: Dr. I Made Naris Pujawan, M.Biomed, SP - PADocument27 pagesCell Injury, Cell Death, and Adaptations: Dr. I Made Naris Pujawan, M.Biomed, SP - PAlindaNo ratings yet
- DIAA0039-StigmaReport 17sp 20210711 PDFDocument28 pagesDIAA0039-StigmaReport 17sp 20210711 PDFIndranil PoddarNo ratings yet
- Pregnancy Induced Hypertension Case StudyDocument77 pagesPregnancy Induced Hypertension Case StudyATEHAN BORDS100% (1)
- Anesthetic Consideration For Patients With Obstructive JaundiceDocument47 pagesAnesthetic Consideration For Patients With Obstructive JaundiceagatakassaNo ratings yet
- @MBS MedicalBooksStore 2019 The PDFDocument394 pages@MBS MedicalBooksStore 2019 The PDFDsdentalNo ratings yet
- LEGIT 62 Ako 1RST Quarter Exam PDEV 111 1Document23 pagesLEGIT 62 Ako 1RST Quarter Exam PDEV 111 1Mylen Noel Elgincolin Manlapaz50% (2)
- Antibacterial Activity of Thaaleesaadhi Chooranam Against Human PathogensDocument8 pagesAntibacterial Activity of Thaaleesaadhi Chooranam Against Human PathogensRAJ KUMARNo ratings yet
- OsteopetrosisDocument13 pagesOsteopetrosisDeep SavaliaNo ratings yet
- Deworming of PetsDocument5 pagesDeworming of PetsRehan Ashraf BandeshaNo ratings yet
- Mann-Assessment-Of-Swallowing-Ability - Scoring SheetDocument1 pageMann-Assessment-Of-Swallowing-Ability - Scoring SheetThu TranNo ratings yet
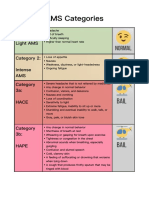
- AMS Symptoms and CategoriesDocument1 pageAMS Symptoms and CategoriesyyggvcNo ratings yet
- Therapeutic Monoclonal Antibodies Approved by FDA in 2019 (Mini Review)Document2 pagesTherapeutic Monoclonal Antibodies Approved by FDA in 2019 (Mini Review)asclepiuspdfsNo ratings yet