Professional Documents
Culture Documents
Nejmra022308 1
Uploaded by
Simón Pérez LópezOriginal Title
Copyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
Nejmra022308 1
Uploaded by
Simón Pérez LópezCopyright:
Available Formats
The new england journal of medicine
review article
mechanisms of disease
Epilepsy
Bernard S. Chang, M.D., and Daniel H. Lowenstein, M.D.
e pilepsy is one of the most common neurologic problems
worldwide. Approximately 2 million persons in the United States have epi-
lepsy, and 3 percent of persons in the general population will have epilepsy at
some point in their lives.1 In recent years, important advances have been made in the di-
agnosis and treatment of seizure disorders.2 However, our understanding of the cellu-
From the Comprehensive Epilepsy Center,
Department of Neurology, Beth Israel Dea-
coness Medical Center, and Harvard Med-
ical School — both in Boston (B.S.C.); and
the University of California San Francisco
Epilepsy Center, Department of Neurology,
University of California San Francisco, San
lar and molecular mechanisms by which epilepsy develops, or epileptogenesis, is still Francisco (D.H.L.).
incomplete.
In this overview, we highlight some of the prevailing ideas about epileptogenesis by N Engl J Med 2003;349:1257-66.
Copyright © 2003 Massachusetts Medical Society.
presenting examples of epilepsy syndromes and theories of their mechanisms of origin.
Several recent reviews offer more specialized and comprehensive discussions of this
topic.3-5
classification of epilepsy
The term “epilepsy” encompasses a number of different syndromes whose cardinal
feature is a predisposition to recurrent unprovoked seizures. Although specific seizures
can be classified according to their clinical features (e.g., complex partial seizures and
generalized tonic–clonic seizures),6 epilepsy syndromes can also be classified accord-
ing to the type of seizure, the presence or absence of neurologic or developmental ab-
normalities, and electroencephalographic (EEG) findings.7 For example, the syndrome
of juvenile myoclonic epilepsy is characterized by the onset of myoclonic seizures, gen-
eralized tonic–clonic seizures, and less frequently absence seizures in adolescents who
have normal intellectual function, with EEG findings of rapid, generalized spike-wave
and polyspike-wave discharges.8
Epilepsy syndromes fall into two broad categories: generalized and partial (or local-
ization-related) syndromes.7,8 In generalized epilepsies, the predominant type of sei-
zures begins simultaneously in both cerebral hemispheres. Many forms of generalized
epilepsy have a strong genetic component; in most, neurologic function is normal. In
partial epilepsies, by contrast, seizures originate in one or more localized foci, although
they can spread to involve the entire brain. Most partial epilepsies are believed to be the
result of one or more central nervous system insults, but in many cases the nature of the
insult is never identified.
mechanisms of generalized epilepsies
absence epilepsy
Childhood absence epilepsy is a generalized epilepsy syndrome that begins between
the ages of four and eight years with absence seizures and, more rarely, generalized ton-
ic–clonic seizures.9 During absence seizures, patients stare and cease normal activity
for a few seconds, then return immediately to normal and have no memory of the event.
Since these seizures can occur tens or hundreds of times a day, an incorrect diagnosis of
n engl j med 349;13 www.nejm.org september 25, 2003 1257
The New England Journal of Medicine
Downloaded from nejm.org on April 6, 2015. For personal use only. No other uses without permission.
Copyright © 2003 Massachusetts Medical Society. All rights reserved.
The new england journal of medicine
attention-deficit disorder or daydreaming is fre- dopaminergic inputs to the thalamus modulate this
quently made. There is a classic EEG pattern of three- circuit and affect the likelihood of a burst mode.23
per-second, generalized spike-wave discharges in In normal non-REM sleep, thalamic relay neu-
childhood absence epilepsy. rons in the burst mode activate the cortex in a rhyth-
For many years, the anatomical origin of absence mic, bilaterally synchronous way, creating visible
seizures and the accompanying EEG pattern were EEG patterns, such as sleep spindles.19 This “sleep
debated. The results of some experiments support- state” of the thalamocortical circuit is in contrast to
ed the hypothesis that absence seizures originated the normal “awake state,” in which the thalamic re-
in the thalamus. For example, electrical stimulation lay neurons are firing in the tonic mode and thal-
of the thalamus in cats produced bilaterally synchro- amocortical projections are transferring sensory in-
nous EEG discharges that resembled the classic ab- formation to the cortex in a nonrhythmic manner.
sence pattern.10 Also, recordings from electrodes In absence epilepsy, the abnormal circuit causes
implanted in the thalamus of a child with absence rhythmic activation of the cortex (typical of normal
epilepsy demonstrated three-per-second EEG dis- non-REM sleep) during wakefulness, which results
charges during typical seizures.11 Other work, how- in the characteristic EEG discharges and clinical
ever, suggested that the cerebral cortex itself was manifestations of an absence seizure.15 The precise
the primary origin of these seizures. For example, abnormality of the circuit has yet to be determined,
similar EEG discharges could be produced by ap- but there are multiple possibilities. Some data sug-
plying proconvulsant agents to the cortical surface gest that the T-type calcium channels may be the pri-
bilaterally.12 mary culprits.24,25 Other work has emphasized the
The mechanism that generates absence seizures importance of altered g-aminobutyric acid (GABA)
is now believed to involve an alteration in the cir- receptor function.26 A combination of factors may
cuitry between the thalamus and the cerebral cortex be involved, including changes in modulatory in-
(Fig. 1).13-15 Much has been learned from in vivo put from the brain stem.23 The overriding concept,
and in vitro electrophysiological recordings in an- however, is that dysfunction of a neuronal circuit
imal models of absence epilepsy, both those that that produces a physiologic state of rhythmic corti-
were experimentally induced and those that were cal activation (sleep) can lead to abnormal paroxys-
genetically determined.16-18 These and other stud- mal episodes of rhythmic cortical activation (absence
ies have shown that thalamocortical circuits gov- seizures).
ern the rhythm of cortical excitation by the thala- This concept helps explain the unique pharma-
mus and underlie normal physiologic patterns such cologic treatment of absence epilepsy. Ethosuxim-
as those that occur during sleep.19 Three neuronal ide, a drug that suppresses absence seizures but
populations are involved in this circuitry: thalamic not other types of seizures, appears to work by caus-
relay neurons, thalamic reticular neurons, and corti- ing voltage-dependent blockade of T-type calcium
cal pyramidal neurons. The thalamic relay neurons currents.27 This mechanism, as might be expect-
can activate the cortical pyramidal neurons either ed, is believed to inhibit the burst mode of thalamic-
in a tonic mode, which occurs during wakefulness relay-neuron firing. Valproic acid, an antiepileptic
and rapid-eye-movement (REM) sleep, or in a burst drug used for absence seizures and other types of
mode, which occurs during non-REM sleep. The seizures, also acts on the T-type calcium channels,
burst mode is made possible by T-type calcium as well as other substrates.28 Benzodiazepines that
channels, which allow for low-threshold depolar- activate an inhibitory GABAA receptor subtype on
izations on which bursts of action potentials (medi- thalamic reticular neurons can also be effective in
ated by voltage-gated sodium channels) are super- suppressing absence seizures (although other types
imposed.20 The mode of thalamocortical activation of benzodiazepines can worsen them).29 Baclofen,
— tonic or burst — is controlled largely by input an agonist of a GABA-receptor subtype that hy-
from the thalamic reticular neurons, which hyper- perpolarizes thalamic relay neurons and makes the
polarize the relay neurons, allowing them to fire in burst mode more likely, clearly exacerbates EEG
bursts.21 The reticular neurons can themselves be spike-wave discharges in animal models.30
inhibited through recurrent collaterals from neigh-
boring reticular neurons.22 Both cortical pyramidal generalized epilepsies associated
neurons and thalamic relay neurons project to the with ion-channel mutations
reticular neurons to complete the circuitry. In ad- Although most generalized epilepsies have com-
dition, ascending noradrenergic, serotonergic, and plex inheritance patterns, a few have a mendelian
1258 n engl j med 349;13 www.nejm.org september 25 , 2003
The New England Journal of Medicine
Downloaded from nejm.org on April 6, 2015. For personal use only. No other uses without permission.
Copyright © 2003 Massachusetts Medical Society. All rights reserved.
mechanisms of disease
A + B
EEG Patterns
Wakefulness
+
– + Desynchronized
– T-type Ca++
channel
– GABAB
+ Non-REM sleep
–
GABAA Thalamic relay
Spindles
Norepinephrine,
dopamine,
and serotonin
Absence seizure
Brain stem 3-per-second
spike wave
Figure 1. The Normal Thalamocortical Circuit and EEG Patterns during Wakefulness, Non–Rapid-Eye-Movement
(Non-REM) Sleep, and Absence Seizures.
Panel A shows the normal thalamocortical circuit. Thalamic relay neurons can activate the cortical pyramidal neurons in
either a tonic mode or a burst mode, the latter made possible by T-type calcium channels. The mode of thalamocortical
activation is controlled largely by input from the thalamic reticular neurons, which hyperpolarize the relay neurons through
g-aminobutyric acid type B (GABAB) receptors and are themselves inhibited by neighboring reticular neurons through
activation of GABA type A (GABAA) receptors. Cortical pyramidal neurons activate the thalamic reticular neurons in a
feed-forward loop. Ascending noradrenergic, serotonergic, and dopaminergic inputs from brain-stem structures appear
to modulate this circuit.
Panel B shows EEG patterns of wakefulness, non-REM sleep, and absence seizures. During wakefulness, the cortex is ac-
tivated by the thalamus in a tonic mode, allowing for processing of external sensory inputs. This results in a desynchro-
nized appearance of the EEG. During non-REM sleep, the cortex is activated in a burst mode, resulting in the EEG ap-
pearance of rhythmic sleep spindles. During an absence seizure, the normal thalamocortical circuit becomes dysfunctional,
allowing burst activation of the cortex to occur during wakefulness, which results in the EEG appearance of rhythmic
spike-wave discharges and interrupts responsiveness to external stimuli.
inheritance pattern and are associated with single- tation in the gene for the voltage-gated sodium
gene mutations (Table 1).42-44 Almost all these mu- channel b1 subunit (SCN1B), which modifies the
tations have been found in genes encoding ion- gating and inactivation properties of the channel.31
channel proteins (Fig. 2). Functional studies of the The mutant channel protein, when expressed in oo-
mutant channels have revealed potential mecha- cytes of the frog genus xenopus, allows passage of
nisms for some of these disorders. an increased sodium current. In neurons, the muta-
For example, “generalized epilepsy with febrile tion promotes depolarization and neuronal hyper-
seizures plus” is a genetic syndrome consisting of excitability. Since generalized epilepsy with febrile
febrile seizures plus at least one other type of seizure seizures plus was initially described, phenotypically
(absence, myoclonic, atonic, or afebrile generalized similar families have been identified with mutations
tonic–clonic seizures).45 Pedigree analysis has sug- in sodium channel subunits SCN1A and SCN2A and
gested that the inheritance pattern is autosomal the GABAA receptor subunit, GABRG2.32-34
dominant with incomplete penetrance and linkage Another generalized epilepsy syndrome, benign
to chromosome 19q. In this disorder, there is a mu- familial neonatal convulsions, has also been linked
n engl j med 349;13 www.nejm.org september 25, 2003 1259
The New England Journal of Medicine
Downloaded from nejm.org on April 6, 2015. For personal use only. No other uses without permission.
Copyright © 2003 Massachusetts Medical Society. All rights reserved.
The new england journal of medicine
Table 1. Epilepsy Syndromes Associated with Single-Gene Mutations.
Epilepsy Syndrome Gene Gene Product* Study
Generalized epilepsy with febrile seizures plus SCN1B Sodium-channel subunit Wallace et al.31
SCN1A Sodium-channel subunit Escayg et al.32
SCN2A Sodium-channel subunit Sugawara et al.33
GABRG2 GABAA-receptor subunit Baulac et al.34
Benign familial neonatal convulsions KCNQ2 Potassium channel Biervert et al.,35
Singh et al.36
KCNQ3 Potassium channel Charlier et al.37
Autosomal dominant nocturnal frontal-lobe CHRNA4 Neuronal nicotinic acetylcholine– Steinlein et al.38
epilepsy receptor subunit
CHRNB2 Neuronal nicotinic acetylcholine– Fusco et al.39
receptor subunit
Childhood absence epilepsy and febrile seizures GABRG2 GABAA-receptor subunit Wallace et al.40
Autosomal dominant partial epilepsy LGI1 Leucine-rich transmembrane Kalachikov et al.41
with auditory features protein
*GABAA denotes g-aminobutyric acid type A.
to single-gene mutations. In this autosomal dom- zure syndrome.48,49 These reports raise the prospect
inant disorder, seizures that are not associated that calcium-channel mutations will be found in
with neurologic or metabolic abnormalities begin pure epilepsy syndromes and emphasize the possi-
in the first few days of life and usually remit with- bility that various paroxysmal neurologic disorders
in a few weeks, with or without treatment.46 Mu- share common underlying mechanisms.
tations have been identified in KCNQ2 and KCNQ3,
the genes for potassium channels on chromosomes unanswered questions
20q and 8q.35-37 Functional studies have shown that Our understanding of generalized epileptogene-
the mutant channels allow passage of significantly sis remains far from complete. Why, for example,
less potassium current than wild-type channels.35 do persistent alterations in neuronal circuits or ex-
Since potassium currents are the primary force be- citability result in a paroxysmal disorder such as
hind repolarization of the neuronal membrane after epilepsy? A better understanding of the molecular
depolarization, these mutations would be expected and cellular circumstances that predispose a per-
to prolong depolarization, thereby increasing neu- son to a seizure at a particular time could have im-
ronal hyperexcitability. plications for the prevention of seizures. It is also
In these pure epilepsy syndromes, then, muta- unclear why many seizure syndromes have an age-
tions in genes encoding ion-channel proteins lead dependent onset and why some remit spontane-
to hyperexcitability of cortical neurons through al- ously. These features suggest that developmental
terations in channel function. Since these genes changes in the nervous system have an important
are expressed throughout the brain, it is plausible role in the clinical expression of generalized epi-
that the effect of the mutations is diffuse and there- lepsy syndromes that are genetically determined.50
fore confers a predisposition to a generalized sei-
zure disorder. Similar ion-channel mutations have
mechanisms of
been identified in a variety of disorders now termed partial epilepsies
“channelopathies.” These conditions, which are
characterized by paroxysmal episodes of neurologic mesial temporal-lobe epilepsy
or cardiac dysfunction, include episodic ataxia, pe- We know much less about the mechanisms un-
riodic paralysis, familial hemiplegic migraine, and derlying partial-seizure disorders than we do about
the long-QT syndrome.47 Two recent reports de- generalized epileptogenesis, even though partial
scribe calcium-channel mutations in patients with seizures are the most common seizure disorder in
a combination of episodic ataxia and a mixed-sei- adults, often stemming from focal lesions such as
1260 n engl j med 349;13 www.nejm.org september 25 , 2003
The New England Journal of Medicine
Downloaded from nejm.org on April 6, 2015. For personal use only. No other uses without permission.
Copyright © 2003 Massachusetts Medical Society. All rights reserved.
mechanisms of disease
A B C
Normal ion-channel Mutation in SCN1B Mutation in KCNQ2, KCNQ3
function (generalized epilepsy with (benign familial neonatal
febrile seizures plus) convulsions)
Na+ Na+ Na+
K+ K+ K+
Na+ Na+ Na+
K+ K+ K+
0 mV 0 mV 0 mV
¡90 mV ¡90 mV ¡90 mV
1 sec
Figure 2. Examples of Ion-Channel Dysfunction Associated with Inherited Forms of Epilepsy.
Panel A shows normal neuronal-ion-channel function and the action potential. Sodium and potassium channels are re-
sponsible for the primary components of the action potential, which involve a depolarizing phase mediated by sodium-
channel opening and a repolarizing phase due to potassium-channel opening and sodium-channel inactivation. Other
potassium channels contribute to a longer-term repolarization that helps prevent repetitive firing of the neuron.
Mutations in SCN1B, which encodes a voltage-gated sodium-channel subunit, are associated with generalized epilepsy with
febrile seizures plus (Panel B). The apparent effect of these mutations is to allow passage of an increased sodium current,
which would lead to a greater depolarization during the action potential and an increased tendency to fire repetitive bursts.
Mutations in KCNQ2 and KCNQ3, which both encode potassium channels, are associated with benign familial neonatal
convulsions (Panel C). These mutations, which appear to decrease the potassium outflow underlying the longer-lasting
“M current,” are likely to cause a loss of spike-firing adaptation and therefore an increase in neuronal firing frequency.
head trauma, strokes, and tumors.1 The most prev- dentate hilus and the hippocampal pyramidal-cell
alent of these syndromes features complex partial layer, with relative preservation of dentate granule
seizures arising from the mesial temporal lobe.8,51 cells and a small zone of pyramidal cells (in the cor-
Recordings from intracranial depth electrodes have nu ammonis, field 2, of the hippocampus). The
clearly demonstrated an ictal onset in mesial tempo- dense gliosis that accompanies the loss of neurons
ral structures such as the hippocampus, amygdala, causes shrinkage and hardening of tissue. The term
and adjacent parahippocampal cortex; surgical re- “mesial temporal sclerosis” has also been used for
section of these areas in suitable patients usually this lesion, because often there is neuronal loss in
abolishes the seizures.52 These seizures can begin the neighboring entorhinal cortex and amygdala.57
with olfactory or gustatory hallucinations, an epi- There is a vigorous debate about whether hip-
gastric sensation, or psychic symptoms such as déjà pocampal sclerosis is a cause or an effect of sei-
vu or depersonalization. Once the seizures progress zures.58,59 It has been seen in a wide variety of
to a loss of awareness, the patients may stare blank- epileptic conditions, including cryptogenic tempo-
ly, speak unintelligibly, or exhibit lip smacking, pick- ral-lobe epilepsy60 and epilepsy that follows fe-
ing at clothing, or other automatisms.53 brile seizures or other brain insults early in life,61 as
The most common lesion in surgically resected well as in animal models of head injury62 and sei-
tissue from patients with mesial temporal-lobe epi- zures induced by chemicals.63 It is possible that
lepsy is hippocampal sclerosis, a well-described en- hippocampal sclerosis represents a pathologic final
tity whose cause remains elusive.54-56 In hippocam- common pathway to partial epilepsy from a num-
pal sclerosis, there is selective loss of neurons in the ber of different causes.
n engl j med 349;13 www.nejm.org september 25, 2003 1261
The New England Journal of Medicine
Downloaded from nejm.org on April 6, 2015. For personal use only. No other uses without permission.
Copyright © 2003 Massachusetts Medical Society. All rights reserved.
The new england journal of medicine
Detailed studies of the morphologic changes in excitability, the causative role of mossy-fiber sprout-
hippocampal sclerosis have led to several hypothe- ing in epileptogenesis is still largely speculative.
ses about the mechanism of epileptogenesis in this There is, for example, strong evidence that newly
condition (Fig. 3). The best-described change is the sprouted axons also form synapses on inhibitory in-
sprouting of mossy-fiber axons from dentate gran- terneurons as part of a feedback mechanism, rath-
ule cells.64 Normally, excitatory input to the hippo- er than simply increase excitation.69-71
campus comes directly to the hippocampal dentate Some investigators have suggested that the se-
granule cells from the neighboring entorhinal cor- lective vulnerability of certain neurons may be a
tex, whereas inhibitory input arises locally from in- mechanism of epileptogenesis in hippocampal
terneurons in the inner molecular layer. The den- sclerosis. In animal models, excitatory interneurons
tate granule cells sprout mossy-fiber axons, which located within the dentate gyrus, which normally
extend to pyramidal neurons as part of the hippo- activate inhibitory interneurons, appear to be selec-
campal output pathway. Normal dentate granule tively lost.72 Loss of these excitatory cells would
cells appear to be relatively resistant to hypersyn- be expected to impair the inhibitory feedback and
chronous activation and may actually serve to inhib- feed-forward mechanisms that act on dentate gran-
it the propagation of seizures from the entorhinal ule cells, resulting in hyperexcitability.73 This expla-
cortex.51 In hippocampal sclerosis, however, these nation is plausible, but the evidence that dentate
cells sprout mossy-fiber axons that are directed granule cells can project directly onto inhibitory in-
back into the inner molecular layer,60,65,66 possibly terneurons raises the possibility of a compensatory
because the neurons to which they usually extend mechanism. For these reasons, the implications
have been lost. There is some evidence that these of selective cell loss in the hippocampus, although
aberrant mossy fibers instigate a recurrent excita- highly suggestive of a mechanism of epileptogene-
tory circuit by forming synapses on the dendrites of sis, are still not completely understood.
neighboring dentate granule cells.67,68 Although An intriguing hypothesis lies in the phenome-
such a circuit is a plausible explanation for hyper- non of neurogenesis. Almost all neurons in the brain
CA1 pyramidal Perforant path input
Hippocampal cells Inhibitory
output + + + interneuron
Inhibitory
interneuron – + –
Sprouting
Dentate
granule cells
Excitatory + +
interneuron
Subiculum Dentate g
u tin
gyrus CA3 pyramidal
ro
cells
Perforant Sp
pathway Selectively
vulnerable
Entorhinal Neurogenesis
Mossy fibers to CA3
cortex
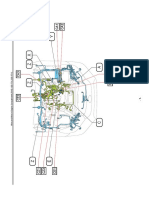
Figure 3. Hippocampal Sclerosis.
Hippocampal sclerosis is the most common identified pathological feature in cases of mesial temporal-lobe epilepsy. Normally, input to the hip-
pocampus comes from the entorhinal cortex to the dentate granule cells through the perforant path. Dentate granule cells project to the CA3 sec-
tor as the first step in the hippocampal output pathway. A close-up of the dentate granule-cell layer reveals several morphologic changes charac-
teristic of hippocampal sclerosis that may play a part in epileptogenesis. Newly sprouted mossy fibers from dentate granule cells can synapse on
dendrites of neighboring dentate granule cells, resulting in a recurrent excitatory circuit. They can also sprout onto inhibitory interneurons. Exci-
tation interneurons, which normally activate inhibitory interneurons, may be selectively vulnerable to brain insults. Finally, neurogenesis of new
dentate granule cells continues into adult life, and these neurons may integrate themselves into abnormal circuits.
1262 n engl j med 349;13 www.nejm.org september 25 , 2003
The New England Journal of Medicine
Downloaded from nejm.org on April 6, 2015. For personal use only. No other uses without permission.
Copyright © 2003 Massachusetts Medical Society. All rights reserved.
mechanisms of disease
are postmitotic and do not divide in adults, but pro- termined. Moreover, molecular alterations, such as
genitor cells in the dentate gyrus of the hippocam- changes in neurotransmitter receptors, are also like-
pus are known to divide. Postnatal neurogenesis in ly to be important. What this research indicates is
the hippocampus can occur throughout life.74 In that changes in local circuits are compatible with the
an animal model of temporal-lobe epilepsy induced development of focal hyperexcitability, which may
with the use of pilocarpine, seizures can trigger in- be the basis of some partial epilepsy syndromes.
creased mitotic activity in a proliferative area of
the dentate gyrus, resulting in the differentiation unanswered questions
of new dentate granule cells.75 This process may be Although studies of mesial temporal-lobe epilepsy
independent of mossy-fiber sprouting, which ap- have yielded useful information, there are other
pears to involve mature dentate granule cells rather plausible mechanisms of partial epileptogenesis
than newly differentiated ones.76 The functional that are not suggested by this syndrome. Some par-
significance of neuronal generation in the hippo- tial epilepsies, for example, are genetically deter-
campus after a brain insult is uncertain, although mined. Autosomal dominant nocturnal frontal-lobe
some evidence suggests that new dentate granule epilepsy, in which single-gene mutations have been
cells become abnormally integrated into neuronal identified, has turned out to be a channelopathy that
circuits.77 The potential clearly exists for an imbal- affects the neuronal nicotinic acetylcholine recep-
ance between excitation and inhibition as new neu- tor, which serves as a ligand-gated sodium chan-
rons differentiate and form synaptic connections. nel.38 Why mutations in this receptor, which is wide-
Since the genesis of dentate granule cells recapitu- ly expressed throughout the brain, should cause
lates similar processes early in the development of partial seizures in the frontal lobe is just one of many
the nervous system, this mechanism could be rele- mysteries. Some genetically determined partial ep-
vant to epileptogenesis both early and later in life. ilepsies, such as benign epilepsy with centrotempo-
In addition to these morphologic features, ral spikes (also called benign rolandic epilepsy), are
changes at the molecular level may also be impor- age-limited syndromes, suggesting the importance
tant. The most prominent of these are alterations of developmental influences.8,50,79 For many pa-
in the composition and expression of GABAA recep- tients with partial epilepsy, there may be an under-
tors on the surface of hippocampal dentate granule lying genetic predisposition that becomes manifest
cells. Normally, GABAA receptors in adults, which only after a sufficient environmental insult. Obvious-
consist of five subunits, serve as inhibitors, hyper- ly, understanding what molecular mechanisms are
polarizing the neuron by allowing passage of chlo- at work in patients with such a predisposition is of
ride ions when activated. In the pilocarpine model considerable clinical interest.
of temporal-lobe epilepsy, however, the expression
of various GABAA-receptor subunits in dentate gran- newer areas of research
ule cells is altered, and these altered receptors have
heightened sensitivity to zinc, which is abundant cortical malformations
in mossy-fiber terminals.78 Because this molecular A rapidly expanding area of investigation in epilep-
change precedes the onset of spontaneous seizures, togenesis is the study of malformations of cortical
it is a plausible mechanism of epileptogenesis. Such development, disorders in which the normal proc-
findings have implications for treatment, since var- ess of development in the cerebral cortex is disrupt-
ious anticonvulsant drugs act through the GABAA ed. These malformations range from microscopic
receptor. dysplasias to global abnormalities such as lissen-
In summary, hippocampal sclerosis, the most cephaly (smooth brain) or subcortical band het-
widely studied pathologic lesion underlying partial erotopia (double cortex)80 and can be classified as
epilepsy, has features of structural reorganization, disorders of neuronal proliferation, neuronal migra-
selective neuronal loss, and neurogenesis. The na- tion, or cortical organization.81 Many such malfor-
ture of these changes supports hypotheses that pre- mations are associated with refractory epilepsy and
dict the development of local hyperexcitability and a are increasingly recognized as a common cause of
predisposition to partial seizures. However, the actu- epilepsy that was previously believed to be crypto-
al contributions of these factors, if any, to the de- genic.82 In numerous cases, magnetic resonance
velopment of an epileptic state have not been de- imaging with high resolution has identified small
n engl j med 349;13 www.nejm.org september 25, 2003 1263
The New England Journal of Medicine
Downloaded from nejm.org on April 6, 2015. For personal use only. No other uses without permission.
Copyright © 2003 Massachusetts Medical Society. All rights reserved.
The new england journal of medicine
cortical malformations in patients without any
conclusions
other obvious causes of epilepsy.
Malformations of cortical architecture are useful Our aim in understanding how epilepsy develops
for investigating the cellular and network changes is to prevent it. Clinically, there is often a “silent in-
that underlie the development of epilepsy.82-84 Al- terval” between the occurrence of a neurologic in-
though work in this area is still in its infancy, recent sult and the appearance of recurrent seizures in
studies have provided us with a glimpse of what lies many acquired forms of epilepsy. In addition, most
ahead. For example, in an animal model of hippo- genetically determined epilepsy syndromes do not
campal heterotopias the heterotopic neurons lack become clinically manifest until well after birth.
a particular potassium channel that in normal hip- Both these facts suggest that epileptogenesis is a
pocampal neurons subserves a voltage-activated fast gradual process that can be specifically targeted.
potassium current.85 This defect would be expect- Ideally, we would like to have a drug that prevents
ed to lead to hyperexcitability. Other investigators the development of epilepsy, rather than one that
have shown in a rat model that neurons within dys- merely suppresses seizures. Unfortunately, none of
plastic areas have impaired GABA-mediated inhibi- the available anticonvulsant agents appear to have
tory synaptic transmission, another defect that could a prophylactic effect in patients who are at risk for
lead to a predisposition to seizures.86 the development of a seizure disorder.89
It is likely that generalized and partial epilepsy
the role of glial cells syndromes arise from different mechanisms. Cur-
Decades of research in epileptogenesis, including rent evidence suggests that generalized epilepsies
much of the work highlighted in this review, have originate from alterations in either neuronal net-
focused on the intrinsic properties and network works, as in absence seizures, or intrinsic neuronal
connections of neurons. Glial cells, although long function, as in channelopathies. Partial epilepsy syn-
considered to be merely supporting cells in the cen- dromes presumably stem from a focal lesion. Inten-
tral nervous system, may also have an important sive studies of hippocampal sclerosis, the most com-
role.87 Glia perform key buffering functions that mon pathological finding in adults with the most
help to maintain the uptake of potassium and common partial epilepsy, have demonstrated many
glutamate and other aspects of the extracellular local changes, but their causative role, if any, in epi-
milieu of neurons. Theoretically, disruption of these leptogenesis is still unknown. Newer avenues of
glial functions could cause neuronal hyperexcit- study (such as cortical malformations) and newer
ability, since increased levels of extracellular po- conceptual mechanisms (such as the role of glial
tassium decrease the threshold for neuronal fir- cells and the neuronal microenvironment) are like-
ing and increased levels of glutamate could increase ly to yield future insights into this complicated field.
neuronal activation. Preliminary evidence from an For now, however, while prevention is still elusive,
animal model of cortical malformation indicates our clinical goals must remain the treatment and
that astrocytes (a subtype of glia) near the dysplastic cure of epilepsy.
region have a profound reduction in inward po- Supported in part by a grant (NS39950) from the National Insti-
tassium currents.88 Thus, a change in the neuronal tutes of Health.
We are indebted to Drs. Scott Baraban, Edward Cooper, Donald
microenvironment may be another mechanism of Schomer, and Robert Sloviter for their useful suggestions and criti-
epileptogenesis. cal review.
refer enc es
1. Annegers JF. The epidemiology of epi- 5. Engelborghs S, D’Hooge R, De Deyn PP. 9. Panayiotopoulos CP. Absence epilep-
lepsy. In: Wyllie E, ed. The treatment of epi- Pathophysiology of epilepsy. Acta Neurol sies. In: Engel J Jr, Pedley TA, eds. Epilepsy:
lepsy: principles and practice. 3rd ed. Phila- Belg 2000;100:201-13. a comprehensive textbook. Philadelphia: Lip-
delphia: Lippincott Williams & Wilkins, 6. Commission on Classification and Ter- pincott-Raven, 1997:2327-46.
2001:131-8. minology of the International League against 10. Jasper HH, Droogleever-Fortuyn J. Exper-
2. Schachter SC. Epilepsy. Neurol Clin 2001; Epilepsy. Proposal for revised clinical and imental studies on the functional anatomy
19:57-78. electroencephalographic classification of epi- of petit mal epilepsy. Assoc Res Nerv Ment
3. Najm I, Ying Z, Janigro D. Mechanisms leptic seizures. Epilepsia 1981;22:489-501. Dis 1947;26:272-98.
of epileptogenesis. Neurol Clin 2001;19:237- 7. Idem. Proposal for revised classification 11. Williams D. A study of thalamic and cor-
50. of epilepsies and epileptic syndromes. Epi- tical rhythms in petit mal. Brain 1953;76:50-
4. Dalby NO, Mody I. The process of epi- lepsia 1989;30:389-99. 69.
leptogenesis: a pathophysiological approach. 8. Benbadis SR. Epileptic seizures and syn- 12. Marcus EM, Watson CW. Bilateral syn-
Curr Opin Neurol 2001;14:187-92. dromes. Neurol Clin 2001;19:251-70. chronous spike wave electrographic pat-
1264 n engl j med 349;13 www.nejm.org september 25, 2003
The New England Journal of Medicine
Downloaded from nejm.org on April 6, 2015. For personal use only. No other uses without permission.
Copyright © 2003 Massachusetts Medical Society. All rights reserved.
mechanisms of disease
terns in the cat. Arch Neurol 1966;14:601- 30. Hosford DA, Clark S, Cao Z, et al. The 47. Kullmann DM. The neuronal channelo-
10. role of GABAB receptor activation in absence pathies. Brain 2002;125:1177-95.
13. Snead OC III. Basic mechanisms of gen- seizures of lethargic (lh/lh) mice. Science 48. Escayg A, De Waard M, Lee DD, et al.
eralized absence seizures. Ann Neurol 1995; 1992;257:398-401. Coding and noncoding variation of the
37:146-57. 31. Wallace RH, Wang DW, Singh R, et al. human calcium-channel b4-subunit gene
14. Futatsugi Y, Riviello JJ Jr. Mechanisms of Febrile seizures and generalized epilepsy CACNB4 in patients with idiopathic gener-
generalized absence epilepsy. Brain Dev associated with a mutation in the Na+-chan- alized epilepsy and episodic ataxia. Am J
1998;20:75-9. nel b1 subunit gene SCN1B. Nat Genet 1998; Hum Genet 2000;66:1531-9.
15. Kostopoulos GK. Involvement of the 19:366-70. 49. Jouvenceau A, Eunson LH, Spauschus
thalamocortical system in epileptic loss of 32. Escayg A, MacDonald BT, Meisler MH, A, et al. Human epilepsy associated with dys-
consciousness. Epilepsia 2001;42:Suppl 3: et al. Mutations of SCN1A, encoding a neu- function of the brain P/Q-type calcium chan-
13-9. ronal sodium channel, in two families with nel. Lancet 2001;358:801-7.
16. Snead OC III. Pharmacological models GEFS+2. Nat Genet 2000;24:343-5. 50. Sanchez RM, Jensen FE. Maturational
of generalized absence seizures in rodents. 33. Sugawara T, Tsurubuchi Y, Agarwala aspects of epilepsy mechanisms and conse-
J Neural Transm Suppl 1992;35:7-19. KL, et al. A missense mutation of the Na+ quences for the immature brain. Epilepsia
17. Danober L, Deransart C, Depaulis A, channel alpha II subunit gene Na(v)1.2 in a 2001;42:577-85.
Vergnes M, Marescaux C. Pathophysiological patient with febrile and afebrile seizures 51. Engel J Jr. Mesial temporal lobe epi-
mechanisms of genetic absence epilepsy in causes channel dysfunction. Proc Natl Acad lepsy: what have we learned? Neuroscientist
the rat. Prog Neurobiol 1998;55:27-57. Sci U S A 2001;98:6384-9. 2001;7:340-52.
18. Coenen AM, Drinkenburg WH, Inoue 34. Baulac S, Huberfeld G, Gourfinkel-An I, 52. Kim R, Spencer D. Surgery for mesial
M, van Luijtelaar EL. Genetic models of et al. First genetic evidence of GABAA recep- temporal sclerosis. In: Lüders HO, Comair
absence epilepsy, with emphasis on the tor dysfunction in epilepsy: a mutation in the YG. Epilepsy surgery. 2nd ed. Philadelphia:
WAG/Rij strain of rats. Epilepsy Res 1992; g2-subunit gene. Nat Genet 2001;28:46-8. Lippincott Williams & Wilkins, 2001:643-
12:75-86. 35. Biervert C, Schroeder BC, Kubisch C, et 52.
19. Steriade M, McCormick DA, Sejnowski al. A potassium channel mutation in neona- 53. French JA, Williamson PD, Thadani VM,
TJ. Thalamocortical oscillations in the sleep- tal human epilepsy. Science 1998;279:403-6. et al. Characteristics of medial temporal
ing and aroused brain. Science 1993;262: 36. Singh NA, Charlier C, Stauffer D, et al. lobe epilepsy. I. Results of history and phys-
679-85. A novel potassium channel gene, KCNQ2, is ical examination. Ann Neurol 1993;34:774-
20. Nowycky MC, Fox AP, Tsien RW. Three mutated in an inherited epilepsy of new- 80.
types of neuronal calcium channel with dif- borns. Nat Genet 1998;18:25-9. 54. Mathern GW, Babb TL, Armstrong DL.
ferent calcium agonist sensitivity. Nature 37. Charlier C, Singh NA, Ryan SG, et al. Hippocampal sclerosis. In: Engel J Jr, Pedley
1985;316:440-3. A pore mutation in a novel KQT-like potas- TA, eds. Epilepsy: a comprehensive textbook.
21. Crunelli V, Leresche N. A role for GABAB sium channel gene in an idiopathic epilepsy Philadelphia: Lippincott-Raven, 1997:133-
receptors in excitation and inhibition of family. Nat Genet 1998;18:53-5. 55.
thalamocortical cells. Trends Neurosci 38. Steinlein OK, Mulley JC, Propping P, et 55. Blümcke I, Beck H, Lie AA, Wiestler OD.
1991;14:16-21. al. A missense mutation in the neuronal nic- Molecular neuropathology of human mesial
22. Bazhenov M, Timofeev I, Steriade M, otinic acetylcholine receptor alpha 4 subunit temporal lobe epilepsy. Epilepsy Res 1999;
Sejnowski TJ. Self-sustained rhythmic activ- is associated with autosomal dominant noc- 36:205-23.
ity in the thalamic reticular nucleus medi- turnal frontal lobe epilepsy. Nat Genet 1995; 56. Liu Z, Mikati M, Holmes GL. Mesial
ated by depolarizing GABAA receptor poten- 11:201-3. temporal sclerosis: pathogenesis and signifi-
tials. Nat Neurosci 1999;2:168-74. 39. Fusco MD, Becchetti A, Patrignani A, et cance. Pediatr Neurol 1995;12:5-16.
23. McCormick DA. Neurotransmitter al. The nicotinic receptor beta2 subunit is 57. Falconer MA, Taylor DC. Surgical treat-
actions in the thalamus and cerebral cortex mutant in nocturnal frontal lobe epilepsy. ment of drug-resistant epilepsy due to mesial
and their role in neuromodulation of thala- Nat Genet 2000;26:275-6. temporal sclerosis: etiology and significance.
mocortical activity. Prog Neurobiol 1992; 40. Wallace RH, Marini C, Petrou S, et al. Arch Neurol 1968;19:353-61.
39:337-88. Mutant GABAA receptor gamma2-subunit in 58. Berkovic SF, Jackson GD. The hippocam-
24. Kim D, Song I, Keum S, et al. Lack of the childhood absence epilepsy and febrile sei- pal sclerosis whodunit: enter the genes. Ann
burst firing of thalamocortical relay neurons zures. Nat Genet 2001;28:49-52. Neurol 2000;47:557-8.
and resistance to absence seizures in mice 41. Kalachikov S, Evgrafov O, Ross B, et al. 59. Jefferys JGR. Hippocampal sclerosis
lacking a1G T-type Ca2+ channels. Neuron Mutations in LGI1 cause autosomal-domi- and temporal lobe epilepsy: cause or conse-
2001;31:35-45. nant partial epilepsy with auditory features. quence? Brain 1999;122:1007-8.
25. Burgess DL, Noebels JL. Single gene Nat Genet 2002;30:335-41. 60. Sutula T, Cascino G, Cavazos J, Parada I,
defects in mice: the role of voltage-depend- 42. Berkovic SF, Scheffer IE. Genetics of the Ramirez L. Mossy fiber synaptic reorganiza-
ent calcium channels in absence models. epilepsies. Epilepsia 2001;42:Suppl 5:16-23. tion in the epileptic human temporal lobe.
Epilepsy Res 1999;36:111-22. 43. Stafstrom CE, Tempel BL. Epilepsy genes: Ann Neurol 1989;26:321-30.
26. Caddick SJ, Hosford DA. The role of the link between molecular dysfunction and 61. Mathern GW, Babb TL, Vickrey BG,
GABAB mechanisms in animal models of pathophysiology. Ment Retard Dev Disabil Melendez M, Pretorius JK. The clinical-patho-
absence seizures. Mol Neurobiol 1996;13: Res Rev 2000;6:281-92. genic mechanisms of hippocampal neuron
23-32. 44. Prasad AN, Prasad C, Stafstrom CE. loss and surgical outcomes in temporal lobe
27. Glauser TA. Ethosuximide. In: Wyllie E, Recent advances in the genetics of epilepsy: epilepsy. Brain 1995;118:105-18.
ed. The treatment of epilepsy: principles and insights from human and animal studies. 62. Lowenstein DH, Thomas MJ, Smith DH,
practice. 3rd ed. Philadelphia: Lippincott Wil- Epilepsia 1999;40:1329-52. McIntosh TK. Selective vulnerability of den-
liams & Wilkins, 2001:881-91. 45. Scheffer IE, Berkovic SF. Generalized tate hilar neurons following traumatic brain
28. Kwan P, Sills GJ, Brodie MJ. The mecha- epilepsy with febrile seizures plus: a genetic injury: a potential mechanistic link between
nisms of action of commonly used antiepi- disorder with heterogeneous clinical phe- head trauma and disorders of the hippo-
leptic drugs. Pharmacol Ther 2001;90:21-34. notypes. Brain 1997;120:479-90. campus. J Neurosci 1992;12:4846-53.
29. Panayiotopoulos CP. Typical absence 46. Mizrahi EM. Neonatal seizures and neo- 63. Liu Z, Nagao T, Desjardins CG, Gloor P,
seizures and their treatment. Arch Dis Child natal epileptic syndromes. Neurol Clin 2001; Avoli M. Quantitative evaluation of neuronal
1999;81:351-5. 19:427-63. loss in the dorsal hippocampus in rats with
n engl j med 349;13 www.nejm.org september 25, 2003 1265
The New England Journal of Medicine
Downloaded from nejm.org on April 6, 2015. For personal use only. No other uses without permission.
Copyright © 2003 Massachusetts Medical Society. All rights reserved.
mechanisms of disease
long-term pilocarpine seizures. Epilepsy Res 72. Idem. Decreased hippocampal inhibition the human cerebral cortex. Neuron 1999;
1994;17:237-47. and a selective loss of interneurons in exper- 23:19-29.
64. Parent JM, Lowenstein DH. Mossy fiber imental epilepsy. Science 1987;235:73-6. 81. Barkovich AJ, Kuzniecky RI, Jackson
reorganization in the epileptic hippocam- 73. Idem. Permanently altered hippocampal GD, Guerrini R, Dobyns WB. Classification
pus. Curr Opin Neurol 1997;10:103-9. structure, excitability, and inhibition after system for malformations of cortical devel-
65. Tauck D, Nadler J. Evidence of functional experimental status epilepticus in the rat: the opment: update 2001. Neurology 2001;57:
mossy fiber sprouting in hippocampal for- “dormant basket cell” hypothesis and its pos- 2168-78.
mation of kainic acid-treated rats. J Neurosci sible relevance to temporal lobe epilepsy. 82. Schwartzkroin PA, Walsh CA. Cortical
1985;5:1016-22. Hippocampus 1991;1:41-66. malformations and epilepsy. Ment Retard
66. Babb TL, Kupfer WR, Pretorious JK, 74. Eriksson PS, Perfilieva E, Bjork-Eriks- Dev Disabil Res Rev 2000;6:268-80.
Crandall PH, Levesque MF. Synaptic reor- son T, et al. Neurogenesis in the adult human 83. Jacobs KM, Kharazia VN, Prince DA.
ganization by mossy fibers in human epilep- hippocampus. Nat Med 1998;4:1313-7. Mechanisms underlying epileptogenesis in
tic fascia dentata. Neuroscience 1991;42: 75. Parent JM, Yu TW, Leibowitz RT, Gesch- cortical malformations. Epilepsy Res 1999;
351-63. wind DH, Sloviter RS, Lowenstein DH. Den- 36:165-88.
67. Okazaki MM, Evenson DA, Nadler JV. tate granule cell neurogenesis is increased 84. Andermann F. Cortical dysplasias and
Hippocampal mossy fiber sprouting and by seizures and contributes to aberrant net- epilepsy: a review of the architectonic, clini-
synapse formation after status epilepticus in work reorganization in the adult rat hippo- cal, and seizure patterns. Adv Neurol 2000;
rats: visualization after retrograde transport campus. J Neurosci 1997;17:3727-38. 84:479-96.
of biocytin. J Comp Neurol 1995;352:515- 76. Parent JM, Tada E, Fike JR, Lowenstein 85. Castro PA, Cooper EC, Lowenstein DH,
34. DH. Inhibition of dentate granule cell neu- Baraban SC. Hippocampal heterotopia lack
68. Wuarin J, Dudek FE. Electrographic sei- rogenesis with brain irradiation does not functional Kv4.2 potassium channels in the
zures and new recurrent excitatory circuits prevent seizure-induced mossy fiber synap- methylazoxymethanol model of cortical mal-
in the dentate gyrus of hippocampal slices tic reorganization in the rat. J Neurosci formations and epilepsy. J Neurosci 2001;
from kainate-treated epileptic rats. J Neuro- 1999;19:4508-19. 21:6626-34.
sci 1996;16:4438-48. 77. Scharfman HE, Goodman JH, Sollas 86. Zhu WJ, Roper SN. Reduced inhibition
69. Ribak CE, Peterson GM. Intragranular AL. Granule-like neurons at the hilar/CA3 in an animal model of cortical dysplasia.
mossy fibers in rats and gerbils form syn- border after status epilepticus and their syn- J Neurosci 2000;20:8925-31.
apses with the somata and proximal den- chrony with area CA3 pyramidal cells: func- 87. Delgado-Escueta AV. Introduction: glia
drites of basket cells in the dentate gyrus. tional implications of seizure-induced neu- and epilepsy. Adv Neurol 1999;79:561-4.
Hippocampus 1991;1:355-64. rogenesis. J Neurosci 2000;20:6144-58. 88. Bordey A, Lyons SA, Hablitz JJ, Sonthei-
70. Kneisler TB, Dingledine R. Spontaneous 78. Brooks-Kayal AR, Shumate MD, Jin H, mer H. Electrophysiological characteristics
and synaptic input from granule cells and Rikhter TY, Coulter DA. Selective changes in of reactive astrocytes in experimental cortical
the perforant path to dentate basket cells in single cell GABAA receptor expression and dysplasia. J Neurophysiol 2001;85:1719-31.
the rat hippocampus. Hippocampus 1995;5: function in temporal lobe epilepsy. Nat Med 89. Temkin NR. Antiepileptogenesis and
151-64. 1998;4:1166-72. seizure prevention trials with antiepileptic
71. Sloviter RS. Possible functional conse- 79. Ottman R. Progress in the genetics of drugs: meta-analysis of controlled trials.
quences of synaptic reorganization in the the partial epilepsies. Epilepsia 2001;42: Epilepsia 2001;42:515-24.
dentate gyrus of kainate-treated rats. Neuro- Suppl 5:24-30. Copyright © 2003 Massachusetts Medical Society.
sci Lett 1992;137:91-6. 80. Walsh CA. Genetic malformations of
journal index
The index to volume 347 of the Journal will be available on February 20, 2003. At
that time, it can be ordered in a printed and bound format or can be downloaded
from www.nejm.org. To order a bound copy, please call 1-800-217-7874 from the
United States and Canada (call 651-582-3800 from other countries, or e-mail info@
reprintservices.com).
1266 n engl j med 349;13 www.nejm.org september 25, 2003
The New England Journal of Medicine
Downloaded from nejm.org on April 6, 2015. For personal use only. No other uses without permission.
Copyright © 2003 Massachusetts Medical Society. All rights reserved.
You might also like
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5795)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Section Properties Torsional Constant Area of SectionDocument38 pagesSection Properties Torsional Constant Area of SectionAlma M. LaraNo ratings yet
- Anterior Posterior HippocampusDocument25 pagesAnterior Posterior HippocampusChrysoula GkaniNo ratings yet
- Neuroimaging Self Assessment Colour ReviewDocument228 pagesNeuroimaging Self Assessment Colour ReviewHamza Arjah100% (1)
- The Limbic Brain. Andrew Lautin PDFDocument152 pagesThe Limbic Brain. Andrew Lautin PDFAntonio D LazodelaVegaNo ratings yet
- Hippocampus: Jump To Navigation Jump To Search Seahorse Hippocampus (Mythology) Hippocampus (Disambiguation)Document21 pagesHippocampus: Jump To Navigation Jump To Search Seahorse Hippocampus (Mythology) Hippocampus (Disambiguation)Lakshmi NarayananNo ratings yet
- 10.1007/978 3 662 03628 0Document213 pages10.1007/978 3 662 03628 0bvnice100% (1)
- Specialized Astrocytes Mediate Glutamatergic Gliotransmission in The CNSDocument47 pagesSpecialized Astrocytes Mediate Glutamatergic Gliotransmission in The CNSCARDIO 2019No ratings yet
- Probability CalculatorDocument104 pagesProbability CalculatorNorlly Mohd IsaNo ratings yet
- AMM 64 S1 WebDocument176 pagesAMM 64 S1 WebAndrada CatrinoiuNo ratings yet
- InterneuronsDocument6 pagesInterneuronsRafu DestajoNo ratings yet
- Fixed Stage Upright MicroscopeDocument14 pagesFixed Stage Upright MicroscopeAmy AdamsNo ratings yet
- Schema Ketronx1Document12 pagesSchema Ketronx1Manrolla89% (9)
- EN0937USDocument16 pagesEN0937USSaravanan MathiNo ratings yet
- Master Thesis ProposalDocument8 pagesMaster Thesis ProposalEvaNo ratings yet
- 14 GMD - Cycloconverter Control TerminalDocument15 pages14 GMD - Cycloconverter Control TerminalIrving Dirzo Carrillo100% (1)
- Diencephalon, Basal Ganglia, Limbic SystemDocument56 pagesDiencephalon, Basal Ganglia, Limbic SystemJoaquin GuillermoNo ratings yet
- Braak & Braak - 1991 - Neuropathological Stageing of Alzheimer-Related ChangesDocument21 pagesBraak & Braak - 1991 - Neuropathological Stageing of Alzheimer-Related ChangesLuis ÓnidasNo ratings yet
- (Developmental Neuroscience) Anthony T. Campagnoni-Brain Development With A Focus On The Cortex - Developmental Neuroscience Vol 25 Issue 2-4-S Karger Pub (2003) PDFDocument215 pages(Developmental Neuroscience) Anthony T. Campagnoni-Brain Development With A Focus On The Cortex - Developmental Neuroscience Vol 25 Issue 2-4-S Karger Pub (2003) PDFFrancisco DiezNo ratings yet
- Yamaha PSR 640 PSR 740Document79 pagesYamaha PSR 640 PSR 740pigulus0% (2)
- Memory Dysfunction.9Document14 pagesMemory Dysfunction.9Luis Antonio Cespedes HernandezNo ratings yet
- The Limbic System: Behavior Aggression Emotion Sexual Response Phylogenetically AncientDocument22 pagesThe Limbic System: Behavior Aggression Emotion Sexual Response Phylogenetically AncientNaveed AkhterNo ratings yet
- 1 s2.0 S0891061819301024 MainDocument10 pages1 s2.0 S0891061819301024 MainRenato Guerra GonzalezNo ratings yet
- TMP 5 F7 CDocument10 pagesTMP 5 F7 CFrontiersNo ratings yet
- Location - Routing Engine Compartment Wire and Wire (RHD 1GD-FTV, 2GD-FTV)Document2 pagesLocation - Routing Engine Compartment Wire and Wire (RHD 1GD-FTV, 2GD-FTV)Anibal Fabian GonzalezNo ratings yet
- Si Nap To GenesisDocument6 pagesSi Nap To GenesisEleazar ArcticIceNo ratings yet
- Physiology of Memory and LearningDocument48 pagesPhysiology of Memory and LearningWahyoe PoeshNo ratings yet
- Paraphilias As A Sub Type of Obsessive-Compulsive Disorder: A Hypothetical Bio-Social ModelDocument14 pagesParaphilias As A Sub Type of Obsessive-Compulsive Disorder: A Hypothetical Bio-Social ModelmuiNo ratings yet
- Resveratrol Therapy For EpilepsyDocument37 pagesResveratrol Therapy For EpilepsyAlejandro Nico Rondón OrtizNo ratings yet
- Brain Regions With Definitions - NeuroLexDocument32 pagesBrain Regions With Definitions - NeuroLexSrinivas RajanalaNo ratings yet