You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5796)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Faster and Cheaper - How Ride-Sourcing Fills A Gap in Low-Income Los Angeles NeighborhoodsDocument29 pagesFaster and Cheaper - How Ride-Sourcing Fills A Gap in Low-Income Los Angeles NeighborhoodsSam StecklowNo ratings yet
- Hadoop Course Content PDFDocument9 pagesHadoop Course Content PDFNaveen ElancersoftNo ratings yet
- Suction Pile and FoundationDocument19 pagesSuction Pile and FoundationhaydarburedahNo ratings yet
- What Is Moral Reasoning?: Digital Commons at SPUDocument34 pagesWhat Is Moral Reasoning?: Digital Commons at SPUMiftahul FirdausNo ratings yet
- I. Currency Futures Contract 1. Definition of Currency Futures ContractDocument12 pagesI. Currency Futures Contract 1. Definition of Currency Futures ContractMiftahul FirdausNo ratings yet
- Managing Transaction Exposure: Keywords: Foreign Exchange Exposure, Currency Risk, Hedging. JEL Codes: G30, F31Document9 pagesManaging Transaction Exposure: Keywords: Foreign Exchange Exposure, Currency Risk, Hedging. JEL Codes: G30, F31Miftahul FirdausNo ratings yet
- International Financial Management: - An Introduction To Multinational FinanceDocument3 pagesInternational Financial Management: - An Introduction To Multinational FinanceMiftahul FirdausNo ratings yet
- Family Business and Transaction Exposure: Khalil Nimer, Mahmoud Nassar, Naser Abu Ghazaleh and Abdulhadi RamadanDocument22 pagesFamily Business and Transaction Exposure: Khalil Nimer, Mahmoud Nassar, Naser Abu Ghazaleh and Abdulhadi RamadanMiftahul FirdausNo ratings yet
- It Is Generally Not Possible To Completely Eliminate Both Translation Exposure and Transaction ExposDocument1 pageIt Is Generally Not Possible To Completely Eliminate Both Translation Exposure and Transaction ExposMiftahul FirdausNo ratings yet
- Netflix Case QuestionsDocument8 pagesNetflix Case QuestionsMiftahul FirdausNo ratings yet
- Working Capital Management: Answers To End-Of-Chapter QuestionsDocument27 pagesWorking Capital Management: Answers To End-Of-Chapter QuestionsMiftahul FirdausNo ratings yet
- The Cost of Capital: Answers To End-Of-Chapter QuestionsDocument21 pagesThe Cost of Capital: Answers To End-Of-Chapter QuestionsMiftahul FirdausNo ratings yet
- Can Female CEOS of Multinational Companies Play A Role in Improving Both Organizational Practives and InnovationDocument14 pagesCan Female CEOS of Multinational Companies Play A Role in Improving Both Organizational Practives and InnovationMiftahul FirdausNo ratings yet
- Strategic Cost ManagementDocument12 pagesStrategic Cost ManagementvionysusgoghNo ratings yet
- Mvo 1965Document113 pagesMvo 1965younisNo ratings yet
- Cut Pieces: From Flat Plates, Strips and Coil Stock. A. Shearing B. Bend Allowance C. Forming Dies D. Spring BackDocument100 pagesCut Pieces: From Flat Plates, Strips and Coil Stock. A. Shearing B. Bend Allowance C. Forming Dies D. Spring BackJade DigNo ratings yet
- Special Theory of RelativityDocument16 pagesSpecial Theory of RelativityBrigita SteffyNo ratings yet
- The Lateral Trochanteric Wall Gotfried 2004 PDFDocument5 pagesThe Lateral Trochanteric Wall Gotfried 2004 PDFluis perezNo ratings yet
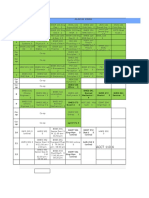
- BSMS Drexel ScheduleDocument4 pagesBSMS Drexel ScheduleAmy ZhiNo ratings yet
- Sample For Solution Manual Theory and Design For Mechanical Measurements 6th Edition by Figliola & BeasleyDocument30 pagesSample For Solution Manual Theory and Design For Mechanical Measurements 6th Edition by Figliola & BeasleyM.R.ZNo ratings yet
- IndraneelRakshit ResumeDocument7 pagesIndraneelRakshit ResumeIndraneel RakshitNo ratings yet
- NCERT Exemplar Class 8 Maths Solutions Chapter 3 Square-Square Root & Cube-Cube RootDocument77 pagesNCERT Exemplar Class 8 Maths Solutions Chapter 3 Square-Square Root & Cube-Cube Rootdeep34No ratings yet
- Alxion: For Direct DriveDocument56 pagesAlxion: For Direct DriveAnselmo Aguado cortesNo ratings yet
- BED SyallabusDocument32 pagesBED Syallabushp4cool9660No ratings yet
- 21 Day Fix Food ListDocument1 page21 Day Fix Food Listjavi martinezNo ratings yet
- Web 24 - Teti Madiadipoera - Treatment and Management of Rhinitis AllergyDocument38 pagesWeb 24 - Teti Madiadipoera - Treatment and Management of Rhinitis AllergyEdzhar HasiholanNo ratings yet
- Practical 9: Enthalpy Change of ReactionDocument4 pagesPractical 9: Enthalpy Change of ReactionJulia QistinaNo ratings yet
- Clarion CX Basics FundamentalsDocument15 pagesClarion CX Basics FundamentalsRajesh VenkatNo ratings yet
- Input OutputcrwillDocument21 pagesInput OutputcrwillAbhishek SinghNo ratings yet
- Nike Strategy AnalysisDocument24 pagesNike Strategy AnalysisasthapriyamvadaNo ratings yet
- How To Achieve A Rich Mindset PDFDocument11 pagesHow To Achieve A Rich Mindset PDFAsbo_Keno100% (1)
- Idbi - 5685 - Apr 2022Document15 pagesIdbi - 5685 - Apr 2022Rohan GuptaNo ratings yet
- Thesis Topics On Social EntrepreneurshipDocument6 pagesThesis Topics On Social EntrepreneurshipCollegePapersToBuySingapore100% (2)
- Persentasi Luwak CoffeeDocument36 pagesPersentasi Luwak CoffeeMukti LestariNo ratings yet
- BS 6089 - 2010 - Assessment of Insitu Compressive TestDocument40 pagesBS 6089 - 2010 - Assessment of Insitu Compressive TestMike Chan100% (2)
- List of RAs UpdatedDocument12 pagesList of RAs UpdatedThe SuperstarNo ratings yet
- MCQ Questions Set 2 Introduction To AccountingDocument3 pagesMCQ Questions Set 2 Introduction To AccountingHsiu PingNo ratings yet
- Your Paragraph TextDocument11 pagesYour Paragraph TextTalha AamirNo ratings yet
- Grlweap 2005Document3 pagesGrlweap 2005José RuizNo ratings yet
- Silentknight FACP Farenhyt IFP-1000 PDFDocument220 pagesSilentknight FACP Farenhyt IFP-1000 PDFwendy vegaNo ratings yet