You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5814)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (845)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Pathophysiology of NephrolithiasisDocument2 pagesPathophysiology of Nephrolithiasisanreilegarde80% (5)
- HBV Si HCV Studenti 201 PDFDocument117 pagesHBV Si HCV Studenti 201 PDFDianaTricoracheNo ratings yet
- DD Epi Eng Course Epidemiologic Process 21.05.18Document62 pagesDD Epi Eng Course Epidemiologic Process 21.05.18DianaTricoracheNo ratings yet
- ToxicoDocument200 pagesToxicoDianaTricoracheNo ratings yet
- Summer Practice FormDocument1 pageSummer Practice FormDianaTricoracheNo ratings yet
- Lesson 1 Oxygenation Suctioning Bronchial HygieneDocument14 pagesLesson 1 Oxygenation Suctioning Bronchial HygieneRENEROSE TORRESNo ratings yet
- SAUD VSD KonklinDocument91 pagesSAUD VSD KonklinDedy Tesna AmijayaNo ratings yet
- Acidosis AlkalosisDocument6 pagesAcidosis AlkalosisJm NapehewNo ratings yet
- Amr FactsheetDocument6 pagesAmr FactsheetAhmed .YNo ratings yet
- Vaccum Extraction-Maternal and Neonatal ComplicationsDocument5 pagesVaccum Extraction-Maternal and Neonatal ComplicationsSabrina JonesNo ratings yet
- Down SyndromeDocument3 pagesDown SyndromeMargie Ballesteros Manzano100% (1)
- NLRP3 Inflammasome and Its Inhibitors: A Review: Bo-Zong Shao, Zhe-Qi Xu, Bin-Ze Han, Ding-Feng Su and Chong LiuDocument9 pagesNLRP3 Inflammasome and Its Inhibitors: A Review: Bo-Zong Shao, Zhe-Qi Xu, Bin-Ze Han, Ding-Feng Su and Chong Liuilc67123No ratings yet
- UW Notes - 7 - Cardiology ArrangedDocument84 pagesUW Notes - 7 - Cardiology ArrangedAaquib AmirNo ratings yet
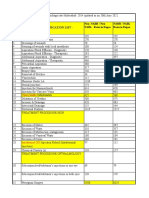
- CGHS Rates 2014 - HyderabadDocument60 pagesCGHS Rates 2014 - HyderabadPradeep PaswanNo ratings yet
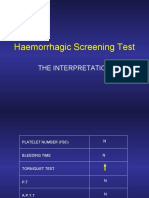
- Haemorrhagic Screening Test: The InterpretationDocument40 pagesHaemorrhagic Screening Test: The InterpretationAngel 冯晓君No ratings yet
- Epidemiology Lesson PlanDocument7 pagesEpidemiology Lesson PlanIshika RoyNo ratings yet
- Curcumin-Free Turmeric Exhibits Anti-Inflammatory and Anticancer Activities: Identification of Novel Components of TurmericDocument14 pagesCurcumin-Free Turmeric Exhibits Anti-Inflammatory and Anticancer Activities: Identification of Novel Components of TurmericHoàngTuấnNo ratings yet
- Canadian First Aid GuideDocument20 pagesCanadian First Aid GuideYvan SawadogoNo ratings yet
- Isoenzyme ClassifiedDocument33 pagesIsoenzyme Classifiedsayush754No ratings yet
- Querrey Biomedical Research CTR at Northwestern UniversityDocument4 pagesQuerrey Biomedical Research CTR at Northwestern UniversityAlbert MooreNo ratings yet
- Pediatric Red Ear Syndrome: A Case Report of An Erythromelalgia Type and Review of The LiteratureDocument4 pagesPediatric Red Ear Syndrome: A Case Report of An Erythromelalgia Type and Review of The LiteraturedanniwebbNo ratings yet
- Physiology of Limbic System by DR ShahabDocument23 pagesPhysiology of Limbic System by DR ShahabShahabuddin Shaikh100% (2)
- Drug Study On Mesalamine MercaptopurineDocument15 pagesDrug Study On Mesalamine Mercaptopurineسوما الشمريNo ratings yet
- Instructor Guide For Introduction To TCCC-MP 180801Document16 pagesInstructor Guide For Introduction To TCCC-MP 180801M. Owen ErwinNo ratings yet
- Disaster Nursing Cfu 084740Document9 pagesDisaster Nursing Cfu 084740Leone HeathensNo ratings yet
- Obstetrical Nursing NotesDocument25 pagesObstetrical Nursing NotesFreeNursingNotes81% (16)
- Semen Analysis: PG Resident, Department of Biochemistry, SGRRIMHS & SMI Hospital, DehradunDocument68 pagesSemen Analysis: PG Resident, Department of Biochemistry, SGRRIMHS & SMI Hospital, DehradunMarj MendezNo ratings yet
- Roxithromycin TabletDocument13 pagesRoxithromycin Tabletno debedeNo ratings yet
- Thesis Synopsis - Naveen ReddyDocument16 pagesThesis Synopsis - Naveen ReddyNaveen ReddyNo ratings yet
- Understanding Cancer - PPT LectureDocument169 pagesUnderstanding Cancer - PPT Lecturemirmodepon05100% (15)
- Question Paper of Dialysis CourseDocument5 pagesQuestion Paper of Dialysis Courserudreshbr rudriNo ratings yet
- 10D Health Problems Should MustDocument1 page10D Health Problems Should MustKin100% (1)
- Ovarian PatientDocument72 pagesOvarian PatientMan MeiNo ratings yet