You might also like
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (120)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- How To Get The Perfect Tattoo PDFDocument11 pagesHow To Get The Perfect Tattoo PDFSebastian GuevaraNo ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Empower 2e B1 Word List GermanDocument102 pagesEmpower 2e B1 Word List GermanOmid SofeNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Psychological TestingDocument149 pagesPsychological Testingxiejie22590No ratings yet
- L.P. of Transcultural NursingDocument14 pagesL.P. of Transcultural Nursingvikas takNo ratings yet
- Dental Laboratory Procedures FixedDocument477 pagesDental Laboratory Procedures FixedDINESH VENKATESANNo ratings yet
- Session Plan: Learning OutcomeDocument6 pagesSession Plan: Learning OutcomeByron AbelitaNo ratings yet
- Abdominal Aortic Aneurysm: AetiologyDocument7 pagesAbdominal Aortic Aneurysm: AetiologyKelvin MaikanaNo ratings yet
- Nursing ChecklistDocument6 pagesNursing Checklistbalaji srinivasan95% (20)
- Uterine Contractions in Normal Labor Developed byDocument4 pagesUterine Contractions in Normal Labor Developed byYuffaa AinayyaaNo ratings yet
- Ppk-Anestesi PDFDocument22 pagesPpk-Anestesi PDFYuffaa AinayyaaNo ratings yet
- Efektivitas Pelaksanaan Program Kampung Keluarga Berencana (KB) Kota Pekanbaru Oleh: Tiara Anggraini Pembimbing: Dadang Mashur, S.Sos., M.SiDocument11 pagesEfektivitas Pelaksanaan Program Kampung Keluarga Berencana (KB) Kota Pekanbaru Oleh: Tiara Anggraini Pembimbing: Dadang Mashur, S.Sos., M.SiYuffaa AinayyaaNo ratings yet
- Clinical Approach: Anemia in ChildhoodDocument30 pagesClinical Approach: Anemia in ChildhoodYuffaa AinayyaaNo ratings yet
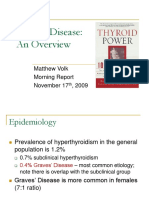
- 11.17.09 Volk GravesDocument17 pages11.17.09 Volk GravesJuan Daniel SidaurukNo ratings yet
- KeratitisDocument64 pagesKeratitisYuffaa AinayyaaNo ratings yet
- AbzhshajDocument53 pagesAbzhshajYuffaa AinayyaaNo ratings yet
- Clinical Question Search Strategy Critical Appraisal of FindingsDocument6 pagesClinical Question Search Strategy Critical Appraisal of FindingsYuffaa AinayyaaNo ratings yet
- Lakukan Critical Appraisal Dari Artikel Dengan Critical Appraisal WorksheetDocument3 pagesLakukan Critical Appraisal Dari Artikel Dengan Critical Appraisal WorksheetYuffaa AinayyaaNo ratings yet
- Harm Worksheet: BackgroundDocument3 pagesHarm Worksheet: BackgroundYuffaa AinayyaaNo ratings yet
- BMI ClassificationDocument1 pageBMI ClassificationMei Risanti SiraitNo ratings yet
- Research Article: Advancing Parental Age and Risk of Solid Tumors in Children: A Case-Control Study in PeruDocument10 pagesResearch Article: Advancing Parental Age and Risk of Solid Tumors in Children: A Case-Control Study in PeruYuffaa AinayyaaNo ratings yet
- BMI ClassificationDocument1 pageBMI ClassificationMei Risanti SiraitNo ratings yet
- Is Advanced Paternal Age A Health Risk For The Offspring?Document7 pagesIs Advanced Paternal Age A Health Risk For The Offspring?Yuffaa AinayyaaNo ratings yet
- Ni Hms 869320Document19 pagesNi Hms 869320Yuffaa AinayyaaNo ratings yet
- Primers 1 (15021), Hal 1-20: Daftar PustakaDocument2 pagesPrimers 1 (15021), Hal 1-20: Daftar PustakaYuffaa AinayyaaNo ratings yet
- New Doc 2019-08-05 13.05.09 - 20190805130600Document1 pageNew Doc 2019-08-05 13.05.09 - 20190805130600Yuffaa AinayyaaNo ratings yet
- Karakteristik Pasien Ocular Surface Nasional RS Mata Cicendo Periode Januari 2012-Juni 2014Document5 pagesKarakteristik Pasien Ocular Surface Nasional RS Mata Cicendo Periode Januari 2012-Juni 2014Yuffaa AinayyaaNo ratings yet
- KWKSKZBSJNZDocument20 pagesKWKSKZBSJNZYuffaa Ainayyaa0% (1)
- Pathophysiology of Graves' Ophthalmopathy: A Literature ReviewDocument11 pagesPathophysiology of Graves' Ophthalmopathy: A Literature ReviewYuffaa AinayyaaNo ratings yet
- Skripsi Tanpa PembahasanDocument53 pagesSkripsi Tanpa PembahasanYuffaa AinayyaaNo ratings yet
- Prop 4Document3 pagesProp 4Yuffaa AinayyaaNo ratings yet
- Research Article: Advancing Parental Age and Risk of Solid Tumors in Children: A Case-Control Study in PeruDocument10 pagesResearch Article: Advancing Parental Age and Risk of Solid Tumors in Children: A Case-Control Study in PeruYuffaa AinayyaaNo ratings yet
- Pathophysiology of Graves' Ophthalmopathy: A Literature ReviewDocument11 pagesPathophysiology of Graves' Ophthalmopathy: A Literature ReviewYuffaa AinayyaaNo ratings yet
- Design Solutions For Your Business-DikonversiDocument2 pagesDesign Solutions For Your Business-DikonversiYuffaa AinayyaaNo ratings yet
- Is Advanced Paternal Age A Health Risk For The Offspring?Document7 pagesIs Advanced Paternal Age A Health Risk For The Offspring?Yuffaa AinayyaaNo ratings yet
- Antiemetik WeteDocument80 pagesAntiemetik WeteWiwit ClimberNo ratings yet
- Is Advanced Paternal Age A Health Risk For The Offspring?Document7 pagesIs Advanced Paternal Age A Health Risk For The Offspring?Yuffaa AinayyaaNo ratings yet
- Prop 4Document3 pagesProp 4Yuffaa AinayyaaNo ratings yet
- Naturopathy-Well Care Centre: Twinkle Chandnani PEARL ACADEMY - (2012-2016) 2 MAY 2016Document28 pagesNaturopathy-Well Care Centre: Twinkle Chandnani PEARL ACADEMY - (2012-2016) 2 MAY 2016jarlinsujiNo ratings yet
- Specific Groups EssayDocument1 pageSpecific Groups Essaysunilvajshi2873No ratings yet
- MESS RISK ASSESMENT REPORT - Group 1 - D PDFDocument12 pagesMESS RISK ASSESMENT REPORT - Group 1 - D PDFSurajNo ratings yet
- APLEY & SOLOMON'S - 5. OsteoarthritisDocument19 pagesAPLEY & SOLOMON'S - 5. OsteoarthritisOngko SetunggalNo ratings yet
- The ScreamDocument2 pagesThe ScreamkaltraNo ratings yet
- Modern Spinsters in The Family and Kinship in The 21st CenturyDocument19 pagesModern Spinsters in The Family and Kinship in The 21st CenturyCentral Asian StudiesNo ratings yet
- GEN 013 Day 02 SASDocument5 pagesGEN 013 Day 02 SASAlbert King CambaNo ratings yet
- BGas InstructionDocument49 pagesBGas Instructionsamkarthik47No ratings yet
- Rehabilitation - A New Approach. Overview and Part One: The ProblemsDocument10 pagesRehabilitation - A New Approach. Overview and Part One: The ProblemsDumitru BiniucNo ratings yet
- Dr. Shanthi Rengarajan V The Oriental Insurance CompanyDocument12 pagesDr. Shanthi Rengarajan V The Oriental Insurance Companyparvati anilkumarNo ratings yet
- Section 1 Product Identification: Material Safety Data SheetDocument4 pagesSection 1 Product Identification: Material Safety Data SheetPutri MasyitahNo ratings yet
- Introduction To SportsDocument16 pagesIntroduction To SportsAlabaster 3927No ratings yet
- امتحان شامل -أداة قياس المهارات العملية - 1Document1 pageامتحان شامل -أداة قياس المهارات العملية - 1Rn nadeenNo ratings yet
- Hope - 1 Grade 11: Exercise For FitnessDocument6 pagesHope - 1 Grade 11: Exercise For FitnessTABBAL JAN PAOLONo ratings yet
- 7 Ways To Treat Chronic Back Pain Without Surgery - Johns Hopkins MedicineDocument3 pages7 Ways To Treat Chronic Back Pain Without Surgery - Johns Hopkins MedicinechhavishNo ratings yet
- Public Health Dentistry Thesis TopicsDocument5 pagesPublic Health Dentistry Thesis Topicss0kuzej0byn2100% (2)
- LESSON 3: Exercise Variables and PrinciplesDocument31 pagesLESSON 3: Exercise Variables and PrinciplesCapulong Kimberly100% (1)
- Max BKG 9TH MRNDocument81 pagesMax BKG 9TH MRNPråbhåkår Ð ÅppûNo ratings yet
- Fetal DevelopmentDocument15 pagesFetal DevelopmentOmar HammadNo ratings yet
- Make Today Amazing Checklist Printable Guide PDFDocument5 pagesMake Today Amazing Checklist Printable Guide PDFemna fadliNo ratings yet
- Kidney Cara Jaga Buah PinggangDocument17 pagesKidney Cara Jaga Buah PinggangmachevallieNo ratings yet
- Fear of Public SpeakingDocument11 pagesFear of Public SpeakingMustanser GhiasNo ratings yet