You might also like
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (844)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5814)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Jack Up Drilling Rig PDFDocument2 pagesJack Up Drilling Rig PDFm3t4ph0RNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Generator ProtectionDocument10 pagesGenerator ProtectionSriram rams100% (1)
- Technical Training Course For ECDIS: WarningDocument84 pagesTechnical Training Course For ECDIS: Warningpsad80No ratings yet
- EE5518 VLSI Digital Circuit Design VLSI Digital Circuit DesignDocument39 pagesEE5518 VLSI Digital Circuit Design VLSI Digital Circuit DesignBharat Kumar100% (1)
- Chapter 2Document111 pagesChapter 2Phạm Ngọc Khánh An lớp 1.10No ratings yet
- Mary Higgins Clark SamplerDocument208 pagesMary Higgins Clark SamplerSimon and SchusterNo ratings yet
- Cargo Terminal Standards 121021Document16 pagesCargo Terminal Standards 121021suryakeshwar singhNo ratings yet
- VBA 21 0960Q 1 ARE Chronic Fatigue SyndromeDocument3 pagesVBA 21 0960Q 1 ARE Chronic Fatigue SyndromeCombat CraigNo ratings yet
- VBA 21 0960P 1 ARE Eating DisorderDocument2 pagesVBA 21 0960P 1 ARE Eating DisorderCombat CraigNo ratings yet
- VBA-21-0960N-2-ARE EyesDocument10 pagesVBA-21-0960N-2-ARE EyesCombat CraigNo ratings yet
- Vba 21 0960p 3 Are PTSD ReviewDocument6 pagesVba 21 0960p 3 Are PTSD ReviewCombat CraigNo ratings yet
- VBA-21-0960M-2-ARE Ankle PDFDocument9 pagesVBA-21-0960M-2-ARE Ankle PDFCombat CraigNo ratings yet
- VBA-21-0960P-2-ARE Mental Other Than PTSD and EatingDocument5 pagesVBA-21-0960P-2-ARE Mental Other Than PTSD and EatingCombat CraigNo ratings yet
- Wrist Conditions Disability Benefits QuestionnaireDocument8 pagesWrist Conditions Disability Benefits QuestionnaireCombat CraigNo ratings yet
- VBA 21 0960M 9 ARE Knee and Lower LegDocument10 pagesVBA 21 0960M 9 ARE Knee and Lower LegCombat CraigNo ratings yet
- VBA 21 0960N 3 ARE Sense of SmellDocument2 pagesVBA 21 0960N 3 ARE Sense of SmellCombat CraigNo ratings yet
- VBA 21 0960M 12 ARE Shoulder and ArmDocument9 pagesVBA 21 0960M 12 ARE Shoulder and ArmCombat CraigNo ratings yet
- VBA 21 0960M 10 ARE Muscle InjuriesDocument6 pagesVBA 21 0960M 10 ARE Muscle InjuriesCombat CraigNo ratings yet
- VBA 21 0960M 11 ARE OsteomyelitisDocument4 pagesVBA 21 0960M 11 ARE OsteomyelitisCombat CraigNo ratings yet
- VBA 21 0960M 14 ARE ThoracolumbarDocument11 pagesVBA 21 0960M 14 ARE ThoracolumbarCombat CraigNo ratings yet
- Vba 21 0960m 13 Are CervicalDocument11 pagesVba 21 0960m 13 Are CervicalCombat CraigNo ratings yet
- VBA-21-0960J-1-ARE Kidney PDFDocument5 pagesVBA-21-0960J-1-ARE Kidney PDFCombat CraigNo ratings yet
- VBA-21-0960J-2-ARE Male Reproductive PDFDocument6 pagesVBA-21-0960J-2-ARE Male Reproductive PDFCombat CraigNo ratings yet
- VBA-21-0960M-1-ARE Amputations PDFDocument4 pagesVBA-21-0960M-1-ARE Amputations PDFCombat CraigNo ratings yet
- VBA-21-0960J-3-ARE Prostate Cancer PDFDocument3 pagesVBA-21-0960J-3-ARE Prostate Cancer PDFCombat CraigNo ratings yet
- VBA-21-0960K-2-ARE Gynecology PDFDocument6 pagesVBA-21-0960K-2-ARE Gynecology PDFCombat CraigNo ratings yet
- VBA-21-0960L-2-ARE Sleep Apnea PDFDocument2 pagesVBA-21-0960L-2-ARE Sleep Apnea PDFCombat CraigNo ratings yet
- VBA-21-0960J-4-ARE Urinary PDFDocument4 pagesVBA-21-0960J-4-ARE Urinary PDFCombat CraigNo ratings yet
- VBA-21-0960G-1-ARE Esophageal GERD PDFDocument4 pagesVBA-21-0960G-1-ARE Esophageal GERD PDFCombat CraigNo ratings yet
- VBA-21-0960G-4-ARE Intestinal Surgery PDFDocument3 pagesVBA-21-0960G-4-ARE Intestinal Surgery PDFCombat CraigNo ratings yet
- VBA-21-0960G-2-ARE Gallbladder Pancreas PDFDocument4 pagesVBA-21-0960G-2-ARE Gallbladder Pancreas PDFCombat CraigNo ratings yet
- VBA-21-0960F-2-ARE Skin PDFDocument5 pagesVBA-21-0960F-2-ARE Skin PDFCombat CraigNo ratings yet
- Common Interview Questions WorksheetDocument3 pagesCommon Interview Questions Worksheetprince husainNo ratings yet
- Mte 10Document10 pagesMte 10VipinNo ratings yet
- The Relationship Between The Effectiveness of PresDocument8 pagesThe Relationship Between The Effectiveness of PresNiki Ando PatinandoNo ratings yet
- Hs English 12 Unit01Document6 pagesHs English 12 Unit01Nguyễn Tài ThiệpNo ratings yet
- Mia by Law Fundamental-ObjectivityDocument5 pagesMia by Law Fundamental-ObjectivityFatinah Husna100% (1)
- Drainage Morphology of Imo Basin in The Anambra - Imo River Basin Area, of Imo State, Southern NigeriaDocument11 pagesDrainage Morphology of Imo Basin in The Anambra - Imo River Basin Area, of Imo State, Southern NigeriannekaNo ratings yet
- PreviewDocument55 pagesPreviewNway Moe SaungNo ratings yet
- PV Technology - LatestDocument21 pagesPV Technology - LatestZaferullah KhanNo ratings yet
- Resultant of Concurrent Force System - Engineering Mechanics ReviewDocument2 pagesResultant of Concurrent Force System - Engineering Mechanics Reviewimrancenakk0% (2)
- Wang1996 Design and Performance Prediction PDFDocument14 pagesWang1996 Design and Performance Prediction PDFalper yeterNo ratings yet
- Module 1 2nd Quarter d11Document5 pagesModule 1 2nd Quarter d11Abbie RañosaNo ratings yet
- Central Mosque Northampton: 112 116. Abington Avenue Abington, Northampton Nn1 4PdDocument1 pageCentral Mosque Northampton: 112 116. Abington Avenue Abington, Northampton Nn1 4PdAshraf OsmaniNo ratings yet
- Stilmas Vapour Compression StillsDocument2 pagesStilmas Vapour Compression StillsKarim PanjwaniNo ratings yet
- Brother Mfc-9420cn PartsDocument34 pagesBrother Mfc-9420cn PartsNikolaos MavridisNo ratings yet
- SpeechDocument2 pagesSpeechAyu RiyuningNo ratings yet
- Tale of Two SievesDocument13 pagesTale of Two SievesMark MarkesonNo ratings yet
- 03-001 Thinking Like A Programmer - Pseudo Code IDocument9 pages03-001 Thinking Like A Programmer - Pseudo Code IzakdejonghNo ratings yet
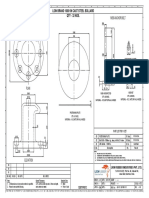
- M56 Anchor Bolt: Lion Brand 1000 KN Cast Steel Bollard Qty - 32 NosDocument1 pageM56 Anchor Bolt: Lion Brand 1000 KN Cast Steel Bollard Qty - 32 NossanaNo ratings yet
- Answer Key-Averages ExerciseDocument3 pagesAnswer Key-Averages ExerciseVanshika WadhwaniNo ratings yet
- Learning Vs Design SchoolDocument3 pagesLearning Vs Design SchoolRupashi GoyalNo ratings yet
- Alpine MRP F240Document18 pagesAlpine MRP F240chris_barnesNo ratings yet
- Asignación Final InglésDocument2 pagesAsignación Final InglésMarcela GonzálezNo ratings yet
- Plastics Training 101: Here's A Quick Summary of The Various Training Methods Available To Plastics ProcessorsDocument2 pagesPlastics Training 101: Here's A Quick Summary of The Various Training Methods Available To Plastics ProcessorsFITIWINo ratings yet