You might also like
- List of International Journals by SubjectDocument529 pagesList of International Journals by SubjectAhmed Adel IbrahimNo ratings yet
- Barash Handbook PDFDocument1,020 pagesBarash Handbook PDFAdăscăliţeiCarmenNo ratings yet
- Esr Check ListDocument8 pagesEsr Check ListMona Ismail AlsomaliNo ratings yet
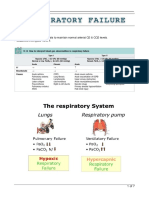
- Respiratory FailureDocument7 pagesRespiratory FailureLulu100% (1)
- Comprehensive Board Review 2015 PDFDocument713 pagesComprehensive Board Review 2015 PDFHuma KhalidNo ratings yet
- Copd ReportDocument69 pagesCopd ReportRadley Jed C. PelagioNo ratings yet
- 16 Martie - Curs BPOC - SlideDocument95 pages16 Martie - Curs BPOC - Slidejonah1024No ratings yet
- Funda NotesDocument55 pagesFunda NotesKristine CastilloNo ratings yet
- Chronic Obstructive Pulmonary Disease: Presented byDocument25 pagesChronic Obstructive Pulmonary Disease: Presented byChinni 12599No ratings yet
- PALS Interim Material 2020 - Provider Manual ChangesDocument3 pagesPALS Interim Material 2020 - Provider Manual ChangesyossyusNo ratings yet
- Advanced Tung Style Acupuncture Vol 5 PDFDocument280 pagesAdvanced Tung Style Acupuncture Vol 5 PDFnhung_nguyen_122100% (6)
- 10 1111@resp 13469Document10 pages10 1111@resp 13469César Avila JimenezNo ratings yet
- Noninvasive Ventilation For Acute Respiratory Failure: ReviewDocument6 pagesNoninvasive Ventilation For Acute Respiratory Failure: ReviewCharles SoNo ratings yet
- Niv Versus HFNCDocument30 pagesNiv Versus HFNCDukeNo ratings yet
- 10 1016@j JCRC 2020 08 008Document29 pages10 1016@j JCRC 2020 08 008GustavoGarcíaNo ratings yet
- Management of Postoperative HypoxemiaDocument14 pagesManagement of Postoperative HypoxemiaFavio Alvarez De BejarNo ratings yet
- Noninvasive Ventilation in Acute Respiratory FailureDocument6 pagesNoninvasive Ventilation in Acute Respiratory FailureCesar C SNo ratings yet
- β Agonist Delivery by High-Flow Nasal Cannula During COPD ExacerbationDocument8 pagesβ Agonist Delivery by High-Flow Nasal Cannula During COPD Exacerbationttiger zhaoNo ratings yet
- Application of Bipap Through Endotracheal Tube in Comatose Patients With Copd ExacerbationDocument5 pagesApplication of Bipap Through Endotracheal Tube in Comatose Patients With Copd ExacerbationMayco BiasibettiNo ratings yet
- Effectiveness of High-Flow Nasal Cannula Oxygen Therapy For Acute Respiratory Failure With HypercapniaDocument7 pagesEffectiveness of High-Flow Nasal Cannula Oxygen Therapy For Acute Respiratory Failure With Hypercapniarahma_husna_1No ratings yet
- Ja Oude 2019Document9 pagesJa Oude 2019yalocim666No ratings yet
- Year in Review 2019: High-Flow Nasal Cannula Oxygen Therapy For Adult SubjectsDocument13 pagesYear in Review 2019: High-Flow Nasal Cannula Oxygen Therapy For Adult SubjectsRicardoNo ratings yet
- Mechanical Ventilation I Hypoxemic Respiratory FailureDocument14 pagesMechanical Ventilation I Hypoxemic Respiratory FailureDavid ParraNo ratings yet
- Vmni Hipercapnia PDFDocument11 pagesVmni Hipercapnia PDFnicolas naranjoNo ratings yet
- Chronic Obstructive Pulmonary DiseaseDocument23 pagesChronic Obstructive Pulmonary DiseaseLe RobertNo ratings yet
- 19 (3.6)Document13 pages19 (3.6)JOHAN STEVEN COSME ARANZAZUNo ratings yet
- Chest 06-2643Document10 pagesChest 06-2643Margarida ReisNo ratings yet
- Noninvasive Ventilation For Patients Presenting With Acute Respiratory Failure: The Randomized Controlled TrialsDocument11 pagesNoninvasive Ventilation For Patients Presenting With Acute Respiratory Failure: The Randomized Controlled TrialsCesar C SNo ratings yet
- Agarwal - Bronchoscopic Lung Biopsy Using Noninvasive Ventilatory Support Case Series and Review of Literature of NIV-assisted BronchosDocument10 pagesAgarwal - Bronchoscopic Lung Biopsy Using Noninvasive Ventilatory Support Case Series and Review of Literature of NIV-assisted BronchosXaralyn XaviereNo ratings yet
- Jurnal MandiriDocument17 pagesJurnal Mandiriyuly rahmawatiNo ratings yet
- Hipertensi Pulmonal JurnalDocument7 pagesHipertensi Pulmonal JurnalAri PrakasaNo ratings yet
- Journal Reading ParuDocument53 pagesJournal Reading ParuDaniel IvanNo ratings yet
- Li Et Al 2020 Smoking Status Affects Clinical Characteristics and Disease Course of Acute Exacerbation of ChronicDocument10 pagesLi Et Al 2020 Smoking Status Affects Clinical Characteristics and Disease Course of Acute Exacerbation of ChronicNur Syah Fitriyana RamadhaniNo ratings yet
- PPHN Edit 17-FebDocument38 pagesPPHN Edit 17-FebAlbert GunawanNo ratings yet
- High Flow Nasal Oxygen in Patients With Covid 19 Associated Acute Respiratory FailureDocument3 pagesHigh Flow Nasal Oxygen in Patients With Covid 19 Associated Acute Respiratory FailureJevon AndraNo ratings yet
- Bronchodilator Reversibility in Chronic Obstructive Pulmonary Disease: Use and LimitationsDocument10 pagesBronchodilator Reversibility in Chronic Obstructive Pulmonary Disease: Use and LimitationsPutri Arasita RachmawatiNo ratings yet
- 2020 Article 2263Document11 pages2020 Article 2263EzeBorjesNo ratings yet
- Sinobronchial Syndrome in Japanese PeopleDocument7 pagesSinobronchial Syndrome in Japanese PeopleEsti yunita MasbaitNo ratings yet
- Resident:Dr. Melly Miranda Supervisor: Dr. Ali Nafiah Nasution, SP - JP (K)Document14 pagesResident:Dr. Melly Miranda Supervisor: Dr. Ali Nafiah Nasution, SP - JP (K)Melly MirandaNo ratings yet
- High Flow Nasal Cannula and Humidification: Nick Dalmon Staff Nurse Intensive Care, William Harvey HospitalDocument23 pagesHigh Flow Nasal Cannula and Humidification: Nick Dalmon Staff Nurse Intensive Care, William Harvey HospitalMori ArisandyNo ratings yet
- Pi Is 0012369216463579Document2 pagesPi Is 0012369216463579Nishant ShresthaNo ratings yet
- Respiratory Medicine CME: Lancelot Mark Pinto, Arpan Chandrakant Shah, Kushal Dipakkumar Shah, Zarir Farokh UdwadiaDocument3 pagesRespiratory Medicine CME: Lancelot Mark Pinto, Arpan Chandrakant Shah, Kushal Dipakkumar Shah, Zarir Farokh UdwadiaLintang SuroyaNo ratings yet
- 1374 FullDocument9 pages1374 FullElendisNo ratings yet
- Oxygen Therapy For Sepsis PatientDocument3 pagesOxygen Therapy For Sepsis PatientJulian LiemNo ratings yet
- Referat Bronkitis KronisDocument7 pagesReferat Bronkitis KronissamiratumananNo ratings yet
- Allison 2016 Non Invasive Ventilation For The EM PhysicianDocument12 pagesAllison 2016 Non Invasive Ventilation For The EM PhysicianSuwandi AlghozyNo ratings yet
- Epistimologi B.inggrisDocument3 pagesEpistimologi B.inggrisbudiNo ratings yet
- Effect On Oral NAC in COPDDocument5 pagesEffect On Oral NAC in COPDMeiyanti MeiyantiNo ratings yet
- Management of Acute Exacerbation of Copd: Dr. Fanny WS KoDocument3 pagesManagement of Acute Exacerbation of Copd: Dr. Fanny WS KoCalca NeusNo ratings yet
- Hipoxemia y VentilacionDocument14 pagesHipoxemia y VentilacionEVOLUCIONES UCI CLINICA CASANARENo ratings yet
- 2 RevistaDocument9 pages2 RevistaLucas QuilmesNo ratings yet
- 07 Treatment of Acute PDFDocument6 pages07 Treatment of Acute PDFNovia RambakNo ratings yet
- GavaertDocument8 pagesGavaertstanleyNo ratings yet
- Effectiveness of Noninvasive Ventilation in COVID-19 Relatedacute Respiratory Distress SyndromeDocument9 pagesEffectiveness of Noninvasive Ventilation in COVID-19 Relatedacute Respiratory Distress SyndromefikriafisNo ratings yet
- Preoxygenation For Tracheal Intubation in Critically Ill Patients: One Technique Does Not Fit AllDocument5 pagesPreoxygenation For Tracheal Intubation in Critically Ill Patients: One Technique Does Not Fit AllMarcela ParraNo ratings yet
- Rituximab - Pulmonary ToxicityDocument10 pagesRituximab - Pulmonary ToxicityRK SpartacusNo ratings yet
- Bell 2015Document5 pagesBell 2015Afien MuktiNo ratings yet
- Nasal High Flow Use in COPD Patients With - Hypercapnic Respiratory Failure - Treatment - Algorithm & Review of The LiteratureDocument12 pagesNasal High Flow Use in COPD Patients With - Hypercapnic Respiratory Failure - Treatment - Algorithm & Review of The Literaturettiger zhaoNo ratings yet
- Vallabhajosyula 2016Document10 pagesVallabhajosyula 2016Arick Frendi AndriyanNo ratings yet
- AECOPD GuidelineDocument8 pagesAECOPD GuidelineRonlie RonneyNo ratings yet
- High Flow Nasal Cannula Oxygen Therapy in Long Hauler Covid-19 PatientsDocument7 pagesHigh Flow Nasal Cannula Oxygen Therapy in Long Hauler Covid-19 PatientsFefiEkaWNo ratings yet
- Obesity Hypoventilation. Traditional Versus NontraditionalDocument11 pagesObesity Hypoventilation. Traditional Versus NontraditionalISABEL SOFIA CABARCAS COGOLLONo ratings yet
- Roca Et Al-2024-Intensive Care MedicineDocument4 pagesRoca Et Al-2024-Intensive Care MedicineSusana Simó MeléndezNo ratings yet
- Update in Airway Obstuction DiseaseDocument42 pagesUpdate in Airway Obstuction DiseaseTiyaTyraSidoraNo ratings yet
- Jurnal INTER BANTUL DG RIZADocument12 pagesJurnal INTER BANTUL DG RIZAMuhammad Amin KutbiNo ratings yet
- Bronchiolitis: Dr. Mustafa Mohamed Ahmed MBBS, MDDocument37 pagesBronchiolitis: Dr. Mustafa Mohamed Ahmed MBBS, MDYuusuf MubarikNo ratings yet
- Jurnal Kecemasan Pre Operasi 5 InggrisDocument8 pagesJurnal Kecemasan Pre Operasi 5 InggrisExtensi 2 STIKes MKNo ratings yet
- Sepsis 101: Colorado Hospital AssociationDocument27 pagesSepsis 101: Colorado Hospital Associationamal.fathullahNo ratings yet
- Basics of Critical Care.....Document34 pagesBasics of Critical Care.....XamanNo ratings yet
- Resus 8908 PLSDocument61 pagesResus 8908 PLSmipan zuzuNo ratings yet
- Geriatric NeuroanesthesiDocument333 pagesGeriatric NeuroanesthesiAdi Wira HadiNo ratings yet
- OPERATING ROOM TECHNIQUES NCM 112aDocument37 pagesOPERATING ROOM TECHNIQUES NCM 112aGrape JuiceNo ratings yet
- Healthcare Strings - BooleansDocument8 pagesHealthcare Strings - BooleansRahul DwivediNo ratings yet
- Anesthesia CourseDocument53 pagesAnesthesia CourseAdeel RaufNo ratings yet
- 1 Surgical MemorandumDocument1 page1 Surgical MemorandumAina HaravataNo ratings yet
- Clinical Anesthesia, 8Th Edition: Reviews of Educational MaterialDocument2 pagesClinical Anesthesia, 8Th Edition: Reviews of Educational MaterialAldous AgustinNo ratings yet
- ANAESTHESDocument2 pagesANAESTHESKhanNo ratings yet
- The Evolution of Veterinary Anaesthesia: "Shell" R S Arch Limited, Tunstall Laboratory Sittingbourne KentDocument7 pagesThe Evolution of Veterinary Anaesthesia: "Shell" R S Arch Limited, Tunstall Laboratory Sittingbourne KentDiana NiculaeNo ratings yet
- Intrathecal Morphine For Analgesia in Minimally Invasive Cardiac Surgery: A Randomized, Placebo-Controlled, Double-Blinded Clinical TrialDocument13 pagesIntrathecal Morphine For Analgesia in Minimally Invasive Cardiac Surgery: A Randomized, Placebo-Controlled, Double-Blinded Clinical TrialLidwina ApyakaNo ratings yet
- Tracheal Intubation: Airway AssessmentDocument7 pagesTracheal Intubation: Airway AssessmentElle ReyesNo ratings yet
- HPL 2021-22Document27 pagesHPL 2021-22sai projectNo ratings yet
- Ab Arogyadaan SchemeDocument11 pagesAb Arogyadaan SchemeSrinivas Kumar KNo ratings yet
- Blood Gas AnalysisDocument28 pagesBlood Gas AnalysiskempolonNo ratings yet
- Independent/Advanced Practice NurseDocument25 pagesIndependent/Advanced Practice NurseswethashakiNo ratings yet
- Sndromededistrsrespiratorioagudoenpediatra Rivero NeumolPediatr2016Document8 pagesSndromededistrsrespiratorioagudoenpediatra Rivero NeumolPediatr2016leslyjanetNo ratings yet
- 8a. General AnaesthesiaDocument28 pages8a. General Anaesthesiamatchees-gone rogueNo ratings yet
- Principles and Practice of Percutaneous TracheostomyDocument180 pagesPrinciples and Practice of Percutaneous TracheostomyFlorentino EspitiaNo ratings yet
- Comparison of General and Regional Anesthesia in Morbidly Obese Patient Case Report Ijdmd 18Document4 pagesComparison of General and Regional Anesthesia in Morbidly Obese Patient Case Report Ijdmd 18Djustiela KarrangNo ratings yet
- Dramatic Cervical Spine Injury Secondary To Videolaryngoscopy inDocument2 pagesDramatic Cervical Spine Injury Secondary To Videolaryngoscopy inJoyce CarolineNo ratings yet