You might also like
- Overcoming Barriers To Using Telehealth For Standardized Language AssessmentsDocument11 pagesOvercoming Barriers To Using Telehealth For Standardized Language Assessments賴奕全No ratings yet
- 2017 Wales THE EFFICACY OF TELEHEALTH DELIVERED SPEECHDocument16 pages2017 Wales THE EFFICACY OF TELEHEALTH DELIVERED SPEECHpaulinaovNo ratings yet
- Clinician Perspectives On Telehealth Assessment of Autism Spectrum Disorder During The COVID-19 PandemicDocument16 pagesClinician Perspectives On Telehealth Assessment of Autism Spectrum Disorder During The COVID-19 PandemicrenatoNo ratings yet
- Aud 0000000000000212Document10 pagesAud 0000000000000212axel pqNo ratings yet
- Kegunaan Bahan BangunanDocument11 pagesKegunaan Bahan BangunanyofitaNo ratings yet
- Treating Rural Pediatric Obesity Through Telemedicine: Baseline Data From A Randomized Controlled TrialDocument9 pagesTreating Rural Pediatric Obesity Through Telemedicine: Baseline Data From A Randomized Controlled Trialapi-546998503No ratings yet
- Hodge 2018Document7 pagesHodge 2018Ines Arias PazNo ratings yet
- 1-22 Cole, Pickard Et Al., 2019 TelehealthDocument8 pages1-22 Cole, Pickard Et Al., 2019 Telehealthamericangurl1284681No ratings yet
- Early Intervention Guidelines for Deaf ChildrenDocument42 pagesEarly Intervention Guidelines for Deaf ChildrenNadzira KarimaNo ratings yet
- EhswallDocument15 pagesEhswallapi-533702960No ratings yet
- Assessment of Hearing Loss in ChildrenDocument25 pagesAssessment of Hearing Loss in ChildrenCristóbal Murillo MuñozNo ratings yet
- Part C EligibilityDocument6 pagesPart C Eligibilityapi-260192872No ratings yet
- 1 s2.0 S0738399121001701 MainDocument8 pages1 s2.0 S0738399121001701 MainYaumil FauziahNo ratings yet
- Early Intervention in Children 0 6 Years With A R 2014 Hong Kong Journal oDocument9 pagesEarly Intervention in Children 0 6 Years With A R 2014 Hong Kong Journal oCostiNo ratings yet
- Alighieri 2020Document10 pagesAlighieri 2020Natalia AlberoNo ratings yet
- Inclusion of Toddlers - AutismDocument18 pagesInclusion of Toddlers - AutismVarvara MarkoulakiNo ratings yet
- Pediatric TeleNP Feasibility and RecommendationsDocument11 pagesPediatric TeleNP Feasibility and RecommendationsInes Arias PazNo ratings yet
- Báo 3Document9 pagesBáo 3Thanh Nhàn Nguyễn ThịNo ratings yet
- Early Hearing Detection and InterventionDocument10 pagesEarly Hearing Detection and InterventionNina KondićNo ratings yet
- J Jfludis 2021 105843Document21 pagesJ Jfludis 2021 105843ANDREA MIRANDA MEZA GARNICANo ratings yet
- Health Care Changes For Children With Special Health CareDocument8 pagesHealth Care Changes For Children With Special Health CareexaNo ratings yet
- Capstone HuacasiDocument40 pagesCapstone Huacasiapi-397532577No ratings yet
- Comparing hearing screening outcomes using smartphone audiometry by specialist and non-specialist healthcare workersDocument10 pagesComparing hearing screening outcomes using smartphone audiometry by specialist and non-specialist healthcare workersNadia DhyaNo ratings yet
- Csa ExaminationDocument21 pagesCsa ExaminationCorina IoanaNo ratings yet
- Home-Based Early Intervention With Families of Children With Disabilities: Who Is Doing What?Document25 pagesHome-Based Early Intervention With Families of Children With Disabilities: Who Is Doing What?eebook123456No ratings yet
- Efficacy of A Reading and Language Intervention For Children With Down Syndrome: A Randomized Controlled TrialDocument10 pagesEfficacy of A Reading and Language Intervention For Children With Down Syndrome: A Randomized Controlled TrialRubashni SubramaniamNo ratings yet
- Children and Youth Services Review: Sarah Dababnah, Susan L. Parish, Lauren Turner Brown, Stephen R. HooperDocument7 pagesChildren and Youth Services Review: Sarah Dababnah, Susan L. Parish, Lauren Turner Brown, Stephen R. HooperDanya KatsNo ratings yet
- Pathways To Services For Children With Cerebral Palsy in Selangor and The Federal Territory, Kuala LumpurDocument4 pagesPathways To Services For Children With Cerebral Palsy in Selangor and The Federal Territory, Kuala LumpurAznaeym AbdLatifNo ratings yet
- Assessment of Co-Occurring Disabilities in Young Children Who AreDocument24 pagesAssessment of Co-Occurring Disabilities in Young Children Who AreMariana BucurNo ratings yet
- Knowledge, Attitude of Sikkim Primary School Teachers About Paediatric Hearing LossDocument6 pagesKnowledge, Attitude of Sikkim Primary School Teachers About Paediatric Hearing LossMaria P12No ratings yet
- Cochlear ImplantsDocument53 pagesCochlear ImplantsSovitJungBaralNo ratings yet
- 2019 - JSLHR S 18 0301Document17 pages2019 - JSLHR S 18 0301Andreia TavaresNo ratings yet
- Practice: Social Work in ActionDocument17 pagesPractice: Social Work in ActionUSFMFPNo ratings yet
- Telepsychiatry: Effective, Evidence-Based, and at A Tipping Point in Health Care Delivery?Document34 pagesTelepsychiatry: Effective, Evidence-Based, and at A Tipping Point in Health Care Delivery?Riza Agung NugrahaNo ratings yet
- AAPD Teledentistry 2021Document2 pagesAAPD Teledentistry 2021Francisca Abarca CifuentesNo ratings yet
- A North Dakota Prevalence Study of Nonverbal School-Age ChildrenDocument13 pagesA North Dakota Prevalence Study of Nonverbal School-Age ChildrenJaavyeraa' BelenNo ratings yet
- Nur 330 - Health Promotion ProjectDocument12 pagesNur 330 - Health Promotion Projectapi-375928224No ratings yet
- Ford 2003Document9 pagesFord 2003Arif Erdem KöroğluNo ratings yet
- 2008 Mashima Overview of Telehealth Activities inDocument17 pages2008 Mashima Overview of Telehealth Activities inLucia CavasNo ratings yet
- Beliefs of Filipino Caregivers On Occupational Therapy Through TelehealthDocument4 pagesBeliefs of Filipino Caregivers On Occupational Therapy Through TelehealthBETINA NICOLE SYNo ratings yet
- Guidelines AconselhamentoDocument28 pagesGuidelines Aconselhamentoraquelgsilva17No ratings yet
- Part C Early Intervention Enrollment Patterns in Low Birth Weight InfantsDocument7 pagesPart C Early Intervention Enrollment Patterns in Low Birth Weight InfantsFarin MauliaNo ratings yet
- Interact Integrate ImpactDocument11 pagesInteract Integrate ImpactSanziana SavaNo ratings yet
- Economics of Education Review 72 (2019) 30-43Document14 pagesEconomics of Education Review 72 (2019) 30-43iraastutikNo ratings yet
- Training Adults and Children with ASD to be Compliant with Dental AssessmentsDocument10 pagesTraining Adults and Children with ASD to be Compliant with Dental AssessmentsSpecial CareNo ratings yet
- The Bucharest Early Intervention Project - Adolescent Mental Health and Adaptation Following Early DeprivationDocument8 pagesThe Bucharest Early Intervention Project - Adolescent Mental Health and Adaptation Following Early DeprivationMerly JHNo ratings yet
- Negotiating Knowledge - Parents Experience of The NeuropsychiatricDocument11 pagesNegotiating Knowledge - Parents Experience of The NeuropsychiatricKarel GuevaraNo ratings yet
- It Felt Like There Was Always Someone There For Us Supporting ChildrenDocument10 pagesIt Felt Like There Was Always Someone There For Us Supporting ChildrenHuế Nguyễn PhươngNo ratings yet
- Child Development - 2011 - Lowell - A Randomized Controlled Trial of Child FIRST A Comprehensive Home‐Based InterventionDocument16 pagesChild Development - 2011 - Lowell - A Randomized Controlled Trial of Child FIRST A Comprehensive Home‐Based InterventionCláudia Isabel SilvaNo ratings yet
- 1 s2.0 S0190740915000870 Main PDFDocument7 pages1 s2.0 S0190740915000870 Main PDFYusranNo ratings yet
- Caso Programa TeacchDocument12 pagesCaso Programa TeacchsaraNo ratings yet
- Early Intervention Guidelines for Children with Hearing LossDocument2 pagesEarly Intervention Guidelines for Children with Hearing LossAbuzar AliNo ratings yet
- Early InterventionDocument13 pagesEarly Interventionapi-290229666No ratings yet
- OSF FinalDocument38 pagesOSF Finalinas zahraNo ratings yet
- Telehealth As A Model For Providing Behaviour AnalDocument36 pagesTelehealth As A Model For Providing Behaviour AnalNabilah AuliaNo ratings yet
- Diaryquestionnairetv 2Document17 pagesDiaryquestionnairetv 2GeorgetownELPNo ratings yet
- LR EffectivenessDocument24 pagesLR Effectivenessapi-349022556No ratings yet
- Systematic Review of Effective Strategies For Reducing Screen Time Among Young ChildrenDocument17 pagesSystematic Review of Effective Strategies For Reducing Screen Time Among Young ChildrenAdrienn MatheNo ratings yet
- Clinical Guide to Assessment and Treatment of Communication DisordersFrom EverandClinical Guide to Assessment and Treatment of Communication DisordersNo ratings yet
- Supporting Families Experiencing Homelessness: Current Practices and Future DirectionsFrom EverandSupporting Families Experiencing Homelessness: Current Practices and Future DirectionsNo ratings yet
- Baby Mouse PatternDocument27 pagesBaby Mouse Patternlamarinescu100% (1)
- Marriage and Family Therapists Working With Couples Who Have Children With AutismDocument12 pagesMarriage and Family Therapists Working With Couples Who Have Children With AutismanaNo ratings yet
- TI Participation Consent FormDocument2 pagesTI Participation Consent FormanaNo ratings yet
- Implementing and Preparing For Home VisitsDocument10 pagesImplementing and Preparing For Home VisitsanaNo ratings yet
- Telepractice Self Eval Form PDFDocument1 pageTelepractice Self Eval Form PDFanaNo ratings yet
- Telepractice Self Eval Form PDFDocument1 pageTelepractice Self Eval Form PDFanaNo ratings yet
- DEC - RPs - 5-1-14 PDFDocument14 pagesDEC - RPs - 5-1-14 PDFanaNo ratings yet
- DEC - RPs - 5-1-14 PDFDocument14 pagesDEC - RPs - 5-1-14 PDFanaNo ratings yet
- Checklist For Determining Home Capacity For Tele PDFDocument1 pageChecklist For Determining Home Capacity For Tele PDFanaNo ratings yet
- Family Routines Inventory PDFDocument2 pagesFamily Routines Inventory PDFanaNo ratings yet
- Modern College Arts Time Table TYBA Sem VI March 2022Document2 pagesModern College Arts Time Table TYBA Sem VI March 2022Aniket SalveNo ratings yet
- PC 314 REVIEWER QUIZ 1 AND 2Document10 pagesPC 314 REVIEWER QUIZ 1 AND 2Victor S. Suratos Jr.No ratings yet
- Luo - Plo4 - Edte608 Final Assessment ProjectDocument7 pagesLuo - Plo4 - Edte608 Final Assessment Projectapi-549590947No ratings yet
- Results-Based Performance Management System (RPMS) : PortfolioDocument82 pagesResults-Based Performance Management System (RPMS) : PortfolioLilibeth Allosada LapathaNo ratings yet
- Pangasinan State UniversityDocument6 pagesPangasinan State UniversityGretz DoriaNo ratings yet
- Summury of A Research in DEDocument2 pagesSummury of A Research in DEu061542No ratings yet
- Welcome Madison 2013 2014Document97 pagesWelcome Madison 2013 2014Alexander León PuelloNo ratings yet
- Farwell SpeechDocument1 pageFarwell SpeechSaurabh ChaturvediNo ratings yet
- LAS 432 Technology, Society, and CultureDocument5 pagesLAS 432 Technology, Society, and CultureAlan MarkNo ratings yet
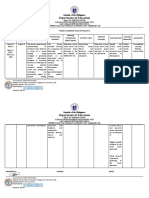
- Eng8 WLP Q3 Week3Document3 pagesEng8 WLP Q3 Week3ANNABEL PALMARINNo ratings yet
- Devachan or HeavenworldDocument14 pagesDevachan or HeavenworldOldan AguilarNo ratings yet
- Mukhyamantri Yuva Scholarship DetailsDocument1 pageMukhyamantri Yuva Scholarship DetailsUtsavNo ratings yet
- Study and Reference Guide-Instructor RatingDocument7 pagesStudy and Reference Guide-Instructor RatingJeff LightheartNo ratings yet
- Good Math Lesson PlansDocument36 pagesGood Math Lesson PlansZulsubhaDaniSiti100% (1)
- Architectural School Design Study CasesDocument117 pagesArchitectural School Design Study CasesRazan KhrisatNo ratings yet
- Task Sheet 1.1-5 RevisedDocument3 pagesTask Sheet 1.1-5 RevisedEL FuentesNo ratings yet
- WEB-Robot Awakening Kinder 2 (English)Document131 pagesWEB-Robot Awakening Kinder 2 (English)Administracion TuproyectoNo ratings yet
- Night Figurative LanguageDocument2 pagesNight Figurative Languageapi-542555028No ratings yet
- Fixed Mindset Vs Growth MindsetDocument16 pagesFixed Mindset Vs Growth MindsetTop Gear AutosNo ratings yet
- Date Sheet Term II Assessment II 2022-23Document2 pagesDate Sheet Term II Assessment II 2022-23nameNo ratings yet
- Ingles 1 Modelo de ExamenDocument5 pagesIngles 1 Modelo de ExamenNiki LMNo ratings yet
- Classroom Structure ChecklistDocument1 pageClassroom Structure ChecklistBella Bella100% (1)
- Accreditation Standard For Quality School Governance - Application - 1Document10 pagesAccreditation Standard For Quality School Governance - Application - 1Ankur DhirNo ratings yet
- Par Statements - Updated 2016Document2 pagesPar Statements - Updated 2016K DNo ratings yet
- B.ed SyllabusDocument123 pagesB.ed SyllabusextraworkxNo ratings yet
- NetApp Partner LevelsDocument1 pageNetApp Partner LevelsPanzo Vézua GarciaNo ratings yet
- Contoh Soalan Public PerceptionDocument27 pagesContoh Soalan Public Perception12035safyaabdulmalikNo ratings yet
- Karina Castillo: I Am A 30 Year Old Woman Looking To Further Expand My Career As A Session Singer in The Music IndustryDocument7 pagesKarina Castillo: I Am A 30 Year Old Woman Looking To Further Expand My Career As A Session Singer in The Music IndustryKarina PorterNo ratings yet
- Allison ResumeDocument2 pagesAllison Resumeapi-351570174No ratings yet
- Bridge Technical Expert to Modernize Nepal's Bridge TechnologiesDocument6 pagesBridge Technical Expert to Modernize Nepal's Bridge TechnologiesRam NepaliNo ratings yet