You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Acknowledging Contributors to a Surgery Review GuideDocument21 pagesAcknowledging Contributors to a Surgery Review GuideSharad Patel100% (2)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Understanding Kundalini Energy and its Role in Spiritual EvolutionDocument190 pagesUnderstanding Kundalini Energy and its Role in Spiritual Evolutionnityanandroy100% (1)
- Surgery BoardsDocument16 pagesSurgery Boardscusom34100% (1)
- Behind The Knife’s Quick Hits for Anesthesia and SurgeryDocument24 pagesBehind The Knife’s Quick Hits for Anesthesia and Surgerycusom34No ratings yet
- Behind The Knife’s Quick Hits for Anesthesia and SurgeryDocument24 pagesBehind The Knife’s Quick Hits for Anesthesia and Surgerycusom34No ratings yet
- Microsurgery ArticleDocument6 pagesMicrosurgery Articlecusom34No ratings yet
- Head and Neck Free - Ap Reconstruction in The Elderly: E.E.M. NaoDocument5 pagesHead and Neck Free - Ap Reconstruction in The Elderly: E.E.M. Naocusom34No ratings yet
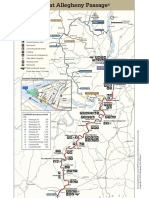
- Bike It Map Gap WebDocument2 pagesBike It Map Gap Webcusom34No ratings yet
- Investigation of Free-Flap Transfer Reconstruction in Elderly Patients and Oral Intake FunctionDocument3 pagesInvestigation of Free-Flap Transfer Reconstruction in Elderly Patients and Oral Intake Functioncusom34No ratings yet
- Efficacy of Anti-Interleukin-1 Receptor Antagonist Anakinra (Kineret of Refractory Sweet's SyndromeDocument5 pagesEfficacy of Anti-Interleukin-1 Receptor Antagonist Anakinra (Kineret of Refractory Sweet's Syndromecusom34No ratings yet
- Synpor Synthes Porous Polyethylene Implant: Surgical TechniqueDocument16 pagesSynpor Synthes Porous Polyethylene Implant: Surgical Techniquecusom34No ratings yet
- Rhinplasty For Adult Cleft Lip Nasal Deformity PDFDocument26 pagesRhinplasty For Adult Cleft Lip Nasal Deformity PDFcusom34No ratings yet
- Rhinplasty For Adult Cleft Lip Nasal Deformity PDFDocument26 pagesRhinplasty For Adult Cleft Lip Nasal Deformity PDFcusom34No ratings yet
- Pediatric PatientDocument29 pagesPediatric Patientcusom34No ratings yet
- Autologous Fat Grafting - Harvesting Techniques PDFDocument7 pagesAutologous Fat Grafting - Harvesting Techniques PDFcusom34No ratings yet
- Pediatric PatientDocument29 pagesPediatric Patientcusom34No ratings yet
- Testosterone SummaryDocument35 pagesTestosterone Summarycusom34No ratings yet
- Aging Neck ManagementDocument10 pagesAging Neck Managementcusom34No ratings yet
- Anatomical Basis of The Posterior Brachial Skin Flap: SummaryDocument6 pagesAnatomical Basis of The Posterior Brachial Skin Flap: Summarycusom34No ratings yet
- Autologous Fat Grafting - Harvesting Techniques PDFDocument7 pagesAutologous Fat Grafting - Harvesting Techniques PDFcusom34No ratings yet
- Anatomically Based Breast Augmentation: A 6-Plane Autologous ApproachDocument2 pagesAnatomically Based Breast Augmentation: A 6-Plane Autologous Approachcusom34No ratings yet
- Facial Reanimation With Masseter Nerve-Innervated Free Gracilis Muscle Transfer in Established Facial Palsy PatientsDocument7 pagesFacial Reanimation With Masseter Nerve-Innervated Free Gracilis Muscle Transfer in Established Facial Palsy Patientscusom34No ratings yet
- Original1.Chapter 53 Surgical Complications of Cirrhosis and Portal HypertensionDocument23 pagesOriginal1.Chapter 53 Surgical Complications of Cirrhosis and Portal Hypertensioncusom34No ratings yet
- Study of Neurovascular Anatomy of The Split Gracilis Facial ReanimaitonDocument9 pagesStudy of Neurovascular Anatomy of The Split Gracilis Facial Reanimaitoncusom34No ratings yet
- Indications and Cont in Total Breast Reconstruction With LipomodelingDocument7 pagesIndications and Cont in Total Breast Reconstruction With Lipomodelingcusom34No ratings yet
- Breast Reconstruction With Free Anterolateral Thigh FlapDocument6 pagesBreast Reconstruction With Free Anterolateral Thigh Flapcusom34No ratings yet
- Early Ambulation After Microsurgical Reconstruction of The Lower ExtremityDocument3 pagesEarly Ambulation After Microsurgical Reconstruction of The Lower Extremitycusom34No ratings yet
- Breast Reconstruction With Free Anterolateral Thigh FlapDocument5 pagesBreast Reconstruction With Free Anterolateral Thigh Flapcusom34No ratings yet
- Application of Extende D Bi-Pedicle Anterolateral Thigh Free Flaps For Reconstruction of Large Defects - A Case SeriesDocument8 pagesApplication of Extende D Bi-Pedicle Anterolateral Thigh Free Flaps For Reconstruction of Large Defects - A Case Seriescusom34No ratings yet
- ABSITE High YieldDocument2 pagesABSITE High Yieldcusom34100% (2)
- Flashcards in Abo Blood GroupDocument10 pagesFlashcards in Abo Blood GroupVincent ReyesNo ratings yet
- Pi Glycerine SuppositoriesDocument2 pagesPi Glycerine SuppositoriesMey KhNo ratings yet
- Clinical Protocol-Second Edition-November 2015Document26 pagesClinical Protocol-Second Edition-November 2015Michael KaiNo ratings yet
- bloodHT Exam QsDocument7 pagesbloodHT Exam QsPUNCHNo ratings yet
- PRISMA 2009 ChecklistDocument7 pagesPRISMA 2009 ChecklistRezky PutriNo ratings yet
- Uganda Universities and Courses For Student Loan SupportDocument5 pagesUganda Universities and Courses For Student Loan SupportThe Campus TimesNo ratings yet
- Chapple Et Al-2017-Journal of Clinical PeriodontologyDocument13 pagesChapple Et Al-2017-Journal of Clinical PeriodontologyJulio César PlataNo ratings yet
- Drugs For AmebiasisDocument13 pagesDrugs For AmebiasisDiartha Budi LegawaNo ratings yet
- Age Dependent ElectroencephaloDocument26 pagesAge Dependent ElectroencephaloHestySukmasariNo ratings yet
- CV - Dr. Atif Ashraf (Physician)Document6 pagesCV - Dr. Atif Ashraf (Physician)dratifashrafNo ratings yet
- Pacop Violet Pharmaceutical ChemistryDocument70 pagesPacop Violet Pharmaceutical ChemistryAstherielle GalvezNo ratings yet
- 2023 Aaha Senior Care Guidelines For Dogs and CatsDocument21 pages2023 Aaha Senior Care Guidelines For Dogs and CatsisvpNo ratings yet
- Radiologic Technologist Licensure Examination Results March 9 2022Document2 pagesRadiologic Technologist Licensure Examination Results March 9 2022RapplerNo ratings yet
- Adr 1Document18 pagesAdr 1shiv kumarNo ratings yet
- Oral Mucosal Lesions Associated With The Wearing of Removable DenturesDocument17 pagesOral Mucosal Lesions Associated With The Wearing of Removable DenturesnybabyNo ratings yet
- 2007 - Tu - Et - Al - 2007 - Revisiting The Relation Between Change and Initial ValueDocument15 pages2007 - Tu - Et - Al - 2007 - Revisiting The Relation Between Change and Initial ValueDanilo MoggiaNo ratings yet
- Syllabus For HAADDocument7 pagesSyllabus For HAADvirasamir100% (2)
- BISQDocument4 pagesBISQNanda Asyura RizkyaniNo ratings yet
- Emergency DrugsDocument19 pagesEmergency DrugsAdy PutroNo ratings yet
- Kinds of Diseases: Name: Rebekha Noveria NPM: 18.11.124 PSIK 3.1Document12 pagesKinds of Diseases: Name: Rebekha Noveria NPM: 18.11.124 PSIK 3.1Rebekha Noveria SitumorangNo ratings yet
- Symptomatology Close 1Document41 pagesSymptomatology Close 1Sk Saklin MustakNo ratings yet
- The Nursing Assessment of Peptic UlcerDocument14 pagesThe Nursing Assessment of Peptic UlcerVelia suwandiNo ratings yet
- Symposium Topic: Current Update in Diagnosis & Management of Emergency MedicineDocument2 pagesSymposium Topic: Current Update in Diagnosis & Management of Emergency MedicineAfriza AnggriniNo ratings yet
- Psychiatry: Mental State ExaminationDocument3 pagesPsychiatry: Mental State ExaminationSok-Moi Chok100% (3)
- Treatment of Adults With Anterior Mandibular Teeth Crowding: Reliability of Little's Irregularity IndexDocument8 pagesTreatment of Adults With Anterior Mandibular Teeth Crowding: Reliability of Little's Irregularity IndexNaeem MoollaNo ratings yet
- Pharma - M6L2 - Drug Therapy For OA and Gouty ArthritisDocument8 pagesPharma - M6L2 - Drug Therapy For OA and Gouty ArthritisAngelaTrinidadNo ratings yet
- Medical Practitioners 23-FEB-2012Document12 pagesMedical Practitioners 23-FEB-2012Next PersonNo ratings yet
- Lose Weight With Comfort Food Ou Love: NHS Chaos Chief Tells The PM: You Can't Sack Me..Document56 pagesLose Weight With Comfort Food Ou Love: NHS Chaos Chief Tells The PM: You Can't Sack Me..Anonymous 1z1cSi0IolNo ratings yet
- The Adornment of The Muslim Doctor (With Good Character)Document49 pagesThe Adornment of The Muslim Doctor (With Good Character)abu salmanNo ratings yet