You might also like
- EMPLOYMENT APPLICATIONDocument3 pagesEMPLOYMENT APPLICATIONizzul_125z1419No ratings yet
- THIBARMY Best Damn NATTY LIFTSDocument11 pagesTHIBARMY Best Damn NATTY LIFTSÒó Reverse100% (3)
- Joining Bupa GlobalDocument16 pagesJoining Bupa GlobalMayar RagabNo ratings yet
- BHF 01535Document8 pagesBHF 01535AlvinNo ratings yet
- WFP Application Form GuideDocument12 pagesWFP Application Form GuideGordonPhillipsNo ratings yet
- Application FormDocument3 pagesApplication FormAhrvin SGNo ratings yet
- Application Form MITDocument3 pagesApplication Form MITBudi TooleeNo ratings yet
- Separation Document - Ss293 1707en PDocument13 pagesSeparation Document - Ss293 1707en PMark LordNo ratings yet
- Newborn Application FormDocument2 pagesNewborn Application FormMicaela KrielNo ratings yet
- MHD app form (Trust)Document6 pagesMHD app form (Trust)mojija5822No ratings yet
- Separation Details: This Form Lets Us Know You Have Separated From Your PartnerDocument6 pagesSeparation Details: This Form Lets Us Know You Have Separated From Your PartnerBrooke ZarubinNo ratings yet
- 1 - Info Sheet English - Doc2Document7 pages1 - Info Sheet English - Doc2Niemar AbaloNo ratings yet
- GC Application FormDocument4 pagesGC Application FormmuzzamilNo ratings yet
- Application Form - PT I-Linkage International - UpdateDocument2 pagesApplication Form - PT I-Linkage International - UpdateDestri Rahma DonaNo ratings yet
- PDFDocument3 pagesPDFAjaegbu A.ONo ratings yet
- AP 336-1 Student Registration Form-Fillable Version - 8 - 0Document4 pagesAP 336-1 Student Registration Form-Fillable Version - 8 - 0Ashley LehmanNo ratings yet
- 1.formal ApplicationDocument8 pages1.formal ApplicationNaturalBite ChefNo ratings yet
- New Zealand Student Visa ApplicationDocument5 pagesNew Zealand Student Visa ApplicationCassia GonçalvesNo ratings yet
- Miss Supranational Philippines 2023 Application FormDocument3 pagesMiss Supranational Philippines 2023 Application FormpaoloplopenioNo ratings yet
- Patient Registration Form 1 2018 Adult UpdatedDocument4 pagesPatient Registration Form 1 2018 Adult UpdatedEskinderNo ratings yet
- London Children's Academy Enrolment Forms 2023Document11 pagesLondon Children's Academy Enrolment Forms 2023Gideon AnumbaNo ratings yet
- EPC Registration FormDocument2 pagesEPC Registration FormErika DuvallNo ratings yet
- Early Learning Application Form - November 2022 Fillable VersionDocument8 pagesEarly Learning Application Form - November 2022 Fillable Versiondiretoria cpvixpsicologiaNo ratings yet
- Marin Country Day School: Application For AdmissionDocument4 pagesMarin Country Day School: Application For AdmissionTammy NamNo ratings yet
- When To Use This Form: Servicesaustralia - Gov.au/centrelinkuploaddocsDocument10 pagesWhen To Use This Form: Servicesaustralia - Gov.au/centrelinkuploaddocsLyley YAYNo ratings yet
- Joining FormsDocument16 pagesJoining FormsGruchuNo ratings yet
- Access Florida Application Details 681754164 PDFDocument7 pagesAccess Florida Application Details 681754164 PDFDonellChristopherTorres0% (1)
- Enc Encoded SGQGMCVPKDB Fn5a5 tG2ZGpstncf9P9zwaoqfb7dMRlwKjBLAOioftCUGwDocument3 pagesEnc Encoded SGQGMCVPKDB Fn5a5 tG2ZGpstncf9P9zwaoqfb7dMRlwKjBLAOioftCUGwMJ Cortez PaguioNo ratings yet
- DS2444 A PrintDocument10 pagesDS2444 A PrintstatchuroseNo ratings yet
- Updated CDU Applicaion FormDocument4 pagesUpdated CDU Applicaion FormAbdul Lateef KhanNo ratings yet
- Application For Household Support GrantDocument5 pagesApplication For Household Support GrantgbabunetNo ratings yet
- Joining Kit: First Name Middle NameDocument20 pagesJoining Kit: First Name Middle NameDNYANESHWAR PAWARNo ratings yet
- AAT FormDocument10 pagesAAT Formrenniemac100% (2)
- PCA190114149 - Aplicacao Joao p1Document5 pagesPCA190114149 - Aplicacao Joao p1Cassia GonçalvesNo ratings yet
- Sample Preschool Registration FormDocument4 pagesSample Preschool Registration FormSir CalaqueiNo ratings yet
- Job Application Form - ExecutiveDocument2 pagesJob Application Form - ExecutiveWan Qing NgNo ratings yet
- Application LetterDocument3 pagesApplication LetterUtkarsh AnandNo ratings yet
- Fm-hr-002 Application Form Mit RhamandaniDocument2 pagesFm-hr-002 Application Form Mit RhamandaniRhamandani SudrajatNo ratings yet
- General Student Personal Information SheetDocument2 pagesGeneral Student Personal Information SheetKristal Joy Hermosa LindoNo ratings yet
- Application Form-1Document2 pagesApplication Form-1blue silverNo ratings yet
- Updated Application Form - HangryDocument20 pagesUpdated Application Form - HangryTaupan JainudinNo ratings yet
- Application FormDocument2 pagesApplication FormBernard Vincent Guitan MineroNo ratings yet
- Select/Premier Medical Plan: Application FormDocument6 pagesSelect/Premier Medical Plan: Application Formadobo sinigangNo ratings yet
- Commonwealth of Australia Statutory Declaration: Purpose of This Form For More InformationDocument4 pagesCommonwealth of Australia Statutory Declaration: Purpose of This Form For More InformationOm KarnNo ratings yet
- Revised GSK Application For Employment - With Criminal DisclosureDocument4 pagesRevised GSK Application For Employment - With Criminal DisclosurePravallika Rao TadepalliNo ratings yet
- Master Benefit ApplicationDocument6 pagesMaster Benefit ApplicationJulia RiveraNo ratings yet
- ACCESS Florida: Benefits InformationDocument8 pagesACCESS Florida: Benefits InformationCrystal HernandezNo ratings yet
- Visa Application FormDocument3 pagesVisa Application Formgirish kumarNo ratings yet
- UGC Bulletin 185Document18 pagesUGC Bulletin 185Rafin সাজ্জাদNo ratings yet
- Accommodation Details: When To Use This FormDocument10 pagesAccommodation Details: When To Use This FormwoodywheelNo ratings yet
- Enrolment Form ADocument8 pagesEnrolment Form Ajamesbond50No ratings yet
- Job Application Form: Position Applied ForDocument7 pagesJob Application Form: Position Applied ForAhmad MarzukiNo ratings yet
- Child B2Document9 pagesChild B2myscichowski1985No ratings yet
- SG Simplecare Individuals ApplicationDocument8 pagesSG Simplecare Individuals Applicationmanishkpandey07No ratings yet
- k-8 enrollment application 2024-25Document3 pagesk-8 enrollment application 2024-25api-741164195No ratings yet
- Fsa PJB PDFDocument8 pagesFsa PJB PDFMichael Dean RaderNo ratings yet
- Application Form EnglishDocument2 pagesApplication Form EnglishMACENZIE WAKEFIELD0% (1)
- Employment Application FormDocument4 pagesEmployment Application FormMardieNo ratings yet
- Lee County Homelessness Program DetailsDocument5 pagesLee County Homelessness Program DetailsjuanNo ratings yet
- Loan Application FormDocument1 pageLoan Application FormGrely FernandezNo ratings yet
- Company Health Insurance Application: Important InformationDocument8 pagesCompany Health Insurance Application: Important InformationMayar RagabNo ratings yet
- Cholesterol and High Blood Pressure Medical Questionnaire: Important InformationDocument2 pagesCholesterol and High Blood Pressure Medical Questionnaire: Important InformationMayar RagabNo ratings yet
- En - RG CoP 2017 2020 Updated With Changes Errata Dec. 2017 Valid 01.01.2018 PDFDocument83 pagesEn - RG CoP 2017 2020 Updated With Changes Errata Dec. 2017 Valid 01.01.2018 PDFDonna Sheena SaberdoNo ratings yet
- EGY BWHO (24) Member Pack OCT14 (Geo Blue)Document48 pagesEGY BWHO (24) Member Pack OCT14 (Geo Blue)Mayar RagabNo ratings yet
- EGY BWHO (24) Member Pack OCT14 (Geo Blue)Document48 pagesEGY BWHO (24) Member Pack OCT14 (Geo Blue)Mayar RagabNo ratings yet
- Working Conditions of Unorganized Indian WorkersDocument15 pagesWorking Conditions of Unorganized Indian WorkersPiyush DwivediNo ratings yet
- All India Institute of Medical SciencesDocument3 pagesAll India Institute of Medical SciencesNaresh BeatsNo ratings yet
- Poster Clinical Investigation of Magic Ring (Modified Plastibell Device) For CircumcisionDocument1 pagePoster Clinical Investigation of Magic Ring (Modified Plastibell Device) For CircumcisionLutfi Aulia RahmanNo ratings yet
- Rare Case of Sirenomelia Congenital AnomalyDocument3 pagesRare Case of Sirenomelia Congenital Anomalymahesh shindeNo ratings yet
- Uber CEO EmailDocument5 pagesUber CEO EmailKhristopher J. BrooksNo ratings yet
- Talent Management SystemDocument22 pagesTalent Management SystemDeepa Yadav100% (1)
- Can Low-Fat Nutrition Labels Lead To Obesity PDFDocument15 pagesCan Low-Fat Nutrition Labels Lead To Obesity PDFSepti Lidya sariNo ratings yet
- Periprosthetic Joint Infection ISM 2013Document362 pagesPeriprosthetic Joint Infection ISM 2013Andrei Costin100% (1)
- How Does Workplace Stress Affect Job Performance?: An Employee'S PerspectiveDocument6 pagesHow Does Workplace Stress Affect Job Performance?: An Employee'S PerspectiveMacovei DianaNo ratings yet
- HUMAN REPRODUCTION-1 Madhu - QuestionDocument69 pagesHUMAN REPRODUCTION-1 Madhu - QuestionAyan Sarkar100% (1)
- How To Stop Loving Someone Who Doesn't Love You: Part 1 of 4: Giving Yourself SpaceDocument17 pagesHow To Stop Loving Someone Who Doesn't Love You: Part 1 of 4: Giving Yourself SpaceDariz MillerNo ratings yet
- Advancesinlocal Anesthesiain Dentistry: Orrett E. Ogle,, Ghazal MahjoubiDocument19 pagesAdvancesinlocal Anesthesiain Dentistry: Orrett E. Ogle,, Ghazal Mahjoubicarlos gilbertoNo ratings yet
- A Six Step Approach To Writing A Formal SummaryDocument5 pagesA Six Step Approach To Writing A Formal SummaryБезымянный КактусNo ratings yet
- Coronavirus:: Separating The Facts From The FearDocument4 pagesCoronavirus:: Separating The Facts From The FearKhairur RijjalNo ratings yet
- LLM Dissertation TopicsDocument4 pagesLLM Dissertation TopicsPayToDoPaperUK100% (1)
- Drug Law Seminar PaperDocument70 pagesDrug Law Seminar PaperBapulNo ratings yet
- ASCE's Roadmap to Sustainable InfrastructureDocument5 pagesASCE's Roadmap to Sustainable InfrastructureRodolfo De La GarzaNo ratings yet
- Underground Interrogation With Steve CotterDocument12 pagesUnderground Interrogation With Steve CotterTom HillNo ratings yet
- A Case of Possible Hypersensitivity Reactions To Human InsulinDocument6 pagesA Case of Possible Hypersensitivity Reactions To Human Insulingandik danu pramigaNo ratings yet
- COMPENSATION Class 1 PDFDocument5 pagesCOMPENSATION Class 1 PDFpsicologothNo ratings yet
- Business VmvogDocument3 pagesBusiness VmvogAmadea SutandiNo ratings yet
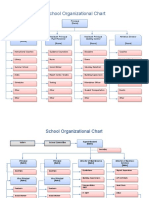
- School Organizational ChartDocument4 pagesSchool Organizational ChartislahNo ratings yet
- Improving Project ProposalsDocument2 pagesImproving Project ProposalsNancy Nicasio SanchezNo ratings yet
- Graded RecitationDocument22 pagesGraded RecitationClara MaeNo ratings yet
- f3 Home-Sci Simplified Notes SPDocument20 pagesf3 Home-Sci Simplified Notes SPmicah isabokeNo ratings yet
- Principles of Monitoring & Evaluation - NotesDocument113 pagesPrinciples of Monitoring & Evaluation - NotesKeith100% (2)
- Cardiology Dr. Payawal UltimateDocument9 pagesCardiology Dr. Payawal UltimateSven OrdanzaNo ratings yet
- Patient's Profile: Doña Remedios Trinidad Romualdez Medical Foundation, Inc. 2 Semester, S.Y. 2020-2021Document16 pagesPatient's Profile: Doña Remedios Trinidad Romualdez Medical Foundation, Inc. 2 Semester, S.Y. 2020-2021Royce Vincent TizonNo ratings yet
- Kaplan: Clinical Chemistry, 5 Edition: Clinical References - Methods of AnalysisDocument9 pagesKaplan: Clinical Chemistry, 5 Edition: Clinical References - Methods of AnalysispudjoNo ratings yet