You might also like
- The Current Relationship Between Surgeon ReimburseDocument4 pagesThe Current Relationship Between Surgeon ReimburseRenan Scalon MachadoNo ratings yet
- Health Care Spending and Quality in Year 1 of The Alternative Quality ContractDocument10 pagesHealth Care Spending and Quality in Year 1 of The Alternative Quality ContractAmira AlhadarNo ratings yet
- The Beginner's Guide To New Health Care Payment Models - BrookingsDocument7 pagesThe Beginner's Guide To New Health Care Payment Models - BrookingsMaca Vera RiveroNo ratings yet
- HPN6Document50 pagesHPN6Joy MichaelNo ratings yet
- Activity Based ManagementDocument26 pagesActivity Based Managementfortune90100% (2)
- Radiology Aco Whitepaper 11-18-14Document9 pagesRadiology Aco Whitepaper 11-18-14api-271257796No ratings yet
- Textbook of Urgent Care Management: Chapter 34, Engaging Accountable Care Organizations in Urgent Care CentersFrom EverandTextbook of Urgent Care Management: Chapter 34, Engaging Accountable Care Organizations in Urgent Care CentersNo ratings yet
- Appropriateness Criteria and Elective Procedures - Total Joint ArthroplastyDocument3 pagesAppropriateness Criteria and Elective Procedures - Total Joint ArthroplastyTruly GracevaNo ratings yet
- Tulsa Memorial Hospital, Santa FE Healthcare, Copperline HealthcareDocument4 pagesTulsa Memorial Hospital, Santa FE Healthcare, Copperline Healthcarealka murarka50% (2)
- Actuarial ObjectiveDocument6 pagesActuarial ObjectiveSumit KhetarpalNo ratings yet
- Orchestrating Physician PreferenceDocument30 pagesOrchestrating Physician PreferenceNeel MehtaNo ratings yet
- European Journal of Operational Research: Ali Vahit Esensoy, Michael W. CarterDocument17 pagesEuropean Journal of Operational Research: Ali Vahit Esensoy, Michael W. Cartertrisya arthaputriNo ratings yet
- AHA Patient Centered Medical HomeDocument21 pagesAHA Patient Centered Medical Homein678No ratings yet
- Accurate Measurement of Financial Toxicity Is A Prerequisite To Finding A RemedyDocument3 pagesAccurate Measurement of Financial Toxicity Is A Prerequisite To Finding A Remedyشهر رمزحنNo ratings yet
- BCG Competing On Outcomes Nov 2013 Tcm80-149649Document0 pagesBCG Competing On Outcomes Nov 2013 Tcm80-149649Yuddy SaputraNo ratings yet
- Custo Efetividade Monitorizacao - 1Document8 pagesCusto Efetividade Monitorizacao - 1André Almeida e SilvaNo ratings yet
- Healthcare Service Lines - The State of The Future by Dr. Jon BurroughsDocument10 pagesHealthcare Service Lines - The State of The Future by Dr. Jon BurroughsAbidi HichemNo ratings yet
- Kiss ADocument22 pagesKiss AJean M Huaman FiallegaNo ratings yet
- 198-Article Text-478-1-10-20210907Document20 pages198-Article Text-478-1-10-20210907juhendNo ratings yet
- A Cost-Consequence Analysis ofDocument10 pagesA Cost-Consequence Analysis ofviviana benavidesNo ratings yet
- Hess 2016Document9 pagesHess 2016kevin gelaudeNo ratings yet
- Team-Based Oncology Care: The Pivotal Role of Oncology NavigationFrom EverandTeam-Based Oncology Care: The Pivotal Role of Oncology NavigationLillie D. ShockneyNo ratings yet
- Unit 6 Discussion 1 Value of The APRN ModelDocument3 pagesUnit 6 Discussion 1 Value of The APRN ModelYash RamawatNo ratings yet
- Health EconomicsDocument26 pagesHealth EconomicsGizem HiçyılmazNo ratings yet
- Information Asymmetry, Insurance, and The Decision To HospitalizeDocument19 pagesInformation Asymmetry, Insurance, and The Decision To HospitalizePunardeep SinghNo ratings yet
- Wound Care Centers: Critical Thinking and Treatment Strategies For WoundsDocument25 pagesWound Care Centers: Critical Thinking and Treatment Strategies For WoundsFooz SroorNo ratings yet
- Neumann 2010Document3 pagesNeumann 2010Afshan GulNo ratings yet
- Response ToDocument7 pagesResponse ToReza AbdarNo ratings yet
- NGR 6813 Hgifford Evidence-Based Paper 7 29 15 FinalDocument22 pagesNGR 6813 Hgifford Evidence-Based Paper 7 29 15 Finalapi-257580555No ratings yet
- Association of Bundled Payments For Joint Replacement Surgery and Patient Outcomes With Simultaneous Hospital Participation in Accountable Care OrganizationsDocument13 pagesAssociation of Bundled Payments For Joint Replacement Surgery and Patient Outcomes With Simultaneous Hospital Participation in Accountable Care OrganizationsMohamed IbrahimNo ratings yet
- Hlthaff 2014 0168Document9 pagesHlthaff 2014 0168Craig WangNo ratings yet
- Benefits of the Australian Triage System /TITLEDocument3 pagesBenefits of the Australian Triage System /TITLEDoaa AwadNo ratings yet
- Art - 2386Document37 pagesArt - 2386Kumar palNo ratings yet
- AHA BundledPayment ReportDocument20 pagesAHA BundledPayment Reportbikram2128100% (1)
- The Hospital Is Dead, Long Live The Hospital! - McKinseyDocument22 pagesThe Hospital Is Dead, Long Live The Hospital! - McKinseyYanto Sandy TjangNo ratings yet
- Acumen Medicare MedicaidDocument184 pagesAcumen Medicare MedicaidAgeNo ratings yet
- Casemix and Information Systems: Health InformaticsDocument24 pagesCasemix and Information Systems: Health InformaticsAchmad yudi ArifiyantoNo ratings yet
- The New Hospital-Physician Enterprise: Meeting the Challenges of Value-Based CareFrom EverandThe New Hospital-Physician Enterprise: Meeting the Challenges of Value-Based CareNo ratings yet
- Costs of Health Care Across Primary Care Models in Ontario: ResearcharticleDocument9 pagesCosts of Health Care Across Primary Care Models in Ontario: ResearcharticleAswarNo ratings yet
- High Value Physician Guide - 2010!10!1Document12 pagesHigh Value Physician Guide - 2010!10!1Jennifer ChristianNo ratings yet
- Jurnalsjw 138Document10 pagesJurnalsjw 138RadenSiwi Bagus HadhiningratNo ratings yet
- A Very Interesting Read About Disease-Specific Costing GuidelineDocument10 pagesA Very Interesting Read About Disease-Specific Costing GuidelineJeisson MorenoNo ratings yet
- How To Determine Cost Effective Analysis - RatikaDocument14 pagesHow To Determine Cost Effective Analysis - Ratikatifanny carolinaNo ratings yet
- Medicare DataDocument68 pagesMedicare DataNicolas CNo ratings yet
- Using Pragmatic Clinical Trials To Test The Effectiveness of Patient-Centered Medical Home Models in Real-World Settings PCMH Research Methods SeriesDocument11 pagesUsing Pragmatic Clinical Trials To Test The Effectiveness of Patient-Centered Medical Home Models in Real-World Settings PCMH Research Methods SeriesJames LindonNo ratings yet
- Journal of Operations Management: Deepa Wani, Manoj Malhotra, Sriram VenkataramanDocument13 pagesJournal of Operations Management: Deepa Wani, Manoj Malhotra, Sriram VenkataramanSarah WaichertNo ratings yet
- Evidence Based RUADocument12 pagesEvidence Based RUAAsma AliNo ratings yet
- The Utilization of Hospitalists Associated With Compensation: Insourcing Instead of Outsourcing Health CareDocument10 pagesThe Utilization of Hospitalists Associated With Compensation: Insourcing Instead of Outsourcing Health Careadrian_badriNo ratings yet
- Jope 38 SDocument6 pagesJope 38 SRhyka AchmadNo ratings yet
- Health Policy Brief: Accountable Care OrganizationsDocument6 pagesHealth Policy Brief: Accountable Care Organizationspalak32No ratings yet
- How An Urgent Care Service Line Can Benefit A Multi-Specialty PracticeDocument21 pagesHow An Urgent Care Service Line Can Benefit A Multi-Specialty PracticeAbidi HichemNo ratings yet
- Hayward EvaluationGenericScreens 1993Document10 pagesHayward EvaluationGenericScreens 1993Dauna Apriansa Anggoro PutriNo ratings yet
- Primary Care Impact On Health Outcomes A Literature ReviewDocument6 pagesPrimary Care Impact On Health Outcomes A Literature Reviewm1dyhuh1jud2No ratings yet
- Utilization Management in A Large Urban Academic Medical CenterDocument11 pagesUtilization Management in A Large Urban Academic Medical CenterMELYANo ratings yet
- Comprehensive Health Care Reform and Biomedical InnovationDocument21 pagesComprehensive Health Care Reform and Biomedical InnovationcashelNo ratings yet
- Benefit of Multidisciplinary Wound Care Center On The Volume and Outcomes of A Vascular Surgery PracticeDocument8 pagesBenefit of Multidisciplinary Wound Care Center On The Volume and Outcomes of A Vascular Surgery PracticeCandace LongNo ratings yet
- Comprehensive Care PhysicianDocument9 pagesComprehensive Care PhysiciannurNo ratings yet
- Strategies to Explore Ways to Improve Efficiency While Reducing Health Care CostsFrom EverandStrategies to Explore Ways to Improve Efficiency While Reducing Health Care CostsNo ratings yet
- Asa 2013Document1,076 pagesAsa 2013Marwa Mahrous100% (4)
- 0000542-200203000-00031 HospitalDocument7 pages0000542-200203000-00031 HospitalVivek PandeyNo ratings yet
- Pi Is 1548559519301144Document20 pagesPi Is 1548559519301144hemer hadyn calderon alvites0% (1)
- Improving Palliative Care For Patients in The Intensive Care UnitDocument12 pagesImproving Palliative Care For Patients in The Intensive Care UnitLuke Wolfstein HidetoraNo ratings yet
- Minimal Spatial Heterogeneity in Chronic Lymphocytic Leukemia at DiagnosisDocument5 pagesMinimal Spatial Heterogeneity in Chronic Lymphocytic Leukemia at DiagnosisLuke Wolfstein HidetoraNo ratings yet
- Preface Preoperativepatientevaluation: Practicingevidence-Based, Cost-EffectivemedicineDocument2 pagesPreface Preoperativepatientevaluation: Practicingevidence-Based, Cost-EffectivemedicineLuke Wolfstein HidetoraNo ratings yet
- Practice Management: Opportunities and ChallengesDocument3 pagesPractice Management: Opportunities and ChallengesLuke Wolfstein HidetoraNo ratings yet
- Higher Primary Care Physician Continuity Is Associated With Lower Costs and HospitalizationsDocument6 pagesHigher Primary Care Physician Continuity Is Associated With Lower Costs and HospitalizationsLuke Wolfstein HidetoraNo ratings yet
- Nicotinic Receptor Subtypes and Cognitive Function: Edward D. LevinDocument8 pagesNicotinic Receptor Subtypes and Cognitive Function: Edward D. LevinJeffery McDonaldNo ratings yet
- 2019 American Dental Association. All Rights ReservedDocument1 page2019 American Dental Association. All Rights ReservedLuke Wolfstein HidetoraNo ratings yet
- Value-Based Oral Health Care: Moving Forward With Dental Patient-Reported OutcomesDocument5 pagesValue-Based Oral Health Care: Moving Forward With Dental Patient-Reported OutcomesLuke Wolfstein HidetoraNo ratings yet
- Value-Based Mental Healthcare: The Quality Aspect Value-Based Mental Healthcare: The Cost AspectDocument1 pageValue-Based Mental Healthcare: The Quality Aspect Value-Based Mental Healthcare: The Cost AspectLuke Wolfstein HidetoraNo ratings yet
- Jurnal Kedokteran Dan Kesehatan IndonesiaDocument10 pagesJurnal Kedokteran Dan Kesehatan IndonesiaLuke Wolfstein HidetoraNo ratings yet
- Nicotinic Receptor Subtypes and Cognitive Function: Edward D. LevinDocument8 pagesNicotinic Receptor Subtypes and Cognitive Function: Edward D. LevinJeffery McDonaldNo ratings yet
- Vector Borne Action Plan-2017Document49 pagesVector Borne Action Plan-2017Luke Wolfstein HidetoraNo ratings yet
- Atmosphere 09 00385 v2Document60 pagesAtmosphere 09 00385 v2Luke Wolfstein HidetoraNo ratings yet
- 10 1016@j Exger 2018 11 002Document6 pages10 1016@j Exger 2018 11 002Luke Wolfstein HidetoraNo ratings yet
- Presentation 210716Document17 pagesPresentation 210716Luke Wolfstein HidetoraNo ratings yet
- Levy 2018Document11 pagesLevy 2018Luke Wolfstein HidetoraNo ratings yet
- 2 PBDocument10 pages2 PBLuke Wolfstein HidetoraNo ratings yet
- Irreducible Fracture-Dislocations of The Femoral Head Without Posterior Wall Acetabular FracturesDocument7 pagesIrreducible Fracture-Dislocations of The Femoral Head Without Posterior Wall Acetabular Fracturesakb601No ratings yet
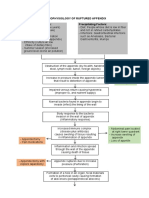
- Pathophysiology of Ruptured AppendixDocument2 pagesPathophysiology of Ruptured AppendixAya PaquitNo ratings yet
- Rehabilitation of The Hand and Upper Extremity 2 Volume Set e Book Expert Consult 6th Edition Ebook PDFDocument62 pagesRehabilitation of The Hand and Upper Extremity 2 Volume Set e Book Expert Consult 6th Edition Ebook PDFsummer.yates611100% (40)
- Georgina Tracey Veterinary Nursing, Fetac Level 6Document8 pagesGeorgina Tracey Veterinary Nursing, Fetac Level 6Georgie TraceyNo ratings yet
- Hasson & Wong Lateral Slit TechniqueDocument7 pagesHasson & Wong Lateral Slit Techniquerl20No ratings yet
- Chap 2 THE SUTUREDocument30 pagesChap 2 THE SUTUREhuyenthanh1807No ratings yet
- Physio After SurgeryDocument2 pagesPhysio After SurgeryGursangeet KaurNo ratings yet
- Can Robotics Increase The Rate of Unemployment in Hospitals in The FutureDocument9 pagesCan Robotics Increase The Rate of Unemployment in Hospitals in The Futureapi-462519362No ratings yet
- Customer Satisfaction in HospitalsDocument23 pagesCustomer Satisfaction in HospitalsanilsumanNo ratings yet
- Medicare Claims Processing Manual: Chapter 12 - Physicians/Nonphysician PractitionersDocument185 pagesMedicare Claims Processing Manual: Chapter 12 - Physicians/Nonphysician PractitionersPimo HypkaNo ratings yet
- PID L4-L5 (Case Study)Document67 pagesPID L4-L5 (Case Study)NannieNo ratings yet
- DOFA Analysis of Plastic Surgeries in ColombiaDocument2 pagesDOFA Analysis of Plastic Surgeries in ColombiaHarol EscalanteNo ratings yet
- High Output Enterocutaneous Fistula (Case Study) 2011Document6 pagesHigh Output Enterocutaneous Fistula (Case Study) 2011Joon RaynerNo ratings yet
- Lecturer: Hemn Kareem Qadir Fundamentals of Nursing Lec. 1Document2 pagesLecturer: Hemn Kareem Qadir Fundamentals of Nursing Lec. 1Karwan DilmanyNo ratings yet
- Forever Living Product TestimoniesDocument9 pagesForever Living Product TestimoniesGurmeet Singh RajpalNo ratings yet
- Effectiveness of Myofunctional Therapy in Ankyloglossia: A Systematic ReviewDocument18 pagesEffectiveness of Myofunctional Therapy in Ankyloglossia: A Systematic Reviewmistic0No ratings yet
- The Pedicled TRAM Flap in Breast ReconstructionDocument22 pagesThe Pedicled TRAM Flap in Breast ReconstructionJose Mauricio Suarez BecerraNo ratings yet
- 23-Discharge Against Medical Advice (Dama)Document3 pages23-Discharge Against Medical Advice (Dama)akositabonNo ratings yet
- Rundown Iaca 7Document2 pagesRundown Iaca 7Muh Anugerah YusroNo ratings yet
- An Atlas of Head and Neck Images Part I 2002 Atlas of The Oral and Maxillofacial Surgery ClinicsDocument2 pagesAn Atlas of Head and Neck Images Part I 2002 Atlas of The Oral and Maxillofacial Surgery ClinicsMohammed Qasim Al-WataryNo ratings yet
- 2010 SanctionsDocument38 pages2010 Sanctionsgiyasay671No ratings yet
- Perioperative NursingDocument9 pagesPerioperative NursingLouie Kem Anthony BabaranNo ratings yet
- BBA Timetable V17Document11 pagesBBA Timetable V17Alisa Sharen AssyfaNo ratings yet
- Post Op Alveoloplasty - RRR - 1 PDFDocument1 pagePost Op Alveoloplasty - RRR - 1 PDFAndykaYayanSetiawanNo ratings yet
- Absolute GlaucomaDocument12 pagesAbsolute GlaucomaPaulus AnungNo ratings yet
- Nejm 09-04-2015Document107 pagesNejm 09-04-2015Javier B GreenNo ratings yet
- Orthopaedics KardexDocument16 pagesOrthopaedics KardexLuisaTsinaLehNo ratings yet
- What Is Microsurgical Tubal Ligation Reversal?Document2 pagesWhat Is Microsurgical Tubal Ligation Reversal?Andy WijayaNo ratings yet
- Jurnal Teori NigtingaleDocument4 pagesJurnal Teori NigtingaleUmi AsyrafiNo ratings yet
- Entropion and Ectropion Repair: BackgroundDocument10 pagesEntropion and Ectropion Repair: BackgroundDiaz RandanilNo ratings yet