You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5814)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (845)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Warrior Cardio - The Revolutionary Metabo - Rooney, MartinDocument6 pagesWarrior Cardio - The Revolutionary Metabo - Rooney, MartinMila AS33% (6)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- CXR ABC by DR ShamolDocument139 pagesCXR ABC by DR Shamolazar103100% (3)
- COVID - English Final PDFDocument2 pagesCOVID - English Final PDFazar103No ratings yet
- TNSOP 6 Clinical GuidelinesDocument14 pagesTNSOP 6 Clinical Guidelinesazar103No ratings yet
- TNSOP 4 Home Care PDFDocument1 pageTNSOP 4 Home Care PDFazar103No ratings yet
- TNSOP 2 Sample Collection PDFDocument4 pagesTNSOP 2 Sample Collection PDFazar103No ratings yet
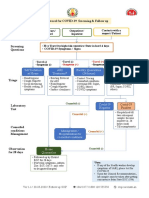
- Protocol For COVID 19 Screening and Followup PDFDocument1 pageProtocol For COVID 19 Screening and Followup PDFazar103No ratings yet
- Contact Follow Up: Identify Contacts of Lab Confirmed COVID-19 Patients by District EOC (Use FORM 3A)Document1 pageContact Follow Up: Identify Contacts of Lab Confirmed COVID-19 Patients by District EOC (Use FORM 3A)azar103No ratings yet
- Awareness About Tooth Extraction Among General Public A SurveyDocument9 pagesAwareness About Tooth Extraction Among General Public A SurveyInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- JLO 310 PPT Presentation Objectives SWDocument5 pagesJLO 310 PPT Presentation Objectives SWThando MbathaNo ratings yet
- Dap ManualDocument31 pagesDap Manualnesuma100% (1)
- SAMPLE-GER0107PAI - Stimulant Abuse Deterrents and Treatments - 2018Document24 pagesSAMPLE-GER0107PAI - Stimulant Abuse Deterrents and Treatments - 2018anon_448322966No ratings yet
- Ferreira Marques: Portuguese Lawyer & Free ManDocument6 pagesFerreira Marques: Portuguese Lawyer & Free ManJavier NessNo ratings yet
- General BooksDocument122 pagesGeneral BooksZora DNo ratings yet
- Vaccine Declaration COVID 19Document2 pagesVaccine Declaration COVID 19Kyla NguyenNo ratings yet
- Unit-2 Soft Skills For Professional ExcellenceDocument10 pagesUnit-2 Soft Skills For Professional Excellencebot284919No ratings yet
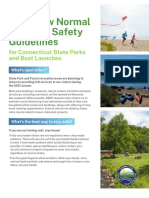
- DEEP FlyerDocument2 pagesDEEP FlyerPeter YankowskiNo ratings yet
- Instruction Sheet: Bruise/Hematoma: University of North Carolina Wilmington Abrons Student Health CenterDocument1 pageInstruction Sheet: Bruise/Hematoma: University of North Carolina Wilmington Abrons Student Health CenterRoman CoNo ratings yet
- When Love and Science Double Date (In)Document1 pageWhen Love and Science Double Date (In)Pepito perezNo ratings yet
- Orthodontic Learning Curve: A Journey We All MakeDocument2 pagesOrthodontic Learning Curve: A Journey We All MakeeltonNo ratings yet
- Tph204 Medical DeclarationDocument12 pagesTph204 Medical DeclarationshafiqullahhashumiNo ratings yet
- Science Investigatory ProjectDocument7 pagesScience Investigatory Project카밀카밀No ratings yet
- Lesson1structureandfunction Circulatorysystem 140718072518 Phpapp01Document45 pagesLesson1structureandfunction Circulatorysystem 140718072518 Phpapp01Richel Escalante MaglunsodNo ratings yet
- The Two Part Film Technique Empowering DDocument19 pagesThe Two Part Film Technique Empowering DmonpsyNo ratings yet
- IPT ScriptDocument4 pagesIPT ScriptDiana Jennieve TuzonNo ratings yet
- Long Quiz in PE and Health 12Document2 pagesLong Quiz in PE and Health 12Diana San DiegoNo ratings yet
- Focus Charting On Sepsis NeonatorumDocument1 pageFocus Charting On Sepsis NeonatorumDhanNie CenitaNo ratings yet
- Analysis of Jasola Gaon by RamshaDocument67 pagesAnalysis of Jasola Gaon by RamshaArisha NusratNo ratings yet
- 05-00000271 Step I 20230511094814Document2 pages05-00000271 Step I 20230511094814Sonia Ibanez OrenciadaNo ratings yet
- Jet, Ultrasonic, and Mesh Nebulizers: An Evaluation of Nebulizers For Better Clinical OutcomesDocument7 pagesJet, Ultrasonic, and Mesh Nebulizers: An Evaluation of Nebulizers For Better Clinical OutcomesShabilah Novia SNo ratings yet
- Hulskamp, M.A.A. 08Document297 pagesHulskamp, M.A.A. 08Henry LopesNo ratings yet
- Oxygen DepletionDocument12 pagesOxygen DepletionAhsan AliNo ratings yet
- Ficha de AvaliacaoDocument28 pagesFicha de AvaliacaosanlaypossoliaestheticNo ratings yet
- EEG Sleep StagingDocument5 pagesEEG Sleep StagingIstiaqAnsariRakibNo ratings yet
- Exam Based On Unit 1Document2 pagesExam Based On Unit 1ALS Amr Shakir AlDeebNo ratings yet
- Normative Data For Ten Spanish-Language Neuropsychological Tests in Eleven Latin American Countries PDFDocument239 pagesNormative Data For Ten Spanish-Language Neuropsychological Tests in Eleven Latin American Countries PDFNicol Mariana V. FernándezNo ratings yet
- HOANG HOA THAM Junior High School HKII G9Document3 pagesHOANG HOA THAM Junior High School HKII G9Hien TranNo ratings yet