You might also like
- Tom Grant Case ManualDocument136 pagesTom Grant Case Manualdozydory100% (3)
- Sample Eligibility FormsDocument26 pagesSample Eligibility Formsapi-241173571100% (1)
- Storm Water Pump StationDocument6 pagesStorm Water Pump StationНемања КараклајићNo ratings yet
- Installation, Operation and Maintenance - LOK-FLANGE ® Multitube Heat ExchangersDocument5 pagesInstallation, Operation and Maintenance - LOK-FLANGE ® Multitube Heat ExchangersCLIFFORDPANo ratings yet
- The Care, Core, Cure Theory - Lydia HallDocument3 pagesThe Care, Core, Cure Theory - Lydia HallEzraRamosLambarte0% (1)
- SONY Z MechanismDocument64 pagesSONY Z MechanismHarinarayana ChennupatiNo ratings yet
- Diabetes DietDocument8 pagesDiabetes DietkitchaaNo ratings yet
- Teaching Plan For Diabetes MellitusDocument5 pagesTeaching Plan For Diabetes MellitusWebster Claveria100% (5)
- Basics of Oil AnalysisDocument21 pagesBasics of Oil Analysisvalerie.sch67% (3)
- Food Insulin IndexDocument14 pagesFood Insulin IndexSharanyMustafa100% (1)
- Nutrition Therapy For Diabetes Effectiveness Carbohydrates and AlcoholDocument12 pagesNutrition Therapy For Diabetes Effectiveness Carbohydrates and Alcoholscience lulNo ratings yet
- Eapp q2 Module 9Document21 pagesEapp q2 Module 9Edsel Hormachuelas100% (1)
- Cell InjuryDocument46 pagesCell Injuryeri_tariganNo ratings yet
- J Clin Endocrinol Metab. 2012 97 16 38Document23 pagesJ Clin Endocrinol Metab. 2012 97 16 38rizwan234No ratings yet
- 823 FullDocument5 pages823 FullPencari IlmuNo ratings yet
- Carbohydrate To Insulin Ratio - Breakfast-Lunch-DinnerDocument5 pagesCarbohydrate To Insulin Ratio - Breakfast-Lunch-Dinnermario rodriguezNo ratings yet
- 膳食碳水化合物摄入量与新发糖尿病:中国全国性队列研究Document8 pages膳食碳水化合物摄入量与新发糖尿病:中国全国性队列研究张芬No ratings yet
- Effects of Advanced Carbohydrate Counting On Glucose Control and QolDocument9 pagesEffects of Advanced Carbohydrate Counting On Glucose Control and QollloplNo ratings yet
- Oce Guera 2016Document6 pagesOce Guera 2016Anonymous 1EQutBNo ratings yet
- Insulin Pump Therapy in Children and Adolescents - Improvements in Key Parameters of Diabetes Management Including Quality of LifeDocument5 pagesInsulin Pump Therapy in Children and Adolescents - Improvements in Key Parameters of Diabetes Management Including Quality of Lifeasdv eqdNo ratings yet
- Timing of Insulin Injections Adherence and GlycemiDocument12 pagesTiming of Insulin Injections Adherence and GlycemiOlesiaNo ratings yet
- T1DM Commentary Pediatrics 2018Document4 pagesT1DM Commentary Pediatrics 2018GlowstarNo ratings yet
- Jakoby2011 PROTOCOLODocument6 pagesJakoby2011 PROTOCOLOMau MillanNo ratings yet
- Diabetic Medicine - 2022 - Speight - Impact of Glycaemic Technologies On Quality of Life and Related Outcomes in AdultsDocument23 pagesDiabetic Medicine - 2022 - Speight - Impact of Glycaemic Technologies On Quality of Life and Related Outcomes in AdultsBogi VargaNo ratings yet
- Egyptian Pediatric Association Gazette: M.H. Elsamahy, Y.I. Elhenawy, N. AltayebDocument5 pagesEgyptian Pediatric Association Gazette: M.H. Elsamahy, Y.I. Elhenawy, N. Altayebida ayu agung WijayantiNo ratings yet
- V Diabetic Medicine - 2009 - Smart - Children and Adolescents On Intensive Insulin Therapy Maintain Postprandial GlycaemicDocument7 pagesV Diabetic Medicine - 2009 - Smart - Children and Adolescents On Intensive Insulin Therapy Maintain Postprandial GlycaemicReeds LaurelNo ratings yet
- Snorgaard CHO Restriction Patients DM2Document10 pagesSnorgaard CHO Restriction Patients DM2GracielaRecheNo ratings yet
- Ef Ficacy of An Education Program For People With Diabetes and Insulin Pump Treatment (INPUT) : Results From A Randomized Controlled TrialDocument10 pagesEf Ficacy of An Education Program For People With Diabetes and Insulin Pump Treatment (INPUT) : Results From A Randomized Controlled TrialadddNo ratings yet
- Effects of Yoga in Adults With Type 2 Diabetes Mellitus: A Meta-AnalysisDocument9 pagesEffects of Yoga in Adults With Type 2 Diabetes Mellitus: A Meta-AnalysisPerez Wahyu PurnasariNo ratings yet
- Ajuste Con Dosis PreviasDocument23 pagesAjuste Con Dosis PreviasOscar AlfonsoNo ratings yet
- Flexible Intensive Insulin Therapy: Practical Modalities and Metabolic ImpactDocument5 pagesFlexible Intensive Insulin Therapy: Practical Modalities and Metabolic ImpactIJAR JOURNALNo ratings yet
- Fphys 13 960580Document13 pagesFphys 13 960580غاز الشمالNo ratings yet
- Analysis: Hypoglycemia As An Indicator of Good Diabetes CareDocument4 pagesAnalysis: Hypoglycemia As An Indicator of Good Diabetes CareEmanuel BaltigNo ratings yet
- Https:/zero Sci-Hub Se/5089//boulet2016Document10 pagesHttps:/zero Sci-Hub Se/5089//boulet2016Caroline QueirogaNo ratings yet
- Endocrinology Diabetes702Document7 pagesEndocrinology Diabetes702Phelix O DaniyanNo ratings yet
- Dabetes InglesDocument10 pagesDabetes InglesIsabelNo ratings yet
- Diabetes Artigo 04Document19 pagesDiabetes Artigo 04Júlio EpifanioNo ratings yet
- Dia 2017 2525 AbstractsDocument134 pagesDia 2017 2525 AbstractsPranav Kumar Prabhakar100% (1)
- Treatment of Patients With Type 1 Diabetes Insulin Pumps or Multiple Injections 2016 Biocybernetics and Biomedical EngineeringDocument8 pagesTreatment of Patients With Type 1 Diabetes Insulin Pumps or Multiple Injections 2016 Biocybernetics and Biomedical EngineeringJose J.No ratings yet
- Blood Glucose DexamethasoneDocument12 pagesBlood Glucose DexamethasoneArifa LainaNo ratings yet
- Diabetes Reversal by Plant Based Diet Dr. BiswaroopDocument7 pagesDiabetes Reversal by Plant Based Diet Dr. Biswaroopsatya_vanapalli3422100% (1)
- SLIDE JURNAL DHR MTDocument29 pagesSLIDE JURNAL DHR MTTenyson AnalauwNo ratings yet
- 02.WS Glimepiride Padang LaksmiDocument32 pages02.WS Glimepiride Padang LaksmiDinda YusditiraNo ratings yet
- Type 1 Diabetes MellitusDocument10 pagesType 1 Diabetes Mellitusayu permata dewiNo ratings yet
- Why Is Premixed Insulin The Preferred Insulin? Novel Answers To A Decade-Old QuestionDocument3 pagesWhy Is Premixed Insulin The Preferred Insulin? Novel Answers To A Decade-Old QuestionDanielShenfieldNo ratings yet
- Beck 2017 Effect of Continuous Glucose Monitoring On Glycemic Control in AdultsDocument8 pagesBeck 2017 Effect of Continuous Glucose Monitoring On Glycemic Control in AdultschoouleleNo ratings yet
- 2Document8 pages2Claudia NgNo ratings yet
- Jama Beck 2017 Oi 160152Document8 pagesJama Beck 2017 Oi 160152Athaya YuflihNo ratings yet
- Jurnal EpidDocument6 pagesJurnal EpidLalaNo ratings yet
- Management of Hyperglycemia in Critical Care.5Document10 pagesManagement of Hyperglycemia in Critical Care.5nicho927No ratings yet
- Insulin Detemir and Basal Insulin TherapyDocument7 pagesInsulin Detemir and Basal Insulin Therapymayrapp16No ratings yet
- PJMS 38 992Document6 pagesPJMS 38 992Nur WahyuniNo ratings yet
- Systematic Review and Meta-Analysis of Dietary Carbohydrate Restriction in Patients With Type 2 DiabetesDocument11 pagesSystematic Review and Meta-Analysis of Dietary Carbohydrate Restriction in Patients With Type 2 DiabetesLaah PhaanxhiithaahNo ratings yet
- c3 Type 1 Diabetes MellitusDocument10 pagesc3 Type 1 Diabetes Mellitusjulio perezNo ratings yet
- 614 FullDocument11 pages614 Full31271111No ratings yet
- Burs Lem 2021Document13 pagesBurs Lem 2021ERINSONNo ratings yet
- Clinical Nutrition Course: "Let Food Be Thy Medicine" - HippocratesDocument31 pagesClinical Nutrition Course: "Let Food Be Thy Medicine" - HippocratesAbhishek ThakurNo ratings yet
- Eckert 2021Document10 pagesEckert 2021Igor EckertNo ratings yet
- Fpubh 11 1078361Document6 pagesFpubh 11 1078361Оксана КожокаруNo ratings yet
- Effect Cocoa Dark Chocolate Consump Lipid Profile Glycemia BloodDocument15 pagesEffect Cocoa Dark Chocolate Consump Lipid Profile Glycemia BloodEliseia CarvalhoNo ratings yet
- Tests of Glycemia in Diabetes: D E. G, R R. L, R A. L, J I. M, D N, C M. P, D B. SDocument13 pagesTests of Glycemia in Diabetes: D E. G, R R. L, R A. L, J I. M, D N, C M. P, D B. Sfebriyani dyahNo ratings yet
- JCEM Diabetes in Pregnancy 2013Document23 pagesJCEM Diabetes in Pregnancy 2013Ann DahngNo ratings yet
- 2 Year Remission of Type 2 Diabetes and Pancreas MDocument10 pages2 Year Remission of Type 2 Diabetes and Pancreas Mgipokratik5No ratings yet
- Post-Transplant Diabetes MellitusDocument4 pagesPost-Transplant Diabetes MellitusSarah Gita SinagaNo ratings yet
- Does Minimed 780G Insulin Pump System Affect Energy and Nutrient Intake?: Long-Term Follow-Up StudyDocument7 pagesDoes Minimed 780G Insulin Pump System Affect Energy and Nutrient Intake?: Long-Term Follow-Up StudyDaniel VazquezNo ratings yet
- Index of C-Peptide Glucose Ratio For Carbo70 Can Be Usefeul in Clinical Practice For DiabetesDocument4 pagesIndex of C-Peptide Glucose Ratio For Carbo70 Can Be Usefeul in Clinical Practice For DiabetesSTBz09No ratings yet
- Gut Hormones and Appetite Control: A Focus On PYY and GLP-1 As Therapeutic Targets in ObesityDocument11 pagesGut Hormones and Appetite Control: A Focus On PYY and GLP-1 As Therapeutic Targets in ObesityMIIIBNo ratings yet
- ISPAD Clinical Practice Consensus Guidelines 2018: Exercise in Children and Adolescents With DiabetesDocument22 pagesISPAD Clinical Practice Consensus Guidelines 2018: Exercise in Children and Adolescents With Diabetesdesak indryNo ratings yet
- Outsmarting Diabetes: A Dynamic Approach for Reducing the Effects of Insulin-Dependent DiabetesFrom EverandOutsmarting Diabetes: A Dynamic Approach for Reducing the Effects of Insulin-Dependent DiabetesRating: 3.5 out of 5 stars3.5/5 (3)
- Wait Times To Medical Care and Treatment in Canada: LAWS-6046 - (34) - 22S - Emily PassanhaDocument10 pagesWait Times To Medical Care and Treatment in Canada: LAWS-6046 - (34) - 22S - Emily Passanhaemily passanhaNo ratings yet
- MatthewpiccolinocvDocument6 pagesMatthewpiccolinocvapi-485639349No ratings yet
- Pages From SAES-H-001-12Document1 pagePages From SAES-H-001-12mohammed s fawabNo ratings yet
- CM HPS: Legend: Cable by JLM: Cable by CimcDocument1 pageCM HPS: Legend: Cable by JLM: Cable by CimcMd Abu BorhanNo ratings yet
- Use of Saga Leaves (Abrus Precatorius) As An Alternative Medicine To Help Treat in The Kampung Cisimeut Kecamatan Leuwidamar RT 002 RW 002Document6 pagesUse of Saga Leaves (Abrus Precatorius) As An Alternative Medicine To Help Treat in The Kampung Cisimeut Kecamatan Leuwidamar RT 002 RW 002HiilyahNo ratings yet
- Revision - 3Document2 pagesRevision - 3Abhinand PrakashNo ratings yet
- Hf1016414 Hoffman VentiladorDocument4 pagesHf1016414 Hoffman VentiladorMoises AlvarezNo ratings yet
- Parenting Education Literacy Position Paper 2014-07-18Document4 pagesParenting Education Literacy Position Paper 2014-07-18Shreya SharmaNo ratings yet
- Basic Organic Chemistry and Mechanisms Revision From M Wills For When You Are Lost and ConfusedDocument128 pagesBasic Organic Chemistry and Mechanisms Revision From M Wills For When You Are Lost and ConfusedJasim Al-rufayeNo ratings yet
- Evaluation Test T Lo IDocument10 pagesEvaluation Test T Lo IHậu NguyễnNo ratings yet
- RA10354 PrimerDocument24 pagesRA10354 PrimerFloreen SimonNo ratings yet
- Aas - Perkin Elmer Aa800 User-GuideDocument175 pagesAas - Perkin Elmer Aa800 User-GuideFlorin MuselinNo ratings yet
- EPR and Silicon CatalogueDocument6 pagesEPR and Silicon CatalogueHarshad ChauhanNo ratings yet
- Chemistry Unit 5 Part 2Document80 pagesChemistry Unit 5 Part 2Will AndyNo ratings yet
- GR 1749 - People Vs OdictaDocument4 pagesGR 1749 - People Vs OdictaJing DalaganNo ratings yet
- Research - Chapters 123 - GO John Carl OkDocument16 pagesResearch - Chapters 123 - GO John Carl OkAlvaro Jasmine KateNo ratings yet
- FamilyDocument9 pagesFamilyharikumarrmNo ratings yet
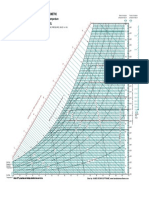
- Carta Sicrometrica A Nivel Del MarDocument1 pageCarta Sicrometrica A Nivel Del MarEstebanCórdobaNo ratings yet
- Chapter 2 Sexual Reproduction in Flowering Plants PART-I MCQsDocument18 pagesChapter 2 Sexual Reproduction in Flowering Plants PART-I MCQslosliya vinayNo ratings yet
- Water ResearchDocument13 pagesWater ResearchmicahelNo ratings yet
- Manipis 2024 Agriculturalwastemgt Project ProfileDocument8 pagesManipis 2024 Agriculturalwastemgt Project ProfileDebah Diaz Baclayon WaycoNo ratings yet