You might also like
- Debbie Corso - Stronger Than BPDDocument96 pagesDebbie Corso - Stronger Than BPDKalil100% (2)
- Global Population and Mobility RevisedDocument39 pagesGlobal Population and Mobility RevisedJan Kenneth Pancho100% (1)
- A Pragmatic View of Thematic AnalysisDocument5 pagesA Pragmatic View of Thematic AnalysisLouis SpencerNo ratings yet
- COSHH Assessment TemplateDocument2 pagesCOSHH Assessment TemplaterichardNo ratings yet
- DysgraphiaDocument7 pagesDysgraphiaTehseen Khan100% (1)
- Ravi Kannaiyan: QC Inspection EngineerDocument5 pagesRavi Kannaiyan: QC Inspection EngineerVinoth BalaNo ratings yet
- Cleaningvssanitizingservsafe1583366413072 PDFDocument2 pagesCleaningvssanitizingservsafe1583366413072 PDFHenry SNo ratings yet
- Running Head: MIAH ZAVARRO V3 Miah Zavarro V3 Name Course Institution DateDocument4 pagesRunning Head: MIAH ZAVARRO V3 Miah Zavarro V3 Name Course Institution DateSammy Chege100% (1)
- Herder-Farmer Conflicts in South East Nigeria: Assessing The DangersDocument8 pagesHerder-Farmer Conflicts in South East Nigeria: Assessing The DangersThe Wilson CenterNo ratings yet
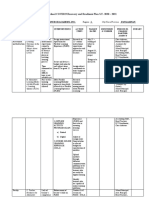
- ESC-GASTPE School COVID19 Recovery and Readiness Plan S.Y. 2020 - 2021Document5 pagesESC-GASTPE School COVID19 Recovery and Readiness Plan S.Y. 2020 - 2021Jubylyn Aficial100% (3)
- Meaning of Self-Esteem: by Dr. Ranjit Singh MalhiDocument2 pagesMeaning of Self-Esteem: by Dr. Ranjit Singh Malhieva pandanaNo ratings yet
- Migrant Women and Women in The Informal SectorDocument13 pagesMigrant Women and Women in The Informal SectorKimberly ValsoteNo ratings yet
- 90021-Article Text-225688-1-10-20130701Document36 pages90021-Article Text-225688-1-10-20130701chalaNo ratings yet
- Slavery and Its Impact On People of African DecentDocument8 pagesSlavery and Its Impact On People of African DecentMinahil AzeemNo ratings yet
- The Philippines: Globalization and MigrationDocument6 pagesThe Philippines: Globalization and MigrationDexter LagrimasNo ratings yet
- HIV/AIDS: A Rural Issue: of The 36,1 Million People Living With HIV/AIDS, An Overwhelming 95 Percent LiveDocument7 pagesHIV/AIDS: A Rural Issue: of The 36,1 Million People Living With HIV/AIDS, An Overwhelming 95 Percent LiveRavi MothoorNo ratings yet
- Male MigrationDocument8 pagesMale MigrationnamitaNo ratings yet
- Comment On The View That The Transatlantic Slave Trade Was A Mixed Blessing For AfricaDocument8 pagesComment On The View That The Transatlantic Slave Trade Was A Mixed Blessing For AfricaJonathanNo ratings yet
- Challenges To Security, Livelihoods, and Gender Justice in South SudanDocument50 pagesChallenges To Security, Livelihoods, and Gender Justice in South SudanOxfamNo ratings yet
- Challenges To Security, Livelihoods, and Gender Justice in South SudanDocument50 pagesChallenges To Security, Livelihoods, and Gender Justice in South SudanOxfamNo ratings yet
- Challenges To Security, Livelihoods, and Gender Justice in South SudanDocument50 pagesChallenges To Security, Livelihoods, and Gender Justice in South SudanOxfamNo ratings yet
- Challenges To Security, Livelihoods, and Gender Justice in South SudanDocument50 pagesChallenges To Security, Livelihoods, and Gender Justice in South SudanOxfamNo ratings yet
- Challenges To Security, Livelihoods, and Gender Justice in South SudanDocument50 pagesChallenges To Security, Livelihoods, and Gender Justice in South SudanOxfamNo ratings yet
- 43571-Article Text-40642-1-10-20090623Document13 pages43571-Article Text-40642-1-10-20090623Shaaira Hoosen Mahomed RazakNo ratings yet
- Challenges To Security, Livelihoods, and Gender Justice in South SudanDocument50 pagesChallenges To Security, Livelihoods, and Gender Justice in South SudanOxfamNo ratings yet
- Challenges To Security, Livelihoods, and Gender Justice in South SudanDocument50 pagesChallenges To Security, Livelihoods, and Gender Justice in South SudanOxfamNo ratings yet
- Challenges To Security, Livelihoods, and Gender Justice in South SudanDocument50 pagesChallenges To Security, Livelihoods, and Gender Justice in South SudanOxfamNo ratings yet
- Challenges To Security, Livelihoods, and Gender Justice in South SudanDocument50 pagesChallenges To Security, Livelihoods, and Gender Justice in South SudanOxfamNo ratings yet
- Challenges To Security, Livelihoods, and Gender Justice in South SudanDocument50 pagesChallenges To Security, Livelihoods, and Gender Justice in South SudanOxfamNo ratings yet
- Challenges To Security, Livelihoods, and Gender Justice in South SudanDocument50 pagesChallenges To Security, Livelihoods, and Gender Justice in South SudanOxfamNo ratings yet
- Challenges To Security, Livelihoods, and Gender Justice in South SudanDocument50 pagesChallenges To Security, Livelihoods, and Gender Justice in South SudanOxfamNo ratings yet
- Challenges To Security, Livelihoods, and Gender Justice in South SudanDocument50 pagesChallenges To Security, Livelihoods, and Gender Justice in South SudanOxfamNo ratings yet
- Challenges To Security, Livelihoods, and Gender Justice in South SudanDocument50 pagesChallenges To Security, Livelihoods, and Gender Justice in South SudanOxfamNo ratings yet
- Challenges To Security, Livelihoods, and Gender Justice in South SudanDocument50 pagesChallenges To Security, Livelihoods, and Gender Justice in South SudanOxfamNo ratings yet
- Angels in The Dust Study GuideDocument4 pagesAngels in The Dust Study GuidetakepartNo ratings yet
- Migration, Refugees, and Health Risks: Conference Panel SummariesDocument5 pagesMigration, Refugees, and Health Risks: Conference Panel SummariesSara Dal SavioNo ratings yet
- Position Paper: The Need For Responsive Government Approach To The Prostitution in The PhilippinesDocument3 pagesPosition Paper: The Need For Responsive Government Approach To The Prostitution in The PhilippinesCalvin TransceNo ratings yet
- Effects of The Armed Conflicts On WomenDocument5 pagesEffects of The Armed Conflicts On WomenleoyuyleoNo ratings yet
- HIV Aids in Rural MalawiDocument30 pagesHIV Aids in Rural MalawiFernanda BelizárioNo ratings yet
- Afaq Rouf 22-11145 Sociocultural Anthropology SOC 223 Section A Mam Julie FlowerdayDocument3 pagesAfaq Rouf 22-11145 Sociocultural Anthropology SOC 223 Section A Mam Julie FlowerdayAfaq RaufNo ratings yet
- Tribals in The NortheastDocument1 pageTribals in The Northeasttaran4gaNo ratings yet
- Ethiopia A Socio-Economic StudyDocument17 pagesEthiopia A Socio-Economic StudyHayleye KinfeNo ratings yet
- SOCHUM Study GuideDocument42 pagesSOCHUM Study Guidesyedabdullah1338No ratings yet
- Lahore College For Women University: Geography AssignmentDocument8 pagesLahore College For Women University: Geography AssignmentAzka AsimNo ratings yet
- West African Eu PolicyDocument10 pagesWest African Eu Policyapi-430758769No ratings yet
- Philippines LiteratureDocument6 pagesPhilippines LiteratureChristina LarubisNo ratings yet
- G-10 Geography Handout 3-4Document35 pagesG-10 Geography Handout 3-4badasaamadinNo ratings yet
- Internal Migration in Ethiopia: Evidence From A Quantitative and Qualitative Research StudyDocument48 pagesInternal Migration in Ethiopia: Evidence From A Quantitative and Qualitative Research Studysishu21No ratings yet
- AP Euro, Renaissance Life NotesDocument7 pagesAP Euro, Renaissance Life NotesfioritureNo ratings yet
- Factors Leading To MigrationDocument14 pagesFactors Leading To MigrationZanzibarNo ratings yet
- The ProjectDocument40 pagesThe ProjectAkinwumi AkintayoNo ratings yet
- Factors Influencing PopulationDocument4 pagesFactors Influencing PopulationPankaj MishraNo ratings yet
- Managing Human Population AS emDocument21 pagesManaging Human Population AS emshees javedNo ratings yet
- Add. InfoDocument4 pagesAdd. InfoJames Walter Odiver ImperialNo ratings yet
- I.R Chapter 7Document7 pagesI.R Chapter 7mariamo IoselianiNo ratings yet
- Silo - Tips - Glory of Hope Orphanage Center Wolaita Ethiopia Project Proposal by Yassin GuntaDocument14 pagesSilo - Tips - Glory of Hope Orphanage Center Wolaita Ethiopia Project Proposal by Yassin GuntaFassikaw EjjiguNo ratings yet
- Sudan RGA Brief - May 2023 - CAREDocument8 pagesSudan RGA Brief - May 2023 - CAREthanhhoa220720075No ratings yet
- Africa: Egypt Sierra LeoneDocument3 pagesAfrica: Egypt Sierra Leoneapi-302428334No ratings yet
- Daniel R. Tuaño BSBM 101 CDocument2 pagesDaniel R. Tuaño BSBM 101 CJane Arcon del RosarioNo ratings yet
- Human MigrationDocument8 pagesHuman MigrationPrabhakaran Aranganathan0% (1)
- TRCDocument129 pagesTRCJohn Sheka Porpay TarawalieNo ratings yet
- Migration As An Effect of GlobalisationDocument3 pagesMigration As An Effect of Globalisationionescu andreiNo ratings yet
- Bolivia: Cultural EssentialsDocument42 pagesBolivia: Cultural Essentialskinky_zgNo ratings yet
- Poverty and Inequality in South Africa PDFDocument11 pagesPoverty and Inequality in South Africa PDFsewwandiNo ratings yet
- Youth MigrationDocument8 pagesYouth MigrationAtang TheBoss MokgwareNo ratings yet
- How To Urbanization Bring A Social ChangeDocument4 pagesHow To Urbanization Bring A Social Changesabahat shireenNo ratings yet
- Hist 322 DLMDocument7 pagesHist 322 DLMAlexy Muleh MulihNo ratings yet
- 9 - Lesson 4Document4 pages9 - Lesson 4Lapuz John Nikko R.100% (2)
- Dry Lab Exercise 4 EndocrineDocument4 pagesDry Lab Exercise 4 Endocrine06Fajrian RidhatunnisaNo ratings yet
- Administering Intradermal InjectionDocument17 pagesAdministering Intradermal InjectionPattNo ratings yet
- RM028 PDFDocument2 pagesRM028 PDFKishnsNo ratings yet
- Ijmet 10 02 176Document7 pagesIjmet 10 02 176Venkates PsnaNo ratings yet
- Titus Lithium Battery: Safety Data SheetDocument5 pagesTitus Lithium Battery: Safety Data SheetKittikun Ap UnitechNo ratings yet
- Metil MerkaptanDocument14 pagesMetil MerkaptanEngineer TeknoNo ratings yet
- Common Errors in Dental RadiographyDocument48 pagesCommon Errors in Dental RadiographyDarwin D. J. LimNo ratings yet
- KC - Program Implementation Nepal ExperienceDocument21 pagesKC - Program Implementation Nepal ExperienceDhaka2012No ratings yet
- Cephalosporin UnitDocument11 pagesCephalosporin Unitviper1402No ratings yet
- Peridex (Oral Rinse)Document11 pagesPeridex (Oral Rinse)Emeka NnajiNo ratings yet
- Patient AttendanceNo-Show PredictionDocument10 pagesPatient AttendanceNo-Show PredictionInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Benzofurano-Isatins: Search For Antimicrobial Agents: Arabian Journal of ChemistryDocument8 pagesBenzofurano-Isatins: Search For Antimicrobial Agents: Arabian Journal of Chemistrylucian_lovNo ratings yet
- Health-Problems 2 - 63706Document1 pageHealth-Problems 2 - 63706Lyudmila VergunNo ratings yet
- D2 0905 Paediatric Reference Intervals - An Update - Tina YenDocument25 pagesD2 0905 Paediatric Reference Intervals - An Update - Tina YenkamalNo ratings yet
- 7A Detailed Lesson Plan in Health 7 I. Content Standard: Teacher's Activity Students' ActivityDocument10 pages7A Detailed Lesson Plan in Health 7 I. Content Standard: Teacher's Activity Students' ActivityLeizel C. LeonidoNo ratings yet
- Container Data UtilizationDocument2,910 pagesContainer Data UtilizationCege Wa NjorogeNo ratings yet
- Detal ClinicalDocument9 pagesDetal ClinicalmohammedmdfNo ratings yet
- Notice of Post DisqualificationDocument3 pagesNotice of Post DisqualificationMelody Frac ZapateroNo ratings yet
- EAPPQ4W4CADocument9 pagesEAPPQ4W4CAPhebi ReyNo ratings yet
- Radcool 200: Safety Data SheetDocument9 pagesRadcool 200: Safety Data SheetHendri PriyantoNo ratings yet