You might also like
- AminoAcid Therapy - J.Ross 2006.12 PDFDocument94 pagesAminoAcid Therapy - J.Ross 2006.12 PDFJohn Coombs100% (2)
- 100 Ways To Live 100 YearsDocument4 pages100 Ways To Live 100 YearsMary11111No ratings yet
- Water-Soluble Vitamins: An Overview of Key Nutrients for HealthDocument89 pagesWater-Soluble Vitamins: An Overview of Key Nutrients for Healthahmedatef100% (1)
- Chapter 5 HandoutDocument4 pagesChapter 5 Handouttrixie eustaquioNo ratings yet
- UB Ebook Restoring Health Post-VaxDocument33 pagesUB Ebook Restoring Health Post-VaxDazNo ratings yet
- Alkaline Water StudyDocument5 pagesAlkaline Water StudyKENS 5No ratings yet
- Collagen Types 1Document24 pagesCollagen Types 1hayiwadaNo ratings yet
- Slow Burn SumaryDocument10 pagesSlow Burn SumarySharizan GhaniNo ratings yet
- Gut Reset User ManualDocument52 pagesGut Reset User ManualNew Mee100% (1)
- Ortoic AcidDocument25 pagesOrtoic AcidSandy Wasfy100% (1)
- ATI Nutrition Practice Exam B - Google Forms PDFDocument21 pagesATI Nutrition Practice Exam B - Google Forms PDFJohn Mixer33% (3)
- Saluyot (Corchorus Olitorius)Document15 pagesSaluyot (Corchorus Olitorius)Anonymous 3QmDBNoC5n100% (3)
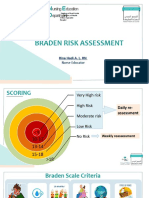
- Braden Risk AssessmentDocument19 pagesBraden Risk AssessmentRina LestariNo ratings yet
- Reverse Inflammation Naturally: Alternative Treatments For Autoimmune Disorders, Rheumatoid Arthritis, Fibromyalgia, Metabolic Syndrome, Allergies, Thyroiditis, Eczema and More. - Michelle HondaDocument5 pagesReverse Inflammation Naturally: Alternative Treatments For Autoimmune Disorders, Rheumatoid Arthritis, Fibromyalgia, Metabolic Syndrome, Allergies, Thyroiditis, Eczema and More. - Michelle HondalycubefuNo ratings yet
- Olivares2001 PDFDocument5 pagesOlivares2001 PDFEduardo Avalos PalaciosNo ratings yet
- Sucralosa y RatonesDocument13 pagesSucralosa y RatonesafamhbkNo ratings yet
- Chapter One 1.0 1.1 Background of The StudyDocument3 pagesChapter One 1.0 1.1 Background of The StudySamson DeCasparNo ratings yet
- Lindenschmidt 1991Document8 pagesLindenschmidt 1991aparna.cNo ratings yet
- Bellomo 2006Document7 pagesBellomo 2006Manal regraguiNo ratings yet
- Bullwho00048 0043Document13 pagesBullwho00048 0043christ.wong012001No ratings yet
- Principles and Practice of Oral RehydrationDocument6 pagesPrinciples and Practice of Oral RehydrationLeydi johana Rodriguez alzateNo ratings yet
- The Effect of Drinking Water PH On The Human Gut Microbiota and Glucose Regulation: Results of A Randomized Controlled Cross-Over InterventionDocument12 pagesThe Effect of Drinking Water PH On The Human Gut Microbiota and Glucose Regulation: Results of A Randomized Controlled Cross-Over InterventionFlor Da PrimaveraNo ratings yet
- 2 Edvol 2 P 2 DDocument152 pages2 Edvol 2 P 2 DJin SiclonNo ratings yet
- Deshidratación en Ancianos Cuidado A Largo Plazo Con Disfagia Orofaríngea 2007Document6 pagesDeshidratación en Ancianos Cuidado A Largo Plazo Con Disfagia Orofaríngea 2007Natalia BeltranNo ratings yet
- hydration in childrenDocument8 pageshydration in childrenpaopics arevaloNo ratings yet
- Inverse Association Between Coffee Drinking and Serum Uric Acid Concentrations in Middle-Aged Japanese MalesDocument6 pagesInverse Association Between Coffee Drinking and Serum Uric Acid Concentrations in Middle-Aged Japanese MalessyifaNo ratings yet
- DRI For Water, 2010Document48 pagesDRI For Water, 2010Stanciu Oana MariaNo ratings yet
- Ispub 13998Document6 pagesIspub 13998Bhaswati nandiNo ratings yet
- 003 Physico Chemical and Bacteriological Analysis of Selected Borehole Well Water SDocument7 pages003 Physico Chemical and Bacteriological Analysis of Selected Borehole Well Water SSuleiman Sa'ed IsmailNo ratings yet
- Ajcn 119925Document11 pagesAjcn 119925Rahmanu ReztaputraNo ratings yet
- ToxicidadDocument9 pagesToxicidadruben varelaNo ratings yet
- Articulos Cientificos Bebidas HidratantesDocument16 pagesArticulos Cientificos Bebidas HidratantesandabrilNo ratings yet
- Lifestyle Related Risk Factors in The Aetiology of Gastro-Oesophageal RefluxDocument6 pagesLifestyle Related Risk Factors in The Aetiology of Gastro-Oesophageal RefluxazlinaNo ratings yet
- V 084 P 00237Document4 pagesV 084 P 00237OlpinNo ratings yet
- Impact of An Andean Breakfast On Biochemistry and Immunochemistry Laboratory Tests: An Evaluation On BehalfDocument14 pagesImpact of An Andean Breakfast On Biochemistry and Immunochemistry Laboratory Tests: An Evaluation On BehalfJaime JaimexNo ratings yet
- Emma Wynn, Marc-Antoine Krieg, Jean-Marc Aeschlimann, Peter BurckhardtDocument5 pagesEmma Wynn, Marc-Antoine Krieg, Jean-Marc Aeschlimann, Peter BurckhardtMihai MishuNo ratings yet
- WHO On ClO2 Pages 1 and 18 RDocument2 pagesWHO On ClO2 Pages 1 and 18 RJoel Chuquichampi HuarayaNo ratings yet
- Dagli2017 (Elevated Head)Document5 pagesDagli2017 (Elevated Head)askhaeraniNo ratings yet
- Alkaline Water and Longevity A Murine StudyDocument2 pagesAlkaline Water and Longevity A Murine StudysarasNo ratings yet
- WangJP 2009Document5 pagesWangJP 2009Milton HasnatNo ratings yet
- Acute Gastroenteritis: Roscheyl Berg Tutor Bsn3A ' 12/14/16Document11 pagesAcute Gastroenteritis: Roscheyl Berg Tutor Bsn3A ' 12/14/16Roscheen Berg TutorNo ratings yet
- High Energy Requirements and Water Throughput of Adult Shuar Forager-Horticulturalists of Amazonian EcuadorDocument11 pagesHigh Energy Requirements and Water Throughput of Adult Shuar Forager-Horticulturalists of Amazonian EcuadorJoseHernanSanchezNo ratings yet
- Water intoxication in adult cattle causes neurological signsDocument7 pagesWater intoxication in adult cattle causes neurological signsallhayokNo ratings yet
- Armstrong - Hydration Biomarkers and Dietary FluidDocument6 pagesArmstrong - Hydration Biomarkers and Dietary FluidAngieda SoepartoNo ratings yet
- Effects of Chronic Protein-Calorie Malnutrition On The KidneyDocument13 pagesEffects of Chronic Protein-Calorie Malnutrition On The KidneyAgnihotram GopinathNo ratings yet
- CelluloseDocument7 pagesCellulosem waltersNo ratings yet
- Tropical Medicine & SurgeryDocument7 pagesTropical Medicine & SurgeryGinny Marie LoefflerNo ratings yet
- Contribution of Thickened Drinks, Food and Enteral and Parenteral Fluids To Fluid Intake in Hospitalised Patients With DysphagiaDocument8 pagesContribution of Thickened Drinks, Food and Enteral and Parenteral Fluids To Fluid Intake in Hospitalised Patients With Dysphagiamaritza AucapánNo ratings yet
- Aarr - Sep .2012Document15 pagesAarr - Sep .2012Γιωργος ΒλαχοςNo ratings yet
- Efek Teh Lengmongrass Di FlitrasiDocument10 pagesEfek Teh Lengmongrass Di FlitrasiAmmaliarachmiNo ratings yet
- Colonie Function and Fermentation in Men Consuming High Fiber Diets1Document10 pagesColonie Function and Fermentation in Men Consuming High Fiber Diets1MuzayyanahNo ratings yet
- American Journal of Gastroenterology Volume 104 Issue 10 2009 (Doi 10.1038/ajg.2009.329) Atia, Antwan N Buchman, Alan L - Oral Rehydration Solutions in Non-Cholera Diarrhea - A ReviewDocument9 pagesAmerican Journal of Gastroenterology Volume 104 Issue 10 2009 (Doi 10.1038/ajg.2009.329) Atia, Antwan N Buchman, Alan L - Oral Rehydration Solutions in Non-Cholera Diarrhea - A ReviewFadhil AbdillahNo ratings yet
- ISPUBDocument4 pagesISPUBNilima Aparajita SahuNo ratings yet
- Trace Minerals in Drinking Water and Total Dietary Intake in the USDocument17 pagesTrace Minerals in Drinking Water and Total Dietary Intake in the USHaseeb Ur RehmanNo ratings yet
- Cejph - Cjp-Faktor Penyebab UrolithiasisDocument6 pagesCejph - Cjp-Faktor Penyebab UrolithiasisCDKadrianNo ratings yet
- Wright 2006Document9 pagesWright 2006Nermeen ElmelegaeNo ratings yet
- Effects of Lactulose and Neomycin On Urea Metabolism in Cirrhotic SubjectsDocument5 pagesEffects of Lactulose and Neomycin On Urea Metabolism in Cirrhotic Subjectsnova adiNo ratings yet
- Comparative Analysis of Three Borehole Water Sources in Nsukka Urban Area, Enugu State, NigeriaDocument5 pagesComparative Analysis of Three Borehole Water Sources in Nsukka Urban Area, Enugu State, Nigeriagolden abidemNo ratings yet
- Nutritionreviews64 0457Document8 pagesNutritionreviews64 0457Patricia Martín OlmedoNo ratings yet
- Gambaran Elektrolit Serum Pada Anak Dengan Diare Akut PDFDocument6 pagesGambaran Elektrolit Serum Pada Anak Dengan Diare Akut PDFCHRISTIN V.WOLOLI OBSGYN 22 juni - 26 juliNo ratings yet
- Mineral Content Comparison of Tap Water and Bottled WaterDocument6 pagesMineral Content Comparison of Tap Water and Bottled Waterdontwanttodontwantt2No ratings yet
- Artigo Spirulina Como Alimento Funcional 3Document9 pagesArtigo Spirulina Como Alimento Funcional 3Mayron SousaNo ratings yet
- Two-Generation Reproduction and Developmental Neurotoxicity Study With Sodium Chlorite in The RatDocument13 pagesTwo-Generation Reproduction and Developmental Neurotoxicity Study With Sodium Chlorite in The RatÓscar G. Rodríguez A.No ratings yet
- A Study of Fluid Intake From Beverages in A Sample of Healthy French Children, Adolescents and AdultsDocument6 pagesA Study of Fluid Intake From Beverages in A Sample of Healthy French Children, Adolescents and AdultsAnonymous hvOuCjNo ratings yet
- Cellular Dehydration Acutely Degrades Mood Mainly in Women: A Counterbalanced, Crossover TrialDocument9 pagesCellular Dehydration Acutely Degrades Mood Mainly in Women: A Counterbalanced, Crossover TrialMarco Antonio Guardamino OjedaNo ratings yet
- Watermelon Juice Reduces HyperglycemiaDocument10 pagesWatermelon Juice Reduces HyperglycemiaTrinity PdplNo ratings yet
- Assessing hydration status in large populationsDocument12 pagesAssessing hydration status in large populationsAbdul Aziz WahyudinNo ratings yet
- Chlorogenic Acid and Caffeic Acid Are Absorbed in HumansDocument6 pagesChlorogenic Acid and Caffeic Acid Are Absorbed in HumansluisbrumovskyNo ratings yet
- Coffe Consumption and Kidney InjuryDocument8 pagesCoffe Consumption and Kidney InjuryCarmen BaezNo ratings yet
- The Effect Amino Acids: of inDocument13 pagesThe Effect Amino Acids: of inZarah Joy TabuyanNo ratings yet
- Frequency of Hyponatraemia and Hypokalaemia in Malnourished Children With Acute DiarrhoeaDocument4 pagesFrequency of Hyponatraemia and Hypokalaemia in Malnourished Children With Acute DiarrhoeaRaja Bajak LautNo ratings yet
- Saline Therapy: Clinical Treatises on the Pathology and Therapy of Disorders of Metabolism and NutritionFrom EverandSaline Therapy: Clinical Treatises on the Pathology and Therapy of Disorders of Metabolism and NutritionNo ratings yet
- Fish Physiology: Organic Chemical Toxicology of FishesFrom EverandFish Physiology: Organic Chemical Toxicology of FishesNo ratings yet
- Epidemiological Investigation On Chronic Copper Toxicity To Children Exposed Via The Public Drinking Water SupplyDocument18 pagesEpidemiological Investigation On Chronic Copper Toxicity To Children Exposed Via The Public Drinking Water SupplyEduardo Avalos PalaciosNo ratings yet
- Characteristics and Prediction of Sound Level in Extra-Large SpacesDocument7 pagesCharacteristics and Prediction of Sound Level in Extra-Large SpacesEduardo Avalos PalaciosNo ratings yet
- Importance of Fresh Water for LivestockDocument6 pagesImportance of Fresh Water for LivestockEduardo Avalos PalaciosNo ratings yet
- Time-Evolution of Sound Levels Around A Roadside BuildingDocument10 pagesTime-Evolution of Sound Levels Around A Roadside BuildingEduardo Avalos PalaciosNo ratings yet
- Mercury FinalDocument18 pagesMercury FinalPopescu DragosNo ratings yet
- Epidemiological Investigation On Chronic Copper Toxicity To Children Exposed Via The Public Drinking Water SupplyDocument18 pagesEpidemiological Investigation On Chronic Copper Toxicity To Children Exposed Via The Public Drinking Water SupplyEduardo Avalos PalaciosNo ratings yet
- Sulfates in Drinking WaterDocument16 pagesSulfates in Drinking WaterMathaiosVNo ratings yet
- A Quantitative Analysis of Chromium and Zinc in Water and Raw Milk in Chittagong, BangladeshDocument8 pagesA Quantitative Analysis of Chromium and Zinc in Water and Raw Milk in Chittagong, BangladeshEduardo Avalos PalaciosNo ratings yet
- Clinical Toxicologyy 22 (6) ,: 1985 by Marcel Dekker, 8 2 8Document4 pagesClinical Toxicologyy 22 (6) ,: 1985 by Marcel Dekker, 8 2 8Eduardo Avalos PalaciosNo ratings yet
- Copper saturation pathways of the urban population in Czech RepublicDocument2 pagesCopper saturation pathways of the urban population in Czech RepublicEduardo Avalos PalaciosNo ratings yet
- Turmeric Powder: Potential Alternative To Antibiotics in Broiler Chicken DietsDocument11 pagesTurmeric Powder: Potential Alternative To Antibiotics in Broiler Chicken DietsKeiven Mark Bigtasin AmpodeNo ratings yet
- Benefits of Wheat Grass JuiceDocument5 pagesBenefits of Wheat Grass JuiceRonald J'sonNo ratings yet
- Growth Performance, Blood Parameters, Immune Response and Carcass Traits of BroilersDocument17 pagesGrowth Performance, Blood Parameters, Immune Response and Carcass Traits of BroilersOliver TalipNo ratings yet
- Asc Code of Ethics PDFDocument212 pagesAsc Code of Ethics PDFCamille PilongoNo ratings yet
- MultivitaminsDocument18 pagesMultivitaminsMickel Angelo Asas MartinezNo ratings yet
- Agri Sba A.KDocument16 pagesAgri Sba A.KTj ShmurdaNo ratings yet
- Build Muscle and Strength at HomeDocument17 pagesBuild Muscle and Strength at HomeMuhammad RamaNo ratings yet
- Zinc and Breast Cancer - Breast Cancer ConquerorDocument1 pageZinc and Breast Cancer - Breast Cancer ConquerorOmar ElfarougNo ratings yet
- Vitamins and Supplements BrochureDocument16 pagesVitamins and Supplements BrochureMlungisi Lu NdlovuNo ratings yet
- Ensure Healthy Blood PressureDocument6 pagesEnsure Healthy Blood PressureWindy Ng WMNo ratings yet
- Osmoregulatory Function of Betaine in Alleviating Heat Stress in PoultryDocument17 pagesOsmoregulatory Function of Betaine in Alleviating Heat Stress in PoultrySINTA DE100% (1)
- Customer Survey AnalysisDocument56 pagesCustomer Survey AnalysisStephy SebastianNo ratings yet
- Nutritional Requirements For The Elderly - Report Kay Doc DaDocument4 pagesNutritional Requirements For The Elderly - Report Kay Doc DaMina SumaoangNo ratings yet
- Regulations for Nutraceuticals, Health Supplements and Specialty FoodsDocument61 pagesRegulations for Nutraceuticals, Health Supplements and Specialty FoodsAdrián De Medina SidoniaNo ratings yet
- Diet in CKDDocument10 pagesDiet in CKDzul43verNo ratings yet
- dm2019-0365 Interim Guidelines On LNS SQDocument8 pagesdm2019-0365 Interim Guidelines On LNS SQMary Joy GaloloNo ratings yet
- Milk Thistle - Product PresentationDocument14 pagesMilk Thistle - Product PresentationAABHIRAMNo ratings yet