You might also like
- Hi, My Name Is John: My Story of Survival with Autism and Learning DisabilitiesFrom EverandHi, My Name Is John: My Story of Survival with Autism and Learning DisabilitiesNo ratings yet
- High-Functioning Autism Spectrum Disorder: Parent's Guide to Creating Routines, Diagnosis, Managing Sensory and Autism Awareness in Kids.From EverandHigh-Functioning Autism Spectrum Disorder: Parent's Guide to Creating Routines, Diagnosis, Managing Sensory and Autism Awareness in Kids.Rating: 5 out of 5 stars5/5 (1)
- Learning more about Autism: Dealing with Autism in the FamilyFrom EverandLearning more about Autism: Dealing with Autism in the FamilyNo ratings yet
- A level Psychology Revision: Cheeky Revision ShortcutsFrom EverandA level Psychology Revision: Cheeky Revision ShortcutsRating: 5 out of 5 stars5/5 (1)
- Unit-4 CHILDHOOD MENTAL DISORDERSDocument22 pagesUnit-4 CHILDHOOD MENTAL DISORDERSNeha JainNo ratings yet
- Neurodevelopmental Disorder Part A 22032023 114816amDocument23 pagesNeurodevelopmental Disorder Part A 22032023 114816amSafi Ul RahmanNo ratings yet
- SENSORY PROCESSING DISORDER: Understanding, Managing, and Thriving with Sensory Processing Challenges (2024 Beginner Guide)From EverandSENSORY PROCESSING DISORDER: Understanding, Managing, and Thriving with Sensory Processing Challenges (2024 Beginner Guide)No ratings yet
- Parenting Guide for Strong Children: Raising Highly Sensitive Children Without ScoldingFrom EverandParenting Guide for Strong Children: Raising Highly Sensitive Children Without ScoldingNo ratings yet
- Understanding Harry's Autism DiagnosisDocument9 pagesUnderstanding Harry's Autism DiagnosisUsama NawazNo ratings yet
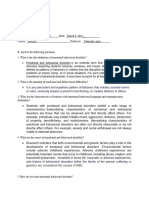
- Types of Emotional and Behavioral DisordersDocument3 pagesTypes of Emotional and Behavioral DisordersJoven Bascao CachoNo ratings yet
- Canobas, Rhona Liza-Dsped-Sec 7-Actv 2Document5 pagesCanobas, Rhona Liza-Dsped-Sec 7-Actv 2Rhona Liza CanobasNo ratings yet
- Childhood Disorder - I: Autism Spectrum Disorder Case StudyDocument8 pagesChildhood Disorder - I: Autism Spectrum Disorder Case Studypadmini singhNo ratings yet
- Boundless Love: Embracing The Energy And Challenges Of Special ChildrenFrom EverandBoundless Love: Embracing The Energy And Challenges Of Special ChildrenNo ratings yet
- Pervasive Developmental Disorders ExplainedDocument22 pagesPervasive Developmental Disorders Explainedrupal aroraNo ratings yet
- Sample Disorders Common Among Children and AdolescentsDocument39 pagesSample Disorders Common Among Children and AdolescentsAdilHumdaniNo ratings yet
- Autism Spectrum DisordersDocument26 pagesAutism Spectrum Disordersbsndbh65wcNo ratings yet
- First Aid for Your Emotional Hurts: Helping Children with Emotional Problems: Helping Children with Emotional ProblemsFrom EverandFirst Aid for Your Emotional Hurts: Helping Children with Emotional Problems: Helping Children with Emotional ProblemsNo ratings yet
- Autism PPTDocument55 pagesAutism PPTTadesse TedlaNo ratings yet
- Sensation Me Crazy: A Guide, Tools, and Fun Games to Assist and Help Develop Your Child With Sensory Processing Disorder (SPD)From EverandSensation Me Crazy: A Guide, Tools, and Fun Games to Assist and Help Develop Your Child With Sensory Processing Disorder (SPD)No ratings yet
- Understanding ADHD: What causes ADHD and how to deal with itFrom EverandUnderstanding ADHD: What causes ADHD and how to deal with itRating: 5 out of 5 stars5/5 (1)
- Dominica AutismDocument27 pagesDominica AutismAadeshMistryNo ratings yet
- Highly sensitive & emotional children: How to lovingly accompany, educate, encourage and strengthen your child - Highly sensitive and happyFrom EverandHighly sensitive & emotional children: How to lovingly accompany, educate, encourage and strengthen your child - Highly sensitive and happyNo ratings yet
- Definition of Autism and ADHDDocument4 pagesDefinition of Autism and ADHDNJ BesanaNo ratings yet
- Beat ADD & ADHD: Treating ADD And ADHD In AdultsFrom EverandBeat ADD & ADHD: Treating ADD And ADHD In AdultsRating: 5 out of 5 stars5/5 (5)
- CNS Development in Children and Neuropsychological AssessmentDocument19 pagesCNS Development in Children and Neuropsychological Assessmentvalentina chistrugaNo ratings yet
- Clinical Mental Disorder 2.1Document32 pagesClinical Mental Disorder 2.1Tim AroscoNo ratings yet
- Autism Treatment Tips: The Complete Guide to Taking Care of an Autistic Child (Autism Spectrum Disorder, Autism Symptoms, Autism Signs)From EverandAutism Treatment Tips: The Complete Guide to Taking Care of an Autistic Child (Autism Spectrum Disorder, Autism Symptoms, Autism Signs)Rating: 4 out of 5 stars4/5 (1)
- Behaviour Problems in Children and HomoeopathyDocument6 pagesBehaviour Problems in Children and HomoeopathyHomoeopathic Pulse100% (1)
- Autism B Theory: The Cause, Development and Support of AutismFrom EverandAutism B Theory: The Cause, Development and Support of AutismNo ratings yet
- Easy Guide to Attachment Disorders in Adults: Understanding Adult Attachment Styles With Relationships And Attachment Trauma And HealingFrom EverandEasy Guide to Attachment Disorders in Adults: Understanding Adult Attachment Styles With Relationships And Attachment Trauma And HealingNo ratings yet
- UntitledDocument1 pageUntitledRepato Jenalyn R.No ratings yet
- Week 11 Ncm 109 Lecture PptxDocument49 pagesWeek 11 Ncm 109 Lecture PptxPolicarpio AprilNo ratings yet
- Signs of ADHD, Diagnosis and Differential DiagnosisDocument25 pagesSigns of ADHD, Diagnosis and Differential DiagnosisYasNo ratings yet
- Empowered Parenting: Practical Tips For Raising A Child With AutismFrom EverandEmpowered Parenting: Practical Tips For Raising A Child With AutismNo ratings yet
- Case Analysis SchizoDocument4 pagesCase Analysis SchizoiamELHIZANo ratings yet
- Childhood Disorders 1Document21 pagesChildhood Disorders 1Prescy Bunoan Dela CruzNo ratings yet
- ADHD RAISING AN EXPLOSIVE CHILD: Nurturing Resilience and Communication in Children with ADHD (2023 Guide for Beginners)From EverandADHD RAISING AN EXPLOSIVE CHILD: Nurturing Resilience and Communication in Children with ADHD (2023 Guide for Beginners)No ratings yet
- Artifact Intro and Ed IdDocument4 pagesArtifact Intro and Ed Idapi-253984664No ratings yet
- Autism Spectrum Disorder: Group 1Document26 pagesAutism Spectrum Disorder: Group 1LAARNI MARIE G. CARIÑONo ratings yet
- Autism Revealed: All you Need to Know about Autism, Autistic Children and Adults, How to Manage Autism, and More!From EverandAutism Revealed: All you Need to Know about Autism, Autistic Children and Adults, How to Manage Autism, and More!No ratings yet
- Types of Disorders, Their Causes and Nature (ADHD, SPD, ASD, ODD, OCDDocument16 pagesTypes of Disorders, Their Causes and Nature (ADHD, SPD, ASD, ODD, OCDriha mogNo ratings yet
- Pervasive Developmental Disorders: Autisic DisorderDocument10 pagesPervasive Developmental Disorders: Autisic DisorderBinu MathewNo ratings yet
- 3.12 TM Lesson PlanDocument3 pages3.12 TM Lesson PlanzonilocaNo ratings yet
- Emotional Agility WorkbookDocument43 pagesEmotional Agility WorkbookpdfdownloadNo ratings yet
- Reflections On Aphantasia: SciencedirectDocument2 pagesReflections On Aphantasia: SciencedirectJORGE ENRIQUE CAICEDO GONZ�LESNo ratings yet
- BCC Understanding The SelfDocument56 pagesBCC Understanding The Selfnew genshinNo ratings yet
- Ocular dominance columns visual stimulationDocument6 pagesOcular dominance columns visual stimulationAlex MNo ratings yet
- The Peripheral Nervous System: ObjectivesDocument4 pagesThe Peripheral Nervous System: ObjectivesIbra TutorNo ratings yet
- Jurnal TinitusDocument14 pagesJurnal TinitusAndriyani YaniNo ratings yet
- Psychology Revision Assignment Key ConceptsDocument2 pagesPsychology Revision Assignment Key Conceptsishwar singhNo ratings yet
- Assessing The Musculoskeletal & Neurological SystemDocument34 pagesAssessing The Musculoskeletal & Neurological SystemalelichengNo ratings yet
- BRAINSTEM II Clinical CorrelatesDocument6 pagesBRAINSTEM II Clinical CorrelatesrizaNo ratings yet
- The Power of Smiling British English TeacherDocument12 pagesThe Power of Smiling British English TeacherGerto RequenaNo ratings yet
- The Flavor of PleasureDocument6 pagesThe Flavor of PleasureNguyen Nha LinhNo ratings yet
- How Sleep Quality Impacts College Students' Test ScoresDocument25 pagesHow Sleep Quality Impacts College Students' Test ScoresLyvette FuntanarNo ratings yet
- Sto. Nino College Science Exam ReviewDocument4 pagesSto. Nino College Science Exam ReviewMARY ROSENo ratings yet
- Emotions Before, During, and After Dreaming Sleep: Calvin Kai-Ching YuDocument14 pagesEmotions Before, During, and After Dreaming Sleep: Calvin Kai-Ching YuMariaNo ratings yet
- Dopamine, Smartphones & You - A Battle For Your Time - Science in The News PDFDocument18 pagesDopamine, Smartphones & You - A Battle For Your Time - Science in The News PDFLeandroCisternaHernandezNo ratings yet
- A Brief History of The Science of LearningDocument36 pagesA Brief History of The Science of LearningPraptaning Budi UtamiNo ratings yet
- How-To SapienDocument36 pagesHow-To SapienOz100% (3)
- ECS302 AI Module I NotesDocument37 pagesECS302 AI Module I NotesAlexandra Daddario0% (1)
- AphasiaDocument4 pagesAphasiaSusan KNo ratings yet
- Three domains of learning taxonomy guideDocument7 pagesThree domains of learning taxonomy guideMelNo ratings yet
- Free Recall VS Cued RecallDocument8 pagesFree Recall VS Cued RecallChaudhuri Musavvir AsifNo ratings yet
- Understanding the Interaction Between Mind and BodyDocument8 pagesUnderstanding the Interaction Between Mind and Bodyamit50% (2)
- 752-Article Text-875-1-10-20191207Document4 pages752-Article Text-875-1-10-20191207sandykartikapNo ratings yet
- Accommodations MenuDocument7 pagesAccommodations Menuapi-508300120No ratings yet
- Biomedical Sleep Inducer Generates FieldsDocument21 pagesBiomedical Sleep Inducer Generates Fieldskiswah computersNo ratings yet
- What Makes a Gifted BrainDocument35 pagesWhat Makes a Gifted Brainmarkus_danusantoso100% (1)
- Types of Pain ExplainedDocument3 pagesTypes of Pain ExplainedSab IbarretaNo ratings yet
- Keeping The Brain HealthyDocument1 pageKeeping The Brain HealthyAditya RamroopNo ratings yet
- Daniel Todes-Ivan Pavlov - Exploring The Animal Machine (Oxford Portraits in Science) - Oxford University Press, USA (2000)Document113 pagesDaniel Todes-Ivan Pavlov - Exploring The Animal Machine (Oxford Portraits in Science) - Oxford University Press, USA (2000)Miguel NevesNo ratings yet