You might also like
- The clinical effectiveness and personal experience of supported standing for children with cerebral palsy: a comprehensive systematic review protocolDocument18 pagesThe clinical effectiveness and personal experience of supported standing for children with cerebral palsy: a comprehensive systematic review protocolAna Claudia Pinheiro MachadoNo ratings yet
- Amep 259557 Perceived Stress Among Iranian Nursing Students in A ClinicaDocument7 pagesAmep 259557 Perceived Stress Among Iranian Nursing Students in A ClinicaMarianne CoracheaNo ratings yet
- No,: 134-A-12/16/01/MC/2022-Admin DateDocument1 pageNo,: 134-A-12/16/01/MC/2022-Admin DateKaushal ChandNo ratings yet
- Stanford MigraineDocument1 pageStanford MigraineReza Ishak EstikoNo ratings yet
- Sources of Stress and Coping Behaviors Among Nursing Students Throughout Their First Clinical TrainingDocument7 pagesSources of Stress and Coping Behaviors Among Nursing Students Throughout Their First Clinical Trainingاحمد العايديNo ratings yet
- Alhamad 2023Document10 pagesAlhamad 2023Juan Carlos FloresNo ratings yet
- Faktor 2 QCDocument13 pagesFaktor 2 QCwi bowoNo ratings yet
- H A - N, P D, MSN, RN: UDA L Oumani HDocument3 pagesH A - N, P D, MSN, RN: UDA L Oumani HHamed NazariNo ratings yet
- Neuroinfectious Disease CONTINUUM Ago 2021Document313 pagesNeuroinfectious Disease CONTINUUM Ago 2021Olga Manco GuzmánNo ratings yet
- Center For Health Sciences BrochureDocument4 pagesCenter For Health Sciences BrochureGraduate School USANo ratings yet
- Academic Health System Universitas Gadjah Mada: Pengembangan Rencana Strategis Dan Program KerjaDocument20 pagesAcademic Health System Universitas Gadjah Mada: Pengembangan Rencana Strategis Dan Program KerjaAndre SiahaanNo ratings yet
- DR Anoop Cv-CompressedDocument3 pagesDR Anoop Cv-CompressedvarunNo ratings yet
- Assessment of 4th year medical student ethicsDocument5 pagesAssessment of 4th year medical student ethicsOmarNo ratings yet
- deocument_526Full download book Laboratory Manual To Accompany Physical Examination Health Assessment Pdf pdfDocument41 pagesdeocument_526Full download book Laboratory Manual To Accompany Physical Examination Health Assessment Pdf pdfkaren.martin433100% (14)
- Adeaaadsasrequiredandrecommendedcourses Final002Document5 pagesAdeaaadsasrequiredandrecommendedcourses Final002api-704664919No ratings yet
- MPH Program Flye-2011 - Ver4 FinalDocument2 pagesMPH Program Flye-2011 - Ver4 Finalhari_srmcNo ratings yet
- MSUcareerDocument1 pageMSUcareernajiy93No ratings yet
- Anallett2007405887 896Document12 pagesAnallett2007405887 896Annisa UtamiNo ratings yet
- Effectiveness of Formal Physical Therapy Following Total Shoulder Arthroplasty: A Systematic ReviewDocument8 pagesEffectiveness of Formal Physical Therapy Following Total Shoulder Arthroplasty: A Systematic ReviewBüşra YılmazNo ratings yet
- Guidebook SKHBDocument13 pagesGuidebook SKHBriska asriaNo ratings yet
- Patients As Partners in Research: It's The Right Thing To DoDocument4 pagesPatients As Partners in Research: It's The Right Thing To DoTNo ratings yet
- National Seminar On Recent Innovations in Health and Life Science ResearchDocument2 pagesNational Seminar On Recent Innovations in Health and Life Science ResearchKU ZOOLOGYNo ratings yet
- Efficacy of Chlorhexidine Herbal Formulation For.13Document6 pagesEfficacy of Chlorhexidine Herbal Formulation For.13Sai BabaNo ratings yet
- university students 2Document2 pagesuniversity students 2احمد العايديNo ratings yet
- Alkhawaldeh Et Al 2024 University Students Physical Activity Perceived Barriers and Benefits To Physical Activity andDocument9 pagesAlkhawaldeh Et Al 2024 University Students Physical Activity Perceived Barriers and Benefits To Physical Activity andاحمد العايديNo ratings yet
- Prevalence of Stress and Its Association With Resilience Among Medical Students in A Tertiary Care Center, Aurangabad, Maharashtra, IndiaDocument9 pagesPrevalence of Stress and Its Association With Resilience Among Medical Students in A Tertiary Care Center, Aurangabad, Maharashtra, IndiaIJAR JOURNALNo ratings yet
- Appcrc-Fm Conference 2017 Draft Program 20170328Document7 pagesAppcrc-Fm Conference 2017 Draft Program 20170328api-352941397No ratings yet
- Application Areas of BioprintingDocument15 pagesApplication Areas of Bioprinting091 Santhosh MNo ratings yet
- Depression in Medical Students: Current InsightsDocument11 pagesDepression in Medical Students: Current InsightswatiNo ratings yet
- Academic Structure - SPDocument3 pagesAcademic Structure - SPTeressa KhouryNo ratings yet
- Resume CV Dr. Kang Zhang MD PHDDocument15 pagesResume CV Dr. Kang Zhang MD PHDKang ZhangNo ratings yet
- Environmental Toxicology in Addressing Public Health Challenges in East AsiaDocument4 pagesEnvironmental Toxicology in Addressing Public Health Challenges in East AsiaS. S. PrinceNo ratings yet
- Art 8Document76 pagesArt 8Fabiana FernandesNo ratings yet
- B.Pharma student's hospital training reportDocument4 pagesB.Pharma student's hospital training reportShaan MohammadNo ratings yet
- The Effect of Study Preparation On Test Anxiety AnDocument7 pagesThe Effect of Study Preparation On Test Anxiety AnjuneldelmundoNo ratings yet
- BS Allied Health 1st Sem 27jan22Document43 pagesBS Allied Health 1st Sem 27jan22Gulab khanNo ratings yet
- Curriculum VitaeDocument9 pagesCurriculum Vitaeshah86zamNo ratings yet
- Omkar Prasad Baidya CertificatesDocument1 pageOmkar Prasad Baidya CertificatesOMKAR PRASAD BAIDYANo ratings yet
- Signature-Signed Signed (1) 220902 173648Document3 pagesSignature-Signed Signed (1) 220902 173648Agil SaputraNo ratings yet
- Bioinformatics and Its Applications in Plant Biology: Seung Yon Rhee, Julie Dickerson, and Dong XuDocument29 pagesBioinformatics and Its Applications in Plant Biology: Seung Yon Rhee, Julie Dickerson, and Dong Xugauravj2000No ratings yet
- Impact of Physical Exercise Programs in Breast Cancer Survivors On Health-Related Quality of Life, Physical Fitness, and Body Composition Evidence From Systematic Reviews and Meta-AnalysesDocument15 pagesImpact of Physical Exercise Programs in Breast Cancer Survivors On Health-Related Quality of Life, Physical Fitness, and Body Composition Evidence From Systematic Reviews and Meta-AnalysesJoao da HoraNo ratings yet
- The Effectiveness of Basic Life Support Training oDocument12 pagesThe Effectiveness of Basic Life Support Training oambreensaba.btconNo ratings yet
- Hamza ThesisDocument45 pagesHamza ThesisShanoo AmeerNo ratings yet
- Structural Equation Modeling: A Multidisciplinary Journal: Please Scroll Down For ArticleDocument32 pagesStructural Equation Modeling: A Multidisciplinary Journal: Please Scroll Down For ArticleIan BishopNo ratings yet
- Aims & Scope: Human & Experimental Toxicology Human & Experimental ToxicologyDocument1 pageAims & Scope: Human & Experimental Toxicology Human & Experimental ToxicologyDr MathanNo ratings yet
- Biomechanical Approaches To Identify and Quantify Injury Mechanisms and Risk Factors in Women's Artistic GymnasticsDocument20 pagesBiomechanical Approaches To Identify and Quantify Injury Mechanisms and Risk Factors in Women's Artistic GymnasticsLucky AbrorryNo ratings yet
- HazmatDocument2 pagesHazmatJaime Virgilio Flores PalominoNo ratings yet
- BCSC1718 S11Document17 pagesBCSC1718 S11ZackychunNo ratings yet
- 03 SHTM2007Document30 pages03 SHTM2007مركز ريلاكس للعلاج الطبيعيNo ratings yet
- Jianliang (Lucas) ManDocument1 pageJianliang (Lucas) ManLucas ManNo ratings yet
- Jurnal Kedokteran Dan Kesehatan Indonesia: Indonesian Journal of Medicine and HealthDocument5 pagesJurnal Kedokteran Dan Kesehatan Indonesia: Indonesian Journal of Medicine and Healthagus indrawanNo ratings yet
- Tentrem Hotel Yogyakarta: Unity in Diversity and The Standardisation of Clinical Pharmacy ServicesDocument2 pagesTentrem Hotel Yogyakarta: Unity in Diversity and The Standardisation of Clinical Pharmacy Servicesganesha trengginasNo ratings yet
- Curriculum Evaluation of Physiology Subject Of.55Document5 pagesCurriculum Evaluation of Physiology Subject Of.55tientai_pcNo ratings yet
- AMEP 316201 Factors Affecting The Quality of Undergraduate Pharmacy StudDocument10 pagesAMEP 316201 Factors Affecting The Quality of Undergraduate Pharmacy StudKingsd HasNo ratings yet
- Faculty Of: Applied SciencesDocument20 pagesFaculty Of: Applied SciencesEddy YusufNo ratings yet
- Retrieve PDFDocument9 pagesRetrieve PDFVictor Enrique Chavez TaegerNo ratings yet
- KMU DPT curriculum guide for anatomy, physiology and moreDocument49 pagesKMU DPT curriculum guide for anatomy, physiology and moreMohammad AliNo ratings yet
- Sri Ramachandra Institute of Higher Education and Research: Our HistoryDocument2 pagesSri Ramachandra Institute of Higher Education and Research: Our HistoryMohan PrasadNo ratings yet
- Sports Medicine 2018 SaundersDocument21 pagesSports Medicine 2018 SaundersElisa EspinosaNo ratings yet
- PROLOG: Patient Management in OfficeFrom EverandPROLOG: Patient Management in OfficeRating: 5 out of 5 stars5/5 (4)
- 2022 State of Medical Device ReportDocument38 pages2022 State of Medical Device ReportDiego A Echavarría ANo ratings yet
- The GRASP Taxonomy of Human Grasp TypesDocument12 pagesThe GRASP Taxonomy of Human Grasp TypesSusana AhumadaNo ratings yet
- Overview of The ANSI/HFES 100 - 2007 Ergonomic Standard: A New Standard Is ReleasedDocument1 pageOverview of The ANSI/HFES 100 - 2007 Ergonomic Standard: A New Standard Is ReleasedDiego A Echavarría ANo ratings yet
- Task AnalisisDocument43 pagesTask AnalisisDiego A Echavarría ANo ratings yet
- Task AnalisisDocument43 pagesTask AnalisisDiego A Echavarría ANo ratings yet
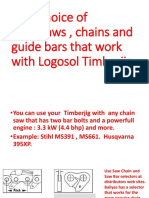
- Your Choice of Chainsaws, Chains and Guide Bars That Work With Logosol TimberjigDocument6 pagesYour Choice of Chainsaws, Chains and Guide Bars That Work With Logosol TimberjigDiego A Echavarría ANo ratings yet
- MHAC-An Assessment Tool For Analysing Manual Material Handling TasksDocument14 pagesMHAC-An Assessment Tool For Analysing Manual Material Handling TasksDiego A Echavarría ANo ratings yet
- Moscow Higher Education Institutions: Eco-Ergonomic Aspects of Operation and Environmental InitiativesDocument7 pagesMoscow Higher Education Institutions: Eco-Ergonomic Aspects of Operation and Environmental InitiativesDiego A Echavarría ANo ratings yet
- E3sconf hrc2018 02017Document5 pagesE3sconf hrc2018 02017Diego A Echavarría ANo ratings yet
- Workplace Ergonomic Guide Darcor Final January 2015Document14 pagesWorkplace Ergonomic Guide Darcor Final January 2015Diego A Echavarría ANo ratings yet
- Effect of Work With Visual Display Units On Musculo-Skeletal Disorders in The Office EnvironmentDocument9 pagesEffect of Work With Visual Display Units On Musculo-Skeletal Disorders in The Office EnvironmentDiego A Echavarría ANo ratings yet
- Assessment of The Ergonomic Risk From Saddle and CDocument14 pagesAssessment of The Ergonomic Risk From Saddle and CDiego A Echavarría ANo ratings yet
- Visual Ergonomics Solutions for Lighting & Eye HealthDocument7 pagesVisual Ergonomics Solutions for Lighting & Eye HealthDiego A Echavarría ANo ratings yet
- Visual Ergonomics at Work and Leisure: Paying It ForwardDocument2 pagesVisual Ergonomics at Work and Leisure: Paying It ForwardDiego A Echavarría ANo ratings yet
- Visual Ergonomics at Work and Leisure: Paying It ForwardDocument2 pagesVisual Ergonomics at Work and Leisure: Paying It ForwardDiego A Echavarría ANo ratings yet
- Validity and Reliability of A Dental Operator Posture Assessment Instrument (PAI)Document10 pagesValidity and Reliability of A Dental Operator Posture Assessment Instrument (PAI)Diego A Echavarría ANo ratings yet
- Quality Assessment of The University Classroom Lighting - A Case StudyDocument8 pagesQuality Assessment of The University Classroom Lighting - A Case StudyDiego A Echavarría ANo ratings yet
- Visual Ergonomics in the WorkplaceDocument11 pagesVisual Ergonomics in the WorkplaceDiego A Echavarría ANo ratings yet
- The Benefits of Natural Light: January-February 2014Document3 pagesThe Benefits of Natural Light: January-February 2014Diego A Echavarría ANo ratings yet
- SSL Trajectories Proc IEEEDocument18 pagesSSL Trajectories Proc IEEEDiego A Echavarría ANo ratings yet
- A Literature Review of The Effects of Natural Light On Building OccupantsDocument58 pagesA Literature Review of The Effects of Natural Light On Building OccupantsDiego A Echavarría ANo ratings yet
- Design Principles For Green Ergonomics: April 2013Document6 pagesDesign Principles For Green Ergonomics: April 2013Diego A Echavarría ANo ratings yet
- Hsg38 Lighting at Work (HSE)Document47 pagesHsg38 Lighting at Work (HSE)kanakarao1No ratings yet
- The Benefits of Natural Light: January-February 2014Document3 pagesThe Benefits of Natural Light: January-February 2014Diego A Echavarría ANo ratings yet
- Daylight For Health and Efficiency - A New Career For An Old FriendDocument8 pagesDaylight For Health and Efficiency - A New Career For An Old FriendDiego A Echavarría ANo ratings yet
- Evaluation and Improvement of Lighting Efficiency in Working SpacesDocument16 pagesEvaluation and Improvement of Lighting Efficiency in Working SpacesDiego A Echavarría ANo ratings yet
- Daylighting & Human PerformanceDocument3 pagesDaylighting & Human PerformancetbeedleNo ratings yet
- Visual Ergonomics Solutions for Lighting & Eye HealthDocument7 pagesVisual Ergonomics Solutions for Lighting & Eye HealthDiego A Echavarría ANo ratings yet
- Human-centric lighting benefits with TELETASK systemDocument13 pagesHuman-centric lighting benefits with TELETASK systemDiego A Echavarría ANo ratings yet
- Flava Works vs. MyVidster, Leaseweb, Voxel - Net, Et All - 4th Amended ComplaintDocument340 pagesFlava Works vs. MyVidster, Leaseweb, Voxel - Net, Et All - 4th Amended ComplaintPhillip BleicherNo ratings yet
- ĐỀ THI GIỮA KÌ 2 - E9 (TẤN)Document4 pagesĐỀ THI GIỮA KÌ 2 - E9 (TẤN)xyencoconutNo ratings yet
- OS Fundamentals: Memory, Processes, KernelsDocument36 pagesOS Fundamentals: Memory, Processes, KernelsSparkerz S Vijay100% (1)
- Mikro Prism Manual English PDFDocument18 pagesMikro Prism Manual English PDFrakeshr2007No ratings yet
- A Simple Gesture RomanDocument2 pagesA Simple Gesture Romanapi-588299405No ratings yet
- Learning Recovery Plan2Document8 pagesLearning Recovery Plan2Remelyn RodrigoNo ratings yet
- CVDocument7 pagesCVRedemptah Mutheu MutuaNo ratings yet
- Ashtadhyayi of PaniniDocument19 pagesAshtadhyayi of Paniniall4downloads50% (2)
- Intellectual DisabilitiesDocument23 pagesIntellectual DisabilitiesKim SorianoNo ratings yet
- Literature Review Computer VisionDocument6 pagesLiterature Review Computer Visionfveec9sx100% (1)
- Data Compilation TemplateDocument257 pagesData Compilation TemplateemelyseuwaseNo ratings yet
- STOW - Vol. 3 - ScheduleDocument12 pagesSTOW - Vol. 3 - ScheduleDavid A. Malin Jr.100% (2)
- Lesson Plan For PortfolioDocument6 pagesLesson Plan For Portfolioapi-282640896No ratings yet
- ch-1 Phy MEASUREMENT AND MOTIONDocument2 pagesch-1 Phy MEASUREMENT AND MOTIONRakesh GuptaNo ratings yet
- Social, Humanitarian and Cultural Committee (SOCHUM)Document58 pagesSocial, Humanitarian and Cultural Committee (SOCHUM)Klara TomsicNo ratings yet
- Fcra Act 2010 PDFDocument2 pagesFcra Act 2010 PDFKateNo ratings yet
- Amazon - in - Order 402-9638723-6823558 PDFDocument1 pageAmazon - in - Order 402-9638723-6823558 PDFanurag kumarNo ratings yet
- X-Ray Artifacts: by DR Mangal S MahajanDocument12 pagesX-Ray Artifacts: by DR Mangal S MahajanTsega HagosNo ratings yet
- WBCSC Information Sheet For Interview Advt - 1 - 2015 - UpdatedDocument1 pageWBCSC Information Sheet For Interview Advt - 1 - 2015 - UpdatedArindam GhoshNo ratings yet
- Monetizing Judgments DatasheetDocument9 pagesMonetizing Judgments DatasheetJohnWilliams100% (4)
- Poultry Fool & FinalDocument42 pagesPoultry Fool & Finalaashikjayswal8No ratings yet
- Jack Welch and Jeffery Immelt: Continuity and Change at GEDocument40 pagesJack Welch and Jeffery Immelt: Continuity and Change at GEPrashant VermaNo ratings yet
- Activityideabank FinalDocument72 pagesActivityideabank FinalJoy Tu TranNo ratings yet
- Inter CavablarDocument86 pagesInter CavablarcavidannuriyevNo ratings yet
- European & Balkan: PerspectivesDocument20 pagesEuropean & Balkan: PerspectivesStefan ChichevalievNo ratings yet
- Asma G.SDocument5 pagesAsma G.SAfia FaheemNo ratings yet
- Soymilk MenDocument7 pagesSoymilk Mentonious95No ratings yet
- Prathiksha Cae ResumeDocument3 pagesPrathiksha Cae ResumeMustafa SheriffNo ratings yet
- Procedures For Conducting Practical Tasks and Supervisor Instructions 0417Document5 pagesProcedures For Conducting Practical Tasks and Supervisor Instructions 0417Vignesh KumarNo ratings yet
- Contract Day Watchman SHS - O. SanoDocument2 pagesContract Day Watchman SHS - O. SanoZaldy Tabugoca100% (2)