You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Preparation: Self-Paced Scripting in Servicenow FundamentalsDocument5 pagesPreparation: Self-Paced Scripting in Servicenow FundamentalsCrippled SoulNo ratings yet
- Therm Coal Out LookDocument27 pagesTherm Coal Out LookMai Kim Ngan100% (1)
- ABO Case Report Work File PDFDocument9 pagesABO Case Report Work File PDFmonwarul azizNo ratings yet
- A 3D Computer Aided Design System Applied To Diagnosis and Treatment in Orthodontics PDFDocument12 pagesA 3D Computer Aided Design System Applied To Diagnosis and Treatment in Orthodontics PDFmonwarul azizNo ratings yet
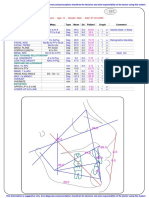
- Ricketts Analysis: Max. PositionDocument1 pageRicketts Analysis: Max. Positionmonwarul azizNo ratings yet
- A Clinical Investigation of The Efficacy of Low Lavel Laser PDFDocument9 pagesA Clinical Investigation of The Efficacy of Low Lavel Laser PDFmonwarul azizNo ratings yet
- 9 Didactica MaestrosDocument6 pages9 Didactica MaestrosCalderon RafaNo ratings yet
- Cellular Effect Related To The Clinical Uses of Laser in Orthodontics PDFDocument5 pagesCellular Effect Related To The Clinical Uses of Laser in Orthodontics PDFmonwarul azizNo ratings yet
- Buccal Corridor PDFDocument6 pagesBuccal Corridor PDFmonwarul azizNo ratings yet
- Clinical Effect of CO2 Laser in Reducing Pain in Orthodontics PDFDocument5 pagesClinical Effect of CO2 Laser in Reducing Pain in Orthodontics PDFmonwarul azizNo ratings yet
- Cellular Effects Related To The Clinical Uses of Laser in OrthodonticsDocument5 pagesCellular Effects Related To The Clinical Uses of Laser in Orthodonticsmonwarul azizNo ratings yet
- MBT Versatile Bracket Placement Guide Ifu PDFDocument1 pageMBT Versatile Bracket Placement Guide Ifu PDFmonwarul azizNo ratings yet
- Laser Debonding of Ceramic Brackets PDFDocument5 pagesLaser Debonding of Ceramic Brackets PDFmonwarul azizNo ratings yet
- The Ricketts Analysis Uses The Following MarkersDocument2 pagesThe Ricketts Analysis Uses The Following Markersmonwarul azizNo ratings yet
- Bcoe Examinee Worksheet PDFDocument1 pageBcoe Examinee Worksheet PDFmonwarul azizNo ratings yet
- Dental Orthodontic Technology Rem F1MA34 PDFDocument10 pagesDental Orthodontic Technology Rem F1MA34 PDFmonwarul azizNo ratings yet
- Clinical Effect of CO2 Laser in Reducing Pain in Orthodontics PDFDocument5 pagesClinical Effect of CO2 Laser in Reducing Pain in Orthodontics PDFmonwarul azizNo ratings yet
- Stet 2023 (Computer Science) Full Form: Programming Learning Center Search On Youtube:-@plc - SD Like and SubscribeDocument7 pagesStet 2023 (Computer Science) Full Form: Programming Learning Center Search On Youtube:-@plc - SD Like and SubscribeShiv KantNo ratings yet
- De La Salle University College of Business Course Checklist: Basirec SystandDocument2 pagesDe La Salle University College of Business Course Checklist: Basirec SystandncllpdllNo ratings yet
- Research Article: Deep Learning-Based Real-Time AI Virtual Mouse System Using Computer Vision To Avoid COVID-19 SpreadDocument8 pagesResearch Article: Deep Learning-Based Real-Time AI Virtual Mouse System Using Computer Vision To Avoid COVID-19 SpreadRatan teja pNo ratings yet
- Updating The Network Controller Server CertificateDocument4 pagesUpdating The Network Controller Server CertificateNavneetMishraNo ratings yet
- Jan Lokpal Bill Lok Sabha Rajya SabhaDocument4 pagesJan Lokpal Bill Lok Sabha Rajya SabhasushkanwarNo ratings yet
- Applying Lean Techniques in The Infrastructure Project: Jubail Industrial City, Suadi ArabiaDocument20 pagesApplying Lean Techniques in The Infrastructure Project: Jubail Industrial City, Suadi ArabiaYogesh SharmaNo ratings yet
- TTD's Role in EducationDocument37 pagesTTD's Role in Educationsri_iasNo ratings yet
- Precision Agriculture Using LoraDocument22 pagesPrecision Agriculture Using Loravrashikesh patilNo ratings yet
- FINANCE CASES AND TOPICSDocument7 pagesFINANCE CASES AND TOPICSFuzael AminNo ratings yet
- Labour Welfare Management at Piaggio vehicles Pvt. LtdDocument62 pagesLabour Welfare Management at Piaggio vehicles Pvt. Ltdnikhil kumarNo ratings yet
- 231025+ +JBS+3Q23+Earnings+Preview VFDocument3 pages231025+ +JBS+3Q23+Earnings+Preview VFgicokobayashiNo ratings yet
- Posteguillo The Semantic Structure of Computer Science Research ArticalsDocument22 pagesPosteguillo The Semantic Structure of Computer Science Research ArticalsRobin ThomasNo ratings yet
- Kamor Ul Islam Jakoan Kobir Riad Omar Faruk Iqramul Hasan MD Abdur Rahman MD Kamrul Hasan FahimDocument16 pagesKamor Ul Islam Jakoan Kobir Riad Omar Faruk Iqramul Hasan MD Abdur Rahman MD Kamrul Hasan FahimRezoan FarhanNo ratings yet
- CAO 2018 T3 Question PaperDocument2 pagesCAO 2018 T3 Question Paperharsh guptaNo ratings yet
- Cisco CallManager Express 10Document8 pagesCisco CallManager Express 10Bryan GaviganNo ratings yet
- Purpose: IT System and Services Acquisition Security PolicyDocument12 pagesPurpose: IT System and Services Acquisition Security PolicysudhansuNo ratings yet
- Top Triangle Bikini Kinda PatternDocument5 pagesTop Triangle Bikini Kinda PatternVALLEDOR, Dianne Ces Marie G.No ratings yet
- BCA IV Sem Open Source TechnologyDocument4 pagesBCA IV Sem Open Source TechnologyKavya NayakNo ratings yet
- Principles of BioenergyDocument25 pagesPrinciples of BioenergyNazAsyrafNo ratings yet
- BIR Rule on Taxing Clubs OverturnedDocument2 pagesBIR Rule on Taxing Clubs OverturnedLucky JavellanaNo ratings yet
- Lasco v. UN Revolving Fund G.R. Nos. 109095-109107Document3 pagesLasco v. UN Revolving Fund G.R. Nos. 109095-109107shannonNo ratings yet
- Soil Fabric LoggingDocument4 pagesSoil Fabric LoggingCaraUnggahNo ratings yet
- FINAL REPORT (L ND M)Document84 pagesFINAL REPORT (L ND M)MuzamilNo ratings yet
- 5TH International Conference BrochureDocument5 pages5TH International Conference Brochureanup patwalNo ratings yet
- Thar Du Kan Calculation Report-13.02.2020 PDFDocument141 pagesThar Du Kan Calculation Report-13.02.2020 PDFZin Ko LinnNo ratings yet
- Multi-User Collaboration With Revit WorksetsDocument10 pagesMulti-User Collaboration With Revit WorksetsRafael Rafael CastilloNo ratings yet
- SC Judgment-Second AppealDocument29 pagesSC Judgment-Second AppealNarapa Reddy YannamNo ratings yet
- Brochure Thermoformer Range enDocument52 pagesBrochure Thermoformer Range enJawad LOUHADINo ratings yet