You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (842)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5806)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Mindfulness For Teens With ADHD - A Skill-Building Workbook To Help You Focus and Succeed PDFDocument234 pagesMindfulness For Teens With ADHD - A Skill-Building Workbook To Help You Focus and Succeed PDFMile Rojas100% (2)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Bioscalar EnergyDocument18 pagesBioscalar EnergyMarco Pauleau100% (1)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Contractor Safety Rules PDFDocument10 pagesContractor Safety Rules PDFKEERTHI INDUSTRIESNo ratings yet
- Near Miss ReportingDocument14 pagesNear Miss Reportingananthu.u100% (4)
- Yasmeen Sitxfa002Document35 pagesYasmeen Sitxfa002ranu jain100% (1)
- Training Needs Assessment For NursesDocument3 pagesTraining Needs Assessment For NursesRodel Sumiran100% (1)
- Book 1Document50 pagesBook 1Varudhini PatkiNo ratings yet
- Methodology - Hot WorksDocument5 pagesMethodology - Hot WorksPortia IbiasNo ratings yet
- Risk Analysis Template 08Document1 pageRisk Analysis Template 08Portia IbiasNo ratings yet
- Electric-And Magnetic-Field Measurements in An Outdoor Electric Power SubstationDocument6 pagesElectric-And Magnetic-Field Measurements in An Outdoor Electric Power SubstationPortia IbiasNo ratings yet
- Office: of The SecretaryDocument2 pagesOffice: of The SecretaryPortia IbiasNo ratings yet
- DOH Ao2020-0014Document40 pagesDOH Ao2020-0014Portia IbiasNo ratings yet
- Griffith, G. M., Totsika, V., Nash, S., & Hastings, R. P. (2011) - I Just Don"t Fit AnywhereDocument15 pagesGriffith, G. M., Totsika, V., Nash, S., & Hastings, R. P. (2011) - I Just Don"t Fit AnywhereTomislav CvrtnjakNo ratings yet
- Adaptacininstrumentos WASTDocument11 pagesAdaptacininstrumentos WASTAsley Cabrera LopezNo ratings yet
- Blended Learning 1 (Week 5)Document6 pagesBlended Learning 1 (Week 5)nurul syazwaniNo ratings yet
- S.L. 234.51 - MLCDocument94 pagesS.L. 234.51 - MLCJoseph Alexander BorgNo ratings yet
- Topic: Use of Antibiotic Therapy For Pediatric Dental PatientsDocument1 pageTopic: Use of Antibiotic Therapy For Pediatric Dental PatientsTenzin WangyalNo ratings yet
- Inclusivness AssignmentDocument17 pagesInclusivness AssignmentEphrem ChernetNo ratings yet
- Documents For Camp Attendance: I, Name....Document2 pagesDocuments For Camp Attendance: I, Name....Deva T N100% (1)
- Occupational Therapy Assessment: 1. SensesDocument17 pagesOccupational Therapy Assessment: 1. SensesVIJAYA DHARSHINI M Bachelor in Occupational Therapy (BOT)No ratings yet
- Full Length Research Article: ISSN: 2230-9926Document5 pagesFull Length Research Article: ISSN: 2230-9926Nisarg SutharNo ratings yet
- Traffic Signs ManualDocument334 pagesTraffic Signs Manualiwansalma100% (1)
- ABCDEFGHI Systematic Approach To Wound Assessment and ManagementDocument36 pagesABCDEFGHI Systematic Approach To Wound Assessment and ManagementsaerodinNo ratings yet
- BIOBASE SCSJ-V Series User ManualDocument25 pagesBIOBASE SCSJ-V Series User Manualsoporte03No ratings yet
- Communication and Nutrional EducationDocument11 pagesCommunication and Nutrional EducationSabrina PanjaitanNo ratings yet
- Concepts To MasterDocument10 pagesConcepts To MasterJessa HiquianaNo ratings yet
- Mediclear: Site Office - 90, Vasant Complex, Mayur Vihar, DelhiDocument3 pagesMediclear: Site Office - 90, Vasant Complex, Mayur Vihar, Delhiafsarkhan85No ratings yet
- The U.S. Virgin Islands Renewable and Alternative Energy Act of 2009Document28 pagesThe U.S. Virgin Islands Renewable and Alternative Energy Act of 2009Detlef LoyNo ratings yet
- Chinese GarterDocument3 pagesChinese Gartereden estrado mendoza100% (1)
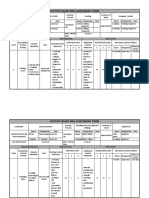
- Activity-Based Risk Assessment Form: Wearing InspectorDocument3 pagesActivity-Based Risk Assessment Form: Wearing InspectorSherly MagatNo ratings yet
- 01-10-13 EditionDocument28 pages01-10-13 EditionSan Mateo Daily JournalNo ratings yet
- 7.5.2.2 Final Report of Dumagat AuroraDocument127 pages7.5.2.2 Final Report of Dumagat AuroraAlvin HalconNo ratings yet
- Digi T Vigilance TestDocument6 pagesDigi T Vigilance TestJillianne FrancoNo ratings yet
- Faradic: Reference ManualDocument19 pagesFaradic: Reference ManualrobertNo ratings yet
- Vet Obst Lecture 2 Placenta Formation and GrowthDocument46 pagesVet Obst Lecture 2 Placenta Formation and GrowthgnpobsNo ratings yet