You might also like
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (844)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5814)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- March 2023 Recalls Solved by Nazia RafiqueDocument18 pagesMarch 2023 Recalls Solved by Nazia RafiqueelgafarypharmacyNo ratings yet
- Oncology MCQDocument61 pagesOncology MCQAwelfr100% (4)
- Lecture - Three (Pharma Marketing)Document44 pagesLecture - Three (Pharma Marketing)Sajid Ali MaariNo ratings yet
- Dr. Hari Paraton - Global Problem AMR - WS PPRA KARS Ed CPDocument28 pagesDr. Hari Paraton - Global Problem AMR - WS PPRA KARS Ed CPindriNo ratings yet
- Inhaler Storage and Expiration PDFDocument1 pageInhaler Storage and Expiration PDFMohammad AbushgairNo ratings yet
- Histamine and Antihistamines. NotesDocument5 pagesHistamine and Antihistamines. NotesSubha2000100% (1)
- Drugs Affecting Myometrium1 PDFDocument9 pagesDrugs Affecting Myometrium1 PDFЛариса ТкачеваNo ratings yet
- Immune System 14Document61 pagesImmune System 14Лариса ТкачеваNo ratings yet
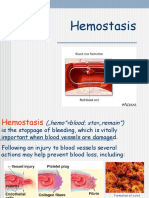
- Lecture HemostasisDocument28 pagesLecture HemostasisЛариса ТкачеваNo ratings yet
- Diseases of The Gastrointestinal TractDocument87 pagesDiseases of The Gastrointestinal TractЛариса ТкачеваNo ratings yet
- Leukocytosis. Leukopenia.: Lecture PresentationDocument23 pagesLeukocytosis. Leukopenia.: Lecture PresentationЛариса ТкачеваNo ratings yet
- Lecture LeukemiaDocument21 pagesLecture LeukemiaЛариса ТкачеваNo ratings yet
- PLT & Heamostasis (Autosaved)Document35 pagesPLT & Heamostasis (Autosaved)Лариса ТкачеваNo ratings yet
- One Compartment Model - Intravenous Bolus (Lecture 2)Document42 pagesOne Compartment Model - Intravenous Bolus (Lecture 2)Yamaan YamaanNo ratings yet
- Form 10 29012022Document81 pagesForm 10 29012022Lya WardaniNo ratings yet
- Kalbe Farma, TBK (Optima) UPDATE JULI 2023 - 1Document12 pagesKalbe Farma, TBK (Optima) UPDATE JULI 2023 - 1ekaputraantoNo ratings yet
- LetrozoleDocument2 pagesLetrozoleunkown userNo ratings yet
- Prescribing Information and Patient Medication Information: BuscopanDocument27 pagesPrescribing Information and Patient Medication Information: BuscopanMey KhNo ratings yet
- Sinarest Vapocap2018Document2 pagesSinarest Vapocap2018v mannNo ratings yet
- Mechanism of Action of Cariprazine 2016Document5 pagesMechanism of Action of Cariprazine 2016Fan TomasNo ratings yet
- OsteoporosisDocument15 pagesOsteoporosisWil LesterNo ratings yet
- Anti-Cholinergic Drugs: DR Naser Ashraf TadviDocument23 pagesAnti-Cholinergic Drugs: DR Naser Ashraf TadviVivek PandeyNo ratings yet
- Angiotensin Ii Receptor Blockers (ARBS) : Danielle Trisha L. MallariDocument7 pagesAngiotensin Ii Receptor Blockers (ARBS) : Danielle Trisha L. MallariTrisha MallariNo ratings yet
- Contoh Gol. Obat KIEDocument3 pagesContoh Gol. Obat KIEAndre D. Cahya100% (1)
- Advantages and Disadvantages of PowdersDocument1 pageAdvantages and Disadvantages of Powdersrawabi bakarmanNo ratings yet
- Final PPT NSTP Drug Addiction g1Document83 pagesFinal PPT NSTP Drug Addiction g1JovilleNo ratings yet
- DsaDocument4 pagesDsaChris NicodemusNo ratings yet
- Tablet PuzzleDocument3 pagesTablet PuzzleRaya Ibarra LumogdangNo ratings yet
- Catalogo de Precios Trasnacional 08-06-19Document52 pagesCatalogo de Precios Trasnacional 08-06-19darinelNo ratings yet
- Sulfamethaxazole, Salbu + IpraDocument5 pagesSulfamethaxazole, Salbu + IpraGwyn RosalesNo ratings yet
- AtenololDocument14 pagesAtenololAthena S FauziaNo ratings yet
- Ganaton SPCDocument8 pagesGanaton SPCNguyen Manh TuanNo ratings yet
- Antidotes 2 List 2011Document2 pagesAntidotes 2 List 2011Alpesh ValaNo ratings yet
- The Underlying Mechanisms of Drug AddictionDocument2 pagesThe Underlying Mechanisms of Drug AddictionWhere Did Macky GallegoNo ratings yet
- Role Play DiareDocument7 pagesRole Play DiareNi Putu aristaNo ratings yet
- Treatment of Corneal Ulcer MODIFIEDDocument6 pagesTreatment of Corneal Ulcer MODIFIEDapi-3700043No ratings yet
- Adrenergic Neuron BlockersDocument3 pagesAdrenergic Neuron BlockersSyeda Nishat Fathima TajNo ratings yet