You might also like
- Esthetic Oral Rehabilitation with Veneers: A Guide to Treatment Preparation and Clinical ConceptsFrom EverandEsthetic Oral Rehabilitation with Veneers: A Guide to Treatment Preparation and Clinical ConceptsRichard D. TrushkowskyNo ratings yet
- Int J of Prosthod Vol. 23 (1) Pp. 49-52 2010Document5 pagesInt J of Prosthod Vol. 23 (1) Pp. 49-52 2010LucianoNo ratings yet
- Molar Incisor Hypomineralization: A Clinical Guide to Diagnosis and TreatmentFrom EverandMolar Incisor Hypomineralization: A Clinical Guide to Diagnosis and TreatmentKatrin BekesNo ratings yet
- Study On Effect of Remaining Dentin Thickness and Coronal Pulp Size On Dentin Hypersensitivity Following Tooth PreparationDocument6 pagesStudy On Effect of Remaining Dentin Thickness and Coronal Pulp Size On Dentin Hypersensitivity Following Tooth Preparationashok ayerNo ratings yet
- 10 3290@j Qi A35700Document11 pages10 3290@j Qi A35700Radulescu MaraNo ratings yet
- Upto 12 Years Clinic Evaluation of 197 PartialDocument9 pagesUpto 12 Years Clinic Evaluation of 197 PartialDan MPNo ratings yet
- Quality of CAD‐CAM inlays placed on aged resin‐based composite restorations used as deep margin elevation: a laboratory studyDocument13 pagesQuality of CAD‐CAM inlays placed on aged resin‐based composite restorations used as deep margin elevation: a laboratory study6mp57dy74sNo ratings yet
- Influence of Preparation Design and Restorative Material On Fatigue and Fracture Strength of Restored Maxillary PremolarsDocument12 pagesInfluence of Preparation Design and Restorative Material On Fatigue and Fracture Strength of Restored Maxillary PremolarsDANTE DELEGUERYNo ratings yet
- Dental practice RCT compares efficacy of interventions for dentin hypersensitivityDocument7 pagesDental practice RCT compares efficacy of interventions for dentin hypersensitivityolalalalalalalalalalaNo ratings yet
- RK 1Document5 pagesRK 1dion leonardoNo ratings yet
- CLI2023 - Ferrando Total Rehabilitation Using Adhesive Dental Restoration in Patiens with Severe Tooth Wear A 5-Year Retrospective CaseDocument15 pagesCLI2023 - Ferrando Total Rehabilitation Using Adhesive Dental Restoration in Patiens with Severe Tooth Wear A 5-Year Retrospective Casecd.brendasotofloresNo ratings yet
- Effectiveness of A Desensitizing Agent Before In-Office Tooth Bleaching in Restored TeethDocument7 pagesEffectiveness of A Desensitizing Agent Before In-Office Tooth Bleaching in Restored TeethFer TorresNo ratings yet
- Comparative Desensitizing Effect of A Toothpaste and Mouthwash (Potassium Nitrate)Document7 pagesComparative Desensitizing Effect of A Toothpaste and Mouthwash (Potassium Nitrate)AsriDianSariNo ratings yet
- Retrieve 39Document23 pagesRetrieve 39Freddy BenalcázarNo ratings yet
- Moncada 2013Document10 pagesMoncada 2013Stefi MullerNo ratings yet
- Clinical Efectiveness of Restorative Materials For The RestorationDocument16 pagesClinical Efectiveness of Restorative Materials For The RestorationKruspkaya Sylvia Nieves Neira ValdezNo ratings yet
- Effect of Immediate Dentin Sealing in Prevention of PostCementation Hypersensitivity in Fullcoverage RestorationsDocument5 pagesEffect of Immediate Dentin Sealing in Prevention of PostCementation Hypersensitivity in Fullcoverage RestorationsIOSRjournalNo ratings yet
- ContentServer (1) .Asp-16Document14 pagesContentServer (1) .Asp-16ERIKA BLANQUETNo ratings yet
- Occlusal Onlay As Mordern RX PDFDocument13 pagesOcclusal Onlay As Mordern RX PDFSMART SMARNo ratings yet
- The Efficacy of Dental Sealant Used With Bonding Agent On Occlusal CariesDocument14 pagesThe Efficacy of Dental Sealant Used With Bonding Agent On Occlusal CariesJeanpareNo ratings yet
- [International Endodontic Journal 2017-Jul 26 Vol. 51] Nazzal, H_ Kenny, K_ Altimimi, A_ Kang, J_ Duggal, M S - A Prospective Clinical Study of Regenerative Endodontic Treatment of Traumatised Immature Teeth With NeDocument38 pages[International Endodontic Journal 2017-Jul 26 Vol. 51] Nazzal, H_ Kenny, K_ Altimimi, A_ Kang, J_ Duggal, M S - A Prospective Clinical Study of Regenerative Endodontic Treatment of Traumatised Immature Teeth With Neكرم الباريNo ratings yet
- Pin-Retained Restoration With Resin Bonded Composite of A Badly Broken ToothDocument3 pagesPin-Retained Restoration With Resin Bonded Composite of A Badly Broken ToothIOSRjournalNo ratings yet
- Histological Comparison of Pulpal Inflamation in Primary Teeth With Occlusal or Proximal CariesDocument8 pagesHistological Comparison of Pulpal Inflamation in Primary Teeth With Occlusal or Proximal CariesGilmer Solis SánchezNo ratings yet
- Artigo 1Document8 pagesArtigo 1joao pauloNo ratings yet
- Occurrence and Causing Stimuli of Postoperative Sensitivity in Composite Restorations PDFDocument8 pagesOccurrence and Causing Stimuli of Postoperative Sensitivity in Composite Restorations PDFDavid ColonNo ratings yet
- 3-14 Magne 2005Document9 pages3-14 Magne 2005Paula SotomayorNo ratings yet
- Journal Homepage: - : Manuscript HistoryDocument11 pagesJournal Homepage: - : Manuscript HistoryIJAR JOURNALNo ratings yet
- Article1404395371 - Shibu and RajanDocument3 pagesArticle1404395371 - Shibu and RajanRuchi ShahNo ratings yet
- Comparative Evaluation of Effect of Denture Adhesives On Retention ofDocument6 pagesComparative Evaluation of Effect of Denture Adhesives On Retention ofdentureNo ratings yet
- TMP BDD4Document7 pagesTMP BDD4FrontiersNo ratings yet
- Two-Implant-Supported Mandibular Overdentures: Do Clinical Denture Quality and Inter-Implant Distance Affect Patient Satisfaction?Document7 pagesTwo-Implant-Supported Mandibular Overdentures: Do Clinical Denture Quality and Inter-Implant Distance Affect Patient Satisfaction?Ahmad FadhilNo ratings yet
- Implant 1Document8 pagesImplant 1phungNo ratings yet
- sjogren1Document8 pagessjogren1mNo ratings yet
- Carranza's Clinical Periodontology 2002Document6 pagesCarranza's Clinical Periodontology 2002Lia Optimeze Alwayz100% (1)
- Int Endodontic J - 2022 - Matoug ElwerfelliDocument17 pagesInt Endodontic J - 2022 - Matoug Elwerfelliالحب الابديNo ratings yet
- Speroni Desplazamiento Paladar2010Document7 pagesSperoni Desplazamiento Paladar2010SergioNo ratings yet
- Table Top Tooth Wear - A Systematic Review of Treatment OptionsDocument8 pagesTable Top Tooth Wear - A Systematic Review of Treatment OptionsZardasht NajmadineNo ratings yet
- D L, H R & L L: Periodontology 2000Document24 pagesD L, H R & L L: Periodontology 2000ph4nt0mgr100% (1)
- Effect of Desensitizing Patch For Dentin Hypersensitivity: Su-Yeon Park, Mi-Ra Lee, Jin-Hee WonDocument7 pagesEffect of Desensitizing Patch For Dentin Hypersensitivity: Su-Yeon Park, Mi-Ra Lee, Jin-Hee WonIndah LestariNo ratings yet
- Edelhoff BDJ 2019Document10 pagesEdelhoff BDJ 2019Jose Manuel Quintero RomeroNo ratings yet
- Restoring Endodontically Treated TeethDocument20 pagesRestoring Endodontically Treated Teethlishenwong100% (1)
- Andersson 2003Document6 pagesAndersson 2003IngrydCamposNo ratings yet
- Stainless Steel Crowns in Pediatric Restorative Dentistry: Applications and AdvantagesDocument2 pagesStainless Steel Crowns in Pediatric Restorative Dentistry: Applications and AdvantagesYulia Asri EfendiNo ratings yet
- Apexification of Anterior Teeth: A Comparative Evaluation of Mineral Trioxide Aggregate and Calcium Hydroxide PasteDocument6 pagesApexification of Anterior Teeth: A Comparative Evaluation of Mineral Trioxide Aggregate and Calcium Hydroxide PastefatimahNo ratings yet
- Endodontic Retreatment Vs Dental ImplantsDocument17 pagesEndodontic Retreatment Vs Dental ImplantsEstefania VargasNo ratings yet
- Pulpotomy For Treatment of Complicated Crown FracturesDocument22 pagesPulpotomy For Treatment of Complicated Crown Fracturessystematic reviewNo ratings yet
- Ortodoncia y CarillasDocument4 pagesOrtodoncia y CarillasLiz StephanyNo ratings yet
- Journal of Dentistry: SciencedirectDocument10 pagesJournal of Dentistry: SciencedirectJAYASOORYAN S P M.D.S. CONSERVATIVE DENTISTRY AND ENDODONTICSNo ratings yet
- Effect of Light Activation On Tooh Sensitivity After in Officce BleachDocument7 pagesEffect of Light Activation On Tooh Sensitivity After in Officce BleachleiddyNo ratings yet
- Denture Adhesives Improve Denture PerformanceDocument2 pagesDenture Adhesives Improve Denture PerformancepaulinaNo ratings yet
- The Influence of Removable Partial Dentures On The Periodontal Health of Abutment and Non Abutment TeethDocument5 pagesThe Influence of Removable Partial Dentures On The Periodontal Health of Abutment and Non Abutment TeethAnthony OrtegaNo ratings yet
- Influence of Chlorhexidine Digluconate On The Clinical Performance of Adhesive Restorations - A 3-Year Follow-UpDocument9 pagesInfluence of Chlorhexidine Digluconate On The Clinical Performance of Adhesive Restorations - A 3-Year Follow-UpMelba RomNo ratings yet
- Clinical Evaluation of Failures in Removable Partial DenturesDocument6 pagesClinical Evaluation of Failures in Removable Partial DenturesAlina AlexandraNo ratings yet
- 1 s2.0 S0300571221001330 MainDocument10 pages1 s2.0 S0300571221001330 MainMairaMaraviChavezNo ratings yet
- Postoperative Sensitivity in Direct Resin CompositesDocument12 pagesPostoperative Sensitivity in Direct Resin CompositesKhalid G. AzouniNo ratings yet
- UntitledDocument25 pagesUntitledpritasya handayaniNo ratings yet
- 1clinical Evaluation of Failures of Removable Partial Dentures PDFDocument7 pages1clinical Evaluation of Failures of Removable Partial Dentures PDFcsmalxNo ratings yet
- Long-Term Survival of Indirect Pulp Treatment Performed in Primary and Permanent Teeth With Clinically Diagnosed Deep Carious LesionsDocument4 pagesLong-Term Survival of Indirect Pulp Treatment Performed in Primary and Permanent Teeth With Clinically Diagnosed Deep Carious LesionsBAHAMON TRUJILLO MAYRA ALEJANDRANo ratings yet
- Advance in MaterialsDocument10 pagesAdvance in Materialssami robalinoNo ratings yet
- MTA Pulpotomy As An Alternative To Root Canal Treatment in Children's Permanent Teeth in A Dental Public Health Setting.Document6 pagesMTA Pulpotomy As An Alternative To Root Canal Treatment in Children's Permanent Teeth in A Dental Public Health Setting.Abdul Rahman AlmishhdanyNo ratings yet
- 10 1016@j Jdent 2019 103227Document34 pages10 1016@j Jdent 2019 103227Marcelo CalimanNo ratings yet
- Articulo 4Document7 pagesArticulo 4Mile MolinaNo ratings yet
- Articulo PDFDocument4 pagesArticulo PDFMile MolinaNo ratings yet
- Articulo PDFDocument4 pagesArticulo PDFMile MolinaNo ratings yet
- Articulo 2Document7 pagesArticulo 2Mile MolinaNo ratings yet
- Ibuprodeno PDFDocument24 pagesIbuprodeno PDFMile MolinaNo ratings yet
- Grade 8 - P.E PPT (Week 1)Document30 pagesGrade 8 - P.E PPT (Week 1)Dave Sedigo100% (1)
- Scenar Testimonials (Updated)Document10 pagesScenar Testimonials (Updated)Tom Askew100% (1)
- Periodontal SurgeryDocument67 pagesPeriodontal SurgeryRifqa NoorNo ratings yet
- Medicaid Medical Record DocumentationDocument3 pagesMedicaid Medical Record DocumentationRam KumarNo ratings yet
- Syllabus ClinPhar143Document2 pagesSyllabus ClinPhar143Angel GoNo ratings yet
- Actemra Med GuideDocument5 pagesActemra Med GuideTrycNo ratings yet
- Emergency Medicine ST3 DRE-EM - 2024 Alternative CertificateDocument8 pagesEmergency Medicine ST3 DRE-EM - 2024 Alternative Certificateiffi82No ratings yet
- Date/ Time Cues Nursing Diagnosis Goals & Objectives Interventions Rationale EvaluationDocument2 pagesDate/ Time Cues Nursing Diagnosis Goals & Objectives Interventions Rationale EvaluationErica P. ManlunasNo ratings yet
- Hiv-Sle Case StudyDocument8 pagesHiv-Sle Case StudycathyNo ratings yet
- Virtual Planning of ImplantDocument6 pagesVirtual Planning of ImplantChekkarraj Sharanya KeshapurNo ratings yet
- Sensus Harian TGL 05 Maret 2022........Document104 pagesSensus Harian TGL 05 Maret 2022........Ruhut Putra SinuratNo ratings yet
- Work-Related Injuries and Illnesses: Osha Forms For RecordingDocument12 pagesWork-Related Injuries and Illnesses: Osha Forms For RecordingCollin GrayNo ratings yet
- S4.M22.HO-Assessing Apical PulseDocument2 pagesS4.M22.HO-Assessing Apical PulseNugraNo ratings yet
- Maternal and Child Nursing - Antepartum PeriodDocument102 pagesMaternal and Child Nursing - Antepartum Periodchuppepay50% (2)
- World English 3 Workbook World English Real People Real Places Real LanguageDocument2 pagesWorld English 3 Workbook World English Real People Real Places Real Languagejose luis0% (5)
- Diagnosis to Treatment PlanningDocument88 pagesDiagnosis to Treatment Planningsrinivaskalluri100% (1)
- Classification of DementiasDocument40 pagesClassification of Dementiasdrkadiyala2100% (1)
- Basic DefinitionDocument7 pagesBasic Definitionsamiurrehman4994No ratings yet
- Dr. Rohit Reejsinghani Appointed As Executive Director of New York HealthDocument2 pagesDr. Rohit Reejsinghani Appointed As Executive Director of New York HealthPR.comNo ratings yet
- National Oral Health Program GuidelinesDocument21 pagesNational Oral Health Program GuidelinesAniket PotnisNo ratings yet
- ENGLISH - Reading - Grammar. UNIT 5.Document14 pagesENGLISH - Reading - Grammar. UNIT 5.Angie ReyesNo ratings yet
- TOG 2023 Volume 25 Issue 3Document86 pagesTOG 2023 Volume 25 Issue 3saeed hasan saeedNo ratings yet
- Medicaliq Blogspot Com 2014-11-130 Top Epidemiology MultipleDocument25 pagesMedicaliq Blogspot Com 2014-11-130 Top Epidemiology MultipleRozen Tareque HasanNo ratings yet
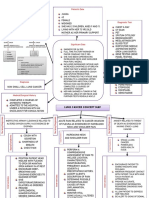
- Lung Cancer Concept Map-Group 2Document2 pagesLung Cancer Concept Map-Group 2Maria Cristina100% (2)
- ACCP Standards of PracticeDocument4 pagesACCP Standards of Practiceryuurecca0% (1)
- Asante Teaching Hospital Activity Based CostingDocument3 pagesAsante Teaching Hospital Activity Based CostingMuskanNo ratings yet
- Global Epidemiology of Hepatitis B Virus (HBV) Infection: Elizabeth W. Hwang, MD, Ramsey Cheung, MDDocument7 pagesGlobal Epidemiology of Hepatitis B Virus (HBV) Infection: Elizabeth W. Hwang, MD, Ramsey Cheung, MDivan gartikaNo ratings yet
- Clinical PharmacokineticsDocument31 pagesClinical PharmacokineticsArdiyanti Puspitasari100% (1)
- 2.standards of Midwifery PracticeDocument22 pages2.standards of Midwifery PracticeVeena DalmeidaNo ratings yet
- ASTHMADocument16 pagesASTHMAAyesigwa Gerald96100% (1)
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (17)
- Why We Die: The New Science of Aging and the Quest for ImmortalityFrom EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityRating: 4 out of 5 stars4/5 (3)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 5 out of 5 stars5/5 (78)
- The Obesity Code: Unlocking the Secrets of Weight LossFrom EverandThe Obesity Code: Unlocking the Secrets of Weight LossRating: 5 out of 5 stars5/5 (4)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsFrom EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNo ratings yet
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionFrom EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionRating: 4 out of 5 stars4/5 (403)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisFrom EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisRating: 4.5 out of 5 stars4.5/5 (42)
- 12 Rules for Life by Jordan B. Peterson - Book Summary: An Antidote to ChaosFrom Everand12 Rules for Life by Jordan B. Peterson - Book Summary: An Antidote to ChaosRating: 4.5 out of 5 stars4.5/5 (207)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsFrom EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsRating: 5 out of 5 stars5/5 (1)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeNo ratings yet
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsFrom EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsRating: 3.5 out of 5 stars3.5/5 (3)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsFrom EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsRating: 4.5 out of 5 stars4.5/5 (169)
- The Ultimate Guide To Memory Improvement TechniquesFrom EverandThe Ultimate Guide To Memory Improvement TechniquesRating: 5 out of 5 stars5/5 (34)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaFrom EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaRating: 4.5 out of 5 stars4.5/5 (266)
- Cult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryFrom EverandCult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryRating: 4 out of 5 stars4/5 (44)
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessFrom EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessRating: 4.5 out of 5 stars4.5/5 (328)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.From EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Rating: 4.5 out of 5 stars4.5/5 (110)
- Techniques Exercises And Tricks For Memory ImprovementFrom EverandTechniques Exercises And Tricks For Memory ImprovementRating: 4.5 out of 5 stars4.5/5 (40)
- The Happiness Trap: How to Stop Struggling and Start LivingFrom EverandThe Happiness Trap: How to Stop Struggling and Start LivingRating: 4 out of 5 stars4/5 (1)
- Algorithms to Live By: The Computer Science of Human DecisionsFrom EverandAlgorithms to Live By: The Computer Science of Human DecisionsRating: 4.5 out of 5 stars4.5/5 (722)
- Summary: How to Be an Adult in Relationships: The Five Keys to Mindful Loving by David Richo: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: How to Be an Adult in Relationships: The Five Keys to Mindful Loving by David Richo: Key Takeaways, Summary & Analysis IncludedRating: 4 out of 5 stars4/5 (11)
- Gut: the new and revised Sunday Times bestsellerFrom EverandGut: the new and revised Sunday Times bestsellerRating: 4 out of 5 stars4/5 (392)
- When the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisFrom EverandWhen the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisRating: 3.5 out of 5 stars3.5/5 (2)




















![[International Endodontic Journal 2017-Jul 26 Vol. 51] Nazzal, H_ Kenny, K_ Altimimi, A_ Kang, J_ Duggal, M S - A Prospective Clinical Study of Regenerative Endodontic Treatment of Traumatised Immature Teeth With Ne](https://imgv2-2-f.scribdassets.com/img/document/649306081/149x198/6cdc9cdd33/1685435519?v=1)