You might also like
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5813)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (844)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- WBB Business PlanDocument23 pagesWBB Business Planapi-582613784100% (1)
- Critical Literature ReviewDocument55 pagesCritical Literature Reviewcth_yao100% (1)
- ABM-APPLIED ECONOMICS 12 - Q1 - W1 - Mod1Document16 pagesABM-APPLIED ECONOMICS 12 - Q1 - W1 - Mod1Carmilleah Freyjah94% (70)
- 1Z0-338 Dumps - Oracle Exadata Database Machine ExamDocument8 pages1Z0-338 Dumps - Oracle Exadata Database Machine ExamThomas William29% (7)
- English 3 WHLP Q1 Module 7Document2 pagesEnglish 3 WHLP Q1 Module 7RM BatulanNo ratings yet
- Dhiraj SOPDocument7 pagesDhiraj SOPAakankshya AwasthiNo ratings yet
- Literature Review s2 Handout PDFDocument23 pagesLiterature Review s2 Handout PDFFirsty MendrofaNo ratings yet
- Prof. Dr. Moustapha Ibrahim Salem Mansourms@alexu - Edu.eg 01005857099Document34 pagesProf. Dr. Moustapha Ibrahim Salem Mansourms@alexu - Edu.eg 01005857099Ahmed ElsayedNo ratings yet
- Ksa Design Thinking For HR Professionals 2020 PDFDocument5 pagesKsa Design Thinking For HR Professionals 2020 PDFHamid OtaifNo ratings yet
- Problem of Child Labour in India and Its Causes:: With Special Reference To The State of AssamDocument14 pagesProblem of Child Labour in India and Its Causes:: With Special Reference To The State of AssamRaajdwip VardhanNo ratings yet
- Eca Syllabus F Nstp1 Maritime 2021Document13 pagesEca Syllabus F Nstp1 Maritime 2021Christopher Dela cruzNo ratings yet
- Language Choice in Note-Taking For C-E Consecutive InterpretingDocument11 pagesLanguage Choice in Note-Taking For C-E Consecutive InterpretingHasan Can BıyıkNo ratings yet
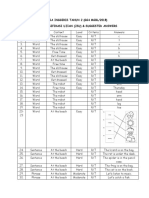
- Bahasa Inggeris Tahun 2 (Gg4 Mgbl/2018) Jadual Spesifikasi Ujian (Jsu) & Suggested AnswersDocument2 pagesBahasa Inggeris Tahun 2 (Gg4 Mgbl/2018) Jadual Spesifikasi Ujian (Jsu) & Suggested AnswersDayangku EffaNo ratings yet
- Resume For Eng 302Document1 pageResume For Eng 302api-239721669No ratings yet
- Book List SSSVV Senior School 2022-23Document17 pagesBook List SSSVV Senior School 2022-23Mokshita JainNo ratings yet
- Humanistic Learning Theory BastableDocument5 pagesHumanistic Learning Theory BastableNikki RicafrenteNo ratings yet
- 86 - PDFsam - Kupdf - Net - Techniques and Materials of MusicDocument5 pages86 - PDFsam - Kupdf - Net - Techniques and Materials of Musicpaco desantisNo ratings yet
- Mathematics 10 PercentilesDocument3 pagesMathematics 10 PercentilesVina Amor GastonNo ratings yet
- Kri Per CV12Document9 pagesKri Per CV12Nelum PereraNo ratings yet
- Subject: Science Topic: Earth and Space Class: II Date: .11.2016Document2 pagesSubject: Science Topic: Earth and Space Class: II Date: .11.2016Saira Irfan - 50270/TCHR/BF-PRINo ratings yet
- Comparative and Superlative AdjectivesDocument4 pagesComparative and Superlative Adjectivesفاطمة الزهراءNo ratings yet
- Thesis On Indian Education SystemDocument8 pagesThesis On Indian Education Systemgbxwghwb100% (2)
- AttalahDocument1 pageAttalahapi-641152423No ratings yet
- IAT100 Week 1 SlidesDocument33 pagesIAT100 Week 1 SlidesFrank ChenNo ratings yet
- Historical and Contemporary Views of LanguageDocument24 pagesHistorical and Contemporary Views of LanguageAlonso GaxiolaNo ratings yet
- RA 4670 Magna Carta For Public School TeachersDocument5 pagesRA 4670 Magna Carta For Public School TeachersLeah DiongcoNo ratings yet
- 2021 Prisma ActualizadoDocument12 pages2021 Prisma Actualizadomaria murciaNo ratings yet
- Zhang Siqi CVDocument2 pagesZhang Siqi CVapi-636694152No ratings yet
- English 10TH Abc Guide 6 PDFDocument5 pagesEnglish 10TH Abc Guide 6 PDFYecica DiazNo ratings yet
- Sarah SulmanDocument1 pageSarah Sulmanapi-679123934No ratings yet