You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5813)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (844)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Basics of DentistryDocument206 pagesBasics of Dentistry84Dreamer75% (4)
- Cellulitis: A.prof. Keam Born. Dental Department of Khmer Soviet Friendship HospitalDocument183 pagesCellulitis: A.prof. Keam Born. Dental Department of Khmer Soviet Friendship HospitalRaksmey PhanNo ratings yet
- Notes 2.0Document56 pagesNotes 2.0ploy_sciNo ratings yet
- Oral Midterm 1Document48 pagesOral Midterm 1yalahopa0% (1)
- Diagnosis of Acute Periodontal LesionsDocument14 pagesDiagnosis of Acute Periodontal Lesionsczarisse escalonaNo ratings yet
- Pattern and Causes of Tooth Extraction in Patients Reporting To A Teaching Dental HospitalDocument6 pagesPattern and Causes of Tooth Extraction in Patients Reporting To A Teaching Dental HospitalAnye PutriNo ratings yet
- Stomatology ReviewDocument17 pagesStomatology Reviewarya kumarNo ratings yet
- Ijerph 18 06796 v2Document24 pagesIjerph 18 06796 v2paolaNo ratings yet
- Preface: Oral Maxillofacial Surg Clin N Am 19 (2007) XiDocument139 pagesPreface: Oral Maxillofacial Surg Clin N Am 19 (2007) XiZainab SalmanNo ratings yet
- Introduction To DentistryDocument13 pagesIntroduction To DentistryDr-Rmz RabadiNo ratings yet
- PERICORONITISDocument11 pagesPERICORONITISudayNo ratings yet
- Odontektomi Bahan Diskusi Od KoasDocument51 pagesOdontektomi Bahan Diskusi Od Koaspanjidrg100% (1)
- Guidelines For Referral of Patients To Oral and Maxillofacial SurgeryDocument4 pagesGuidelines For Referral of Patients To Oral and Maxillofacial SurgeryVictor YuNo ratings yet
- Abscess of THE PeriodontiumDocument57 pagesAbscess of THE PeriodontiumSandeep SunilNo ratings yet
- Management of Pericoronitis-Operculectomy: Dr. Sophia Saud InternDocument23 pagesManagement of Pericoronitis-Operculectomy: Dr. Sophia Saud InternSophia SaudNo ratings yet
- Acute Periodontal Conditions: PeriodonticsDocument9 pagesAcute Periodontal Conditions: Periodonticsmonica896No ratings yet
- Parameters of Care Supplement: Parameter On Acute Periodontal DiseasesDocument4 pagesParameters of Care Supplement: Parameter On Acute Periodontal DiseasesThaisOliveiraNo ratings yet
- The Piezoelectric and Rotatory Osteotomy Technique in Impacted Third Molar Surgery: Comparison Of..Document6 pagesThe Piezoelectric and Rotatory Osteotomy Technique in Impacted Third Molar Surgery: Comparison Of..Hoàng VũNo ratings yet
- Watbson R. 2011 PDFDocument8 pagesWatbson R. 2011 PDFFelipe RoncerosNo ratings yet
- PerikoronitisDocument5 pagesPerikoronitisNadira NurinNo ratings yet
- 6 Acute Gingival InfectionsDocument20 pages6 Acute Gingival Infectionssepehr_rasekh100% (3)
- Mcqs in Facial Spaces Infection @USFDocument7 pagesMcqs in Facial Spaces Infection @USFM.R PsychopathNo ratings yet
- Gingiva Diseases Of89Document3 pagesGingiva Diseases Of89محمد العراقيNo ratings yet
- SurgeryDocument109 pagesSurgeryEman ShahinNo ratings yet
- Acute Gingival InfectionsDocument38 pagesAcute Gingival Infectionshoormunaf8No ratings yet
- DENT 153 Trans 2-1 Principles of Tooth ExtractionDocument9 pagesDENT 153 Trans 2-1 Principles of Tooth ExtractionNianne Carla HernandezNo ratings yet
- Antibiotic Therapy PericoronitisDocument2 pagesAntibiotic Therapy PericoronitisMaulidahNo ratings yet
- Augmentin EffectsDocument39 pagesAugmentin EffectsJasmeen SutariyaNo ratings yet
- Oral Surgery 2 Prelims 1Document27 pagesOral Surgery 2 Prelims 1Ken HoiNo ratings yet
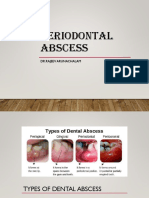
- Periodontal Abscess: DR - Rajeev ArunachalamDocument44 pagesPeriodontal Abscess: DR - Rajeev Arunachalamdamien teeNo ratings yet