One of the most critical issues regarding 2019 nCoV patients is the transitory invasive ventilator support, an elective
tive endotracheal intubation should be
AIRWAY
phase between initial symptoms and potentially severe evolution requiring preferred,or even anticipated, rather than waiting for an emergency procedure
critical care, while taking into account the comorbidities. The choice of (in the precipitating patient) as to minimize complications of intubation itself
supplementary oxygen delivery interface and the decision to provide invasive and also to reduce both the risks of procedural errors and the contamination of
ventilatory support is crucial. healthcare providers.
MANAGEMENT
These decisions have the potential of impacting outcome and may lead to Adoption of early warning scores (EWS), shared and predefined strategies,
consequences on saturation of critical care beds. multidisciplinary team training and simulation of possible scenarios are highly
Non-invasive support methods (CPAP, BiPAP, NIV, HFNO) might correct recommended, taking also into account the available levels of care and feasibility
hypoxemia and counterbalance respiratory failure (though univocal data are of critical care levels of assistance in a non-ICU environment.
missing) and may either delay or avoid endotracheal intubation (with potential The decisional elements for airway management, oxygenation and invasive
complications and effects on outcome). Nevertheless, data from the SARS ventilator support thus include competencies and organization and available
epidemic provide evidence showing that these ventilatory techniques might human and environmental resources.
favor the risk of airborne viral spreading. Given the nature of nCoV 19 in terms Vigilance in prevention, strict adhesion of donning/doffing of PPE, preparedness
of contagiousness, should the patient require, or be expected to necessitate for the care of infected patients remain priority and of utmost importance.
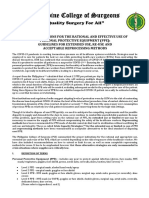
HIGHLIGHTS CLINICAL CHECKLIST (wearing PPE) TUBE POSITION CONTROL -
PROTECTIVE VENTILATION
COVID-19
▶ COMPLETE EVALUATION OF AIRWAYS AND OXYGENATION
▶ INTEGRATED COMPETENCIES FOR EVERY PHASE/STEP (accept difficult airway management risk overestimation)
▶ CAPNOGRAFIC CURVES repeated and with standard morphology
▶ AIRBORNE PROTECTION FOR EVERY PHASE/STEP ▶ HEMODYNAMIC EVALUATION • PRE-EMPTIVE HEMODYNAMIC (if in doubt take it out)
OPTIMIZATION
▶ ANTICIPATE NEEDS, MAXIMIZE FIRST-PASS SUCCESS ▶ AVOID unuseful circuit disconnections (if needed: ventilator on
stand-by/clamp endotracheal tube)
AIRWAY INSTRUMENTATION
DOUBLE-CHECK INDICATIONS ▶ CONSIDER indications for advanced techniques:
▶ HME FILTER ON EVERY OXYGENATION INTERFACE ECMO - experts advise
FOR ENDOTRACHEAL INTUBATION (face mask, circuit, endotracheal tube, supraglottic airway devices,
▶ Adopt Early Warning Scores for intubation/quod vitam prognosis introducer, airway exchange catheters)
(consider DNR cases)
▶ AIRWAY CART READY (DISPOSABLE devices preferable)
▶ Identify negative pressure environment
▶ SUCTION: CLOSED SYSTEM
▶ Balance benefits of CPAP/BiPAP/NIV/HFNO versus risks
PPE DOFFING
▶ ANTIFOGGING
of airborne diffusion ▶ During and after PPE doffing, hands hygiene mandatory
▶ MEDICATIONS: PREPARED AND DOUBLE-CHECKED
▶ IF INTUBATION is required, prefer ELECTIVE procedure
▶ Donning/doffing observer externally checking, individual doffing
(in emergency >> patient risk) ▶ EMERGENCY CART READY (DISPOSABLE devices preferable)
▶ Waste disposal
AWAKE INTUBATION NOT INDICATED:
TEAM PREPARATION ▶ PREOXYGENATION
(according to respiratory and hemodynamic status)
▶Minimize the number of team members: · 3min’ at TV FiO2=100% TRANSPORT
11) The most expert team member should perform the intubation or 1min’ at FVC 8 breaths FiO2=100%
or CPAP/PSV 10 cm H2O + PEEP 5 cm H2O FiO2=100% ▶ Follow bio-containment regulations
and advanced airway control/ventilation (with donned PPE)
[INSIDE the chamber] ▶ RSI in all patients (limit BMV unless unavoidable and apply Cricoid
2 EXPERT assistant on protocols and devices Pressure only in case of ongoing regurgitation)
(doctor/nurse with donned PPE) [INSIDE the chamber] ▶ NASAL PRONGS 3 LT/MIN FIO2=100% FOR APNOIC PHASE S - Secure airway: anticipated intubation
Reference
Wang C, Horby PW, Hayden FG, Gao GF (2020). A novel co-
ronavirus outbreak of global health concern. The Lancet,
3 Second doctor with donned PPE if complex maneuver/difficult
(NODESAT)
T - Team briefing
airway is expected/planned [INSIDE the chamber] ▶ FULL DOSE NEUROMUSCULAR BLOCK
395(10223), 470–473
Centers for Disease Control and Prevention. Coronavirus. RESPECT onset time for laryngoscopy O - Organize (competencies - team - pathways)
https://www.cdc.gov/coronavirus/ about/index.html. 4 Doctor available with donned PPE [OUTSIDE the chamber]
Accessed February 2020 1st LARYNGOSCOPY: P - Prepare (devices)
Livingston E, Bucher K, Rekito A. Coronavirus Disease 2019 5 PPE donning/doffing Observer [OUTSIDE] prefer VIDEOLARYNGOSCOPE with separate screen
and Influenza. JAMA. Published online February 26, 2020.
+ endotracheal tube pre-loaded on introducer
doi:10.1001/jama.2020.2633
WHO - Clinical management of severe acute respiratory CARRY OUT PRELIMINARY BRIEFING FOR ROLE DEFINITION, Re-oxygenate with low TV/pressure between attempts -Early switch
C - Checklist - controls- crisis management
infection when Novel coronavirus (2019-nCoV) infection is
suspected: Interim Guidance. STRATEGY DEFINITION, IDENTIFICATION OF DONNING/DOFFING
OBSERVER
(after failed second attempt) to supraglottic airway devices
(prefer second generation - intubable SADs)
O - Optimize (hemodynamics - oxygenation)
Jansson M, Liao X, Rello J. Strengthening ICU health
security for a coronavirus epidemic. Intensive Crit Care
Nurs. 2020 Feb 7:102812. doi: 10.1016/j.iccn.2020.102812 INTUBATION THROUGH SUPRAGLOTTIC AIRWAY DEVICES:
V - Vigilated donning/doffing
Phelan AL, Katz R, Gostin LO.The novel coronavirus flexible endoscope with separate screen (prefer DISPOSABLE) I - Invasive airways - evaluation and integrated airway management
originating in Wuhan, China: challenges for global health
governance. JAMA. Published online January 30, 2020. PPE DONNING
doi:10.1001/jama.2020.1097
▶ Second level PPE (airway management)
▶ EARLY CRICOTHYROTOMY IF CI-CO
D - Debriefing
Wax RS, Christian MD. Practical recommendations for
critical care and anesthesiology teams caring for novel
coronavirus (2019-nCoV) patients. Can J Anaesth. 2020 Feb
FFP3, facial shield, long sleeve fluid-resistant scrubs, AWAKE INTUBATION INDICATED (only if really mandatory):
12. doi: 10.1007/s12630-020-01591-x double gloves, overshoes
Hongbo Zheng, Wenlong Yao, Li Xu, Xiaohui, Chi, Wei
▶ AIRWAY TOPICALIZATION: no aerosol/vaporization
Mei. Current Protocol for Emergent Tracheal Intubation in ▶ Third level PPE (aerosol generating procedures - bronchoscopy,
Patients with 2019 novel coronavirus (COVID-19) Pneumo- ▶ TITRATED SEDATION (INFUSION PUMP) - sedation depth monitoring
nia Department of Anesthesiology, Tongji Hospital, Tongji awake endotracheal intubation, etc..) helmet in place of FFP3, facial
Medical College, Huazhong University of Science and
Technology, Wuhan, Hubei, China
shield, long sleeve fluid-resistant scrubs, double gloves, overshoes ▶ FLEXIBLE ENDOSCOPE WITH SEPARATE SCREEN
YuI T, Li Y, Wong TW, et al. Evidence of airborne transmis-
(PREFER DISPOSABLE)
sion of the severe acute respiratory syndrome virus. N Engl DONNING/DOFFING OBSERVER EXTERNALLY CHECKING,
J Med. 2004;350(17):1731- 1739
INDIVIDUAL DONNING ▶ RESCUE: INTUBATION THROUGH SUPRAGLOTTIC AIRWAY DEVICES
Peng, Philip W.H. et al. Outbreak of a new coronavirus: (see above) Massimiliano Sorbello, Ida Di Giacinto, Filippo Bressan, Flavia Petrini
what anaesthetists should know. British Journal of
Anaesthesia. In press. doi: https://doi.org/10.1016/j.
on behalf SIAARTI Airway Management Research Group
bja.2020.02.008 ▶ EARLY CRICOTHYROTOMY if CI-CO
You might also like
- Thinking SpellingDocument13 pagesThinking SpellingWendy Walker100% (1)
- Plan de Lectie - Perfectul SimpluDocument11 pagesPlan de Lectie - Perfectul SimpluDiana Hogea-ȚuscanuNo ratings yet
- (Online Teaching) A2 Flyers Speaking Part 1Document8 pages(Online Teaching) A2 Flyers Speaking Part 1MahekNo ratings yet
- Instrumen K3 PermenkesDocument95 pagesInstrumen K3 Permenkesangga_progrestNo ratings yet
- Highlights Clinical Checklist (Wearing Ppe) : Tube Position Control - Protective VentilationDocument1 pageHighlights Clinical Checklist (Wearing Ppe) : Tube Position Control - Protective VentilationIacriNo ratings yet
- Tx. COVID 19 en UCIDocument6 pagesTx. COVID 19 en UCIVictor Augusto Ávila HernándezNo ratings yet
- Decision Tree For Level 1 Patient Management: WWW - Health.gov - AuDocument3 pagesDecision Tree For Level 1 Patient Management: WWW - Health.gov - AuPepo BelovedNo ratings yet
- Anesthesia For Tracheolaryngeal Surgeries ENTDocument6 pagesAnesthesia For Tracheolaryngeal Surgeries ENTMaryamMahmoodNo ratings yet
- Estrategias Modernas de Ventilación Mecánica para El Cirujano de Cuidados Intensivos: Lo Que Necesita SaberDocument14 pagesEstrategias Modernas de Ventilación Mecánica para El Cirujano de Cuidados Intensivos: Lo Que Necesita SaberRousNo ratings yet
- Perrone 2020 Operating Room Setup How To ImproveDocument5 pagesPerrone 2020 Operating Room Setup How To ImproveMahadi Hasan KhanNo ratings yet
- Jama Kibbe 2020 VP 200172 1600712179.77638Document2 pagesJama Kibbe 2020 VP 200172 1600712179.77638Gleice ReinertNo ratings yet
- Permanent Pacemaker TechniqueDocument7 pagesPermanent Pacemaker TechniqueMonica TrifitrianaNo ratings yet
- Jama Murthy 2020 It 200008Document2 pagesJama Murthy 2020 It 200008jorgeNo ratings yet
- Jurding KLP A Anes 3Document18 pagesJurding KLP A Anes 3mreza26No ratings yet
- Care For Critically Ill Patients With COVID-19: Clinical UpdateDocument2 pagesCare For Critically Ill Patients With COVID-19: Clinical UpdateNicole BatistaNo ratings yet
- Target: Coronavirus Case Management InstructionsDocument4 pagesTarget: Coronavirus Case Management Instructionsapi-599439881No ratings yet
- 2019 Diaphragm Protection What Should We TargetDocument6 pages2019 Diaphragm Protection What Should We TargetwilsonmauriciolozanoNo ratings yet
- Emergency Room Safer Transfer ofDocument8 pagesEmergency Room Safer Transfer ofHerdy AdrianoNo ratings yet
- Braga Et Al 2019 Clinical Implications of Febrile Neutropenia Guidelines in The Cancer Patient PopulationDocument3 pagesBraga Et Al 2019 Clinical Implications of Febrile Neutropenia Guidelines in The Cancer Patient PopulationRafael SuzukiNo ratings yet
- Doc-20240131-Wa0 240131 224057Document4 pagesDoc-20240131-Wa0 240131 22405722alhumidi2020No ratings yet
- Weaning Francesas AICM 2019Document7 pagesWeaning Francesas AICM 2019Ana Miryam Pérez ZavalaNo ratings yet
- Tay 2020Document2 pagesTay 2020Corin Boice TelloNo ratings yet
- BJA 2017 Anaesthesia For Laryngo-Tracheal SurgeryDocument7 pagesBJA 2017 Anaesthesia For Laryngo-Tracheal SurgerySalomon Bongi NamupoloNo ratings yet
- COVID 19 and ENT SurgeryDocument6 pagesCOVID 19 and ENT SurgeryYukiko CalimutanNo ratings yet
- Guía 2019 de Intubación y Extubación Francesa 2019Document7 pagesGuía 2019 de Intubación y Extubación Francesa 2019Rafael Edgar Aguilar Bandala ChaparrinNo ratings yet
- COVID-19 Management in HongKongDocument1 pageCOVID-19 Management in HongKongShahzad KamranNo ratings yet
- Perioperative Considerstions in Urgent Surgical Care of Suspected and Confirmed COVID-19 Orthopaedic PatientsDocument23 pagesPerioperative Considerstions in Urgent Surgical Care of Suspected and Confirmed COVID-19 Orthopaedic PatientsDoctor's BettaNo ratings yet
- Economic Evaluation Alongside The Probiotics To Prevent Severe Pneumonia and Endotracheal Colonization Trial (E-PROSPECT) : Study ProtocolDocument8 pagesEconomic Evaluation Alongside The Probiotics To Prevent Severe Pneumonia and Endotracheal Colonization Trial (E-PROSPECT) : Study ProtocolSharan SahotaNo ratings yet
- Doc-20240131-Wa0 240131 224212Document3 pagesDoc-20240131-Wa0 240131 22421222alhumidi2020No ratings yet
- Who 2019 Ncov Ipc Ppe Use 2020.3 EngDocument28 pagesWho 2019 Ncov Ipc Ppe Use 2020.3 EngKumanan1304No ratings yet
- RRL 1Document5 pagesRRL 1Boy MadNo ratings yet
- Protocolos Weaining 2011Document14 pagesProtocolos Weaining 2011perla islasNo ratings yet
- Asv en NiñosDocument7 pagesAsv en Niñosjuan suarezNo ratings yet
- Prediction of Difficult Mask Ventilation: Clinical InvestigationsDocument8 pagesPrediction of Difficult Mask Ventilation: Clinical InvestigationsdiandianNo ratings yet
- Effectiveness-Matters-August-2014-Falls in HospitalsDocument4 pagesEffectiveness-Matters-August-2014-Falls in HospitalsKibsJohnNo ratings yet
- Current Problems in Diagnostic Radiology 50 (2021) 284 287Document4 pagesCurrent Problems in Diagnostic Radiology 50 (2021) 284 287Leonard AcsinteNo ratings yet
- Management of The Agitated Intensive Care Unit PatientDocument27 pagesManagement of The Agitated Intensive Care Unit PatientBEREKETNo ratings yet
- 2015 LeeuwenbergDocument10 pages2015 LeeuwenbergPaulHerreraNo ratings yet
- Lagier2022 Atelectasia en AnestesiologiaDocument31 pagesLagier2022 Atelectasia en AnestesiologiaNicolas SuarezNo ratings yet
- Diaphragm Protection: What Should We Target?: ReviewDocument6 pagesDiaphragm Protection: What Should We Target?: ReviewFernando SousaNo ratings yet
- A V: D D S, C, D, A M P: The Johns Hopkins Hospital Interdisciplinary Clinical Practice ManualDocument2 pagesA V: D D S, C, D, A M P: The Johns Hopkins Hospital Interdisciplinary Clinical Practice ManualIsworo RukmiNo ratings yet
- Is Zero Ventilator-Associated Pneumonia Achievable? Updated Practical Approaches To Ventilator - Associated Pneumonia PreventionDocument22 pagesIs Zero Ventilator-Associated Pneumonia Achievable? Updated Practical Approaches To Ventilator - Associated Pneumonia PreventionCarlos Hernan Castañeda RuizNo ratings yet
- Effects of Aggressive and Conservative Strategies For Mechanical Ventilation LiberationDocument9 pagesEffects of Aggressive and Conservative Strategies For Mechanical Ventilation LiberationGurmeet SinghNo ratings yet
- Jurnal Deskriptif IngDocument6 pagesJurnal Deskriptif IngAulin putri damayantiNo ratings yet
- COVID:10 Rationale Use of PPEDocument11 pagesCOVID:10 Rationale Use of PPEKristalyn RegaspiNo ratings yet
- Multimodal PDFDocument11 pagesMultimodal PDFCarlos CahuayaNo ratings yet
- Postoperative Pulmonary Complications and Their PreventionDocument9 pagesPostoperative Pulmonary Complications and Their PreventionMariana Brízido AptxNo ratings yet
- PIIS0003999320302951Document3 pagesPIIS0003999320302951Adiel CarrascoNo ratings yet
- Journal of Taibah University Medical SciencesDocument9 pagesJournal of Taibah University Medical SciencesrobertoNo ratings yet
- Environmental Controls in Operating Theatres: S. Dharan and D. PittetDocument6 pagesEnvironmental Controls in Operating Theatres: S. Dharan and D. PittetDinda FSNo ratings yet
- Lagier 2022Document31 pagesLagier 2022Carlos Daniel AliagaNo ratings yet
- Jocn 15753-DikonversiDocument16 pagesJocn 15753-DikonversiAlfa DexterNo ratings yet
- CCJM 87a ccc033 FullDocument4 pagesCCJM 87a ccc033 FullKamar Operasi Hermina BogorNo ratings yet
- Telemedicine in The Era of The COVID-19 Pandemic: Implications in Facial Plastic SurgeryDocument3 pagesTelemedicine in The Era of The COVID-19 Pandemic: Implications in Facial Plastic Surgerytresy kalawaNo ratings yet
- Intraop MV and PPC After CC Anest 2019Document17 pagesIntraop MV and PPC After CC Anest 2019Jenny ACNo ratings yet
- Predictive Value of The Negative Inspiratory ForceDocument8 pagesPredictive Value of The Negative Inspiratory ForceTam HmNo ratings yet
- Airway Assessment: Physical ExaminationDocument4 pagesAirway Assessment: Physical ExaminationTrọng MPNo ratings yet
- Ophthalmological Care Management of Cataract.16Document1 pageOphthalmological Care Management of Cataract.16library SDHBNo ratings yet
- Isolation Precaution Persi YohanaDocument13 pagesIsolation Precaution Persi YohanalasmariaNo ratings yet
- Mja2 50598Document10 pagesMja2 50598Andi Astrid AmaliaNo ratings yet
- Consensus Statement: Safe Airway Society Principles of Airway Management and Tracheal Intubation Specific To The COVID-19 Adult Patient GroupDocument10 pagesConsensus Statement: Safe Airway Society Principles of Airway Management and Tracheal Intubation Specific To The COVID-19 Adult Patient GroupMeska AmeliaNo ratings yet
- Burns Karen e A Non Invasive Ventilation VersusDocument10 pagesBurns Karen e A Non Invasive Ventilation VersusIsabel VillalobosNo ratings yet
- BJSTR MS Id 006919Document22 pagesBJSTR MS Id 006919Anz JoyNo ratings yet
- RA-013205 - MASTER PLUMBER - Manila - 2-2022Document112 pagesRA-013205 - MASTER PLUMBER - Manila - 2-2022Rainier VillanuevaNo ratings yet
- Spe 98108 PaDocument12 pagesSpe 98108 PaKacha SmitNo ratings yet
- Financial MGT FormulaDocument3 pagesFinancial MGT FormulaMahbub Zaman AshrafiNo ratings yet
- AGI Accounting FraudDocument9 pagesAGI Accounting Fraudayushaslaliya110No ratings yet
- Management Audit in Different FunctionsDocument25 pagesManagement Audit in Different FunctionsRaj SharmaNo ratings yet
- 28th Sunday in Ordinary TimeDocument3 pages28th Sunday in Ordinary TimeUniversity Catholic Center Austin, TXNo ratings yet
- 6.4.1 Institutional Strategies For Mobilization of Funds and The Optimal Utilization of ResourcesDocument10 pages6.4.1 Institutional Strategies For Mobilization of Funds and The Optimal Utilization of ResourcesiyalazhaguNo ratings yet
- Pelikan Et Al HARC 2014Document54 pagesPelikan Et Al HARC 2014Jennifer AstridNo ratings yet
- Philippine Grid Code: What?Document12 pagesPhilippine Grid Code: What?Ian DimalantaNo ratings yet
- Curriculum Vitae: Personal DetailsDocument3 pagesCurriculum Vitae: Personal DetailsAlfinsyahNo ratings yet
- HV-MX100: Simple ManualDocument28 pagesHV-MX100: Simple ManualSimon PapukyanNo ratings yet
- KLS Gogte Institute of Technology, Belagavi.: "F Distribution"Document15 pagesKLS Gogte Institute of Technology, Belagavi.: "F Distribution"2GI20MCA87Sushma MerawadeNo ratings yet
- C++ CLR DocsDocument1,156 pagesC++ CLR DocsVictor TihoanNo ratings yet
- Sella TurcicaDocument4 pagesSella TurcicaHeidar ZaarourNo ratings yet
- Empire of The Petal Throne Fiefs of The Kurt Hills Atlas RegionDocument21 pagesEmpire of The Petal Throne Fiefs of The Kurt Hills Atlas RegionSendral OrokNo ratings yet
- Exploratory Data Analysis On Indian Economy Using PythonDocument12 pagesExploratory Data Analysis On Indian Economy Using PythonIJRASETPublicationsNo ratings yet
- Intelligent Metering and Control Devices: Applications Summary Features SummaryDocument8 pagesIntelligent Metering and Control Devices: Applications Summary Features SummaryjocemirferstNo ratings yet
- The Greatest of All Time Leonardo Da VinciDocument62 pagesThe Greatest of All Time Leonardo Da VinciJay RanganiNo ratings yet
- Pe 12 - SLHT 4 - January 25 To 29Document4 pagesPe 12 - SLHT 4 - January 25 To 29JESSA SUMAYANGNo ratings yet
- Qualifying Examination For Recruitment of Customer Service Assistants To People's Bank - 2021Document5 pagesQualifying Examination For Recruitment of Customer Service Assistants To People's Bank - 2021Hashan kosalaNo ratings yet
- NagarjunaDocument4 pagesNagarjunaCLG100% (1)
- The Suitable Racking System For Any Demand: ProductsDocument18 pagesThe Suitable Racking System For Any Demand: ProductsSheel JhaNo ratings yet
- Enabling SSL For Enterprise ApplicationsDocument22 pagesEnabling SSL For Enterprise ApplicationsSaket ShrivastavNo ratings yet
- SALT TriageDocument2 pagesSALT TriageThe DoctorNo ratings yet