You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5819)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (845)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Organ SystemDocument7 pagesOrgan SystemMaria MarmitaNo ratings yet
- NURSING-CARE-PLAN-Lung-Cancerxxx 1Document3 pagesNURSING-CARE-PLAN-Lung-Cancerxxx 1Caroline Cha100% (1)
- RespirationDocument3 pagesRespirationDr-Atin Kumar SrivastavaNo ratings yet
- Autopeep Paul Pepe Jhon MariniDocument5 pagesAutopeep Paul Pepe Jhon MariniRenatoNo ratings yet
- Re: Name: Mykid: RN: Diagnosis: 1) Severe Exacerbation of Bronchial Asthma Secondary To Pneumonia/ 2) Uncontrolled Brochial AsthmaDocument1 pageRe: Name: Mykid: RN: Diagnosis: 1) Severe Exacerbation of Bronchial Asthma Secondary To Pneumonia/ 2) Uncontrolled Brochial AsthmaAimanRiddleNo ratings yet
- Repaso 1 Natural ScienceDocument8 pagesRepaso 1 Natural ScienceElenaNo ratings yet
- Anak 10Document10 pagesAnak 10Bella FebriantiNo ratings yet
- Drugs Acting On Respiratory SystemDocument3 pagesDrugs Acting On Respiratory SystemAlyssa Audrey CaoagasNo ratings yet
- 10 - Unit 2+3Document16 pages10 - Unit 2+3Quynh TrangNo ratings yet
- Sistem RespiratoriDocument12 pagesSistem RespiratoriEmMa DHieyahNo ratings yet
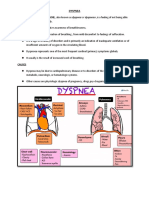
- Dyspnea: CausesDocument7 pagesDyspnea: CausesGetom NgukirNo ratings yet
- DT 103 New Topic 5Document22 pagesDT 103 New Topic 5CHRISTIAN SALABASNo ratings yet
- Group 1 (Science-9)Document3 pagesGroup 1 (Science-9)Joslyn Ditona DialNo ratings yet
- Pulmonary Aspergillosis: SciencedirectDocument8 pagesPulmonary Aspergillosis: SciencedirectEdgard Eduardo Azañero EstradaNo ratings yet
- Basic Interpretation of CXRDocument84 pagesBasic Interpretation of CXRHaluk AlibazogluNo ratings yet
- Parfitt:) : TryacheaDocument15 pagesParfitt:) : TryacheaJaisri MNo ratings yet
- SIC (Carpio, Kurt Andrew)Document5 pagesSIC (Carpio, Kurt Andrew)Kurt Andrew CarpioNo ratings yet
- 11th Bio-Zoology Important Five Mark QuestionsDocument3 pages11th Bio-Zoology Important Five Mark QuestionsSABHARISHKUMAR KNo ratings yet
- Parameters of Interest: - PH - pCO2 - Po2 - Hco3 Normal ValuesDocument25 pagesParameters of Interest: - PH - pCO2 - Po2 - Hco3 Normal ValuesPrincess Dumpit100% (1)
- Immediate Physiological Changes in New BornDocument7 pagesImmediate Physiological Changes in New BornLahunWanniangNo ratings yet
- Emphysema - PhysiopediaDocument1 pageEmphysema - PhysiopediaШеікх АбрарNo ratings yet
- The Women-S Fitness Book PDFDocument338 pagesThe Women-S Fitness Book PDFKaren Jennifer Beltrán Taipe95% (21)
- Deadly DozenDocument22 pagesDeadly DozenAbid Madriddista100% (1)
- History and Physical Examination in Pediatrics (1) - 1Document44 pagesHistory and Physical Examination in Pediatrics (1) - 1okwadha simion100% (1)
- Thermal Effects of WaterDocument8 pagesThermal Effects of WaterOwooluwa AdegboyegaNo ratings yet
- Chest TraumaDocument23 pagesChest TraumaMutaz DredeiNo ratings yet
- II. Upper Respiratory Tract DisordersDocument98 pagesII. Upper Respiratory Tract Disordersarielleortuoste100% (1)
- Ent ModuleDocument14 pagesEnt ModuleVishnu KrshNo ratings yet
- SCI-9 Q1 Mod1 Respiartoryandcirculatory V3b PDFDocument16 pagesSCI-9 Q1 Mod1 Respiartoryandcirculatory V3b PDFJerielyn Mae GarvidaNo ratings yet
- Chest and LungsDocument49 pagesChest and LungsChala KeneNo ratings yet