You might also like
- Reflection 1Document3 pagesReflection 1api-479716004No ratings yet
- Reflection 1 RofDocument2 pagesReflection 1 Rofapi-479716004No ratings yet
- Reflection 2Document2 pagesReflection 2api-479716004No ratings yet
- Reflection 2 X-Ray Report WrittingDocument2 pagesReflection 2 X-Ray Report Writtingapi-479716004No ratings yet
- Reflection 1Document2 pagesReflection 1api-479716004No ratings yet
- Rubric Reflective Portfolio 2020Document3 pagesRubric Reflective Portfolio 2020api-479716004No ratings yet
- Week 9 Portolio QuestionsDocument4 pagesWeek 9 Portolio Questionsapi-479716004No ratings yet
- ReflectionDocument2 pagesReflectionapi-479716004No ratings yet
- Reflection 2Document3 pagesReflection 2api-479716004No ratings yet
- Week 1 Portfolios QuestionsDocument7 pagesWeek 1 Portfolios Questionsapi-479716004No ratings yet
- Week 2 Portfolio QuestionsDocument12 pagesWeek 2 Portfolio Questionsapi-479716004No ratings yet
- Week 8 Portfolio QuestionsDocument2 pagesWeek 8 Portfolio Questionsapi-479716004No ratings yet
- Week 7 Portfolio QuestionsDocument8 pagesWeek 7 Portfolio Questionsapi-479716004No ratings yet
- Week 6 Portfolio QuestionsDocument6 pagesWeek 6 Portfolio Questionsapi-479716004No ratings yet
- Week 4 Portfolio QuestionsDocument5 pagesWeek 4 Portfolio Questionsapi-479716004No ratings yet
- Week 5 Portfolio QuestionsDocument4 pagesWeek 5 Portfolio Questionsapi-479716004No ratings yet
- Week 3 Portfolio QuestionsDocument5 pagesWeek 3 Portfolio Questionsapi-479716004No ratings yet
- Week 8 QuestionsDocument8 pagesWeek 8 Questionsapi-479716004No ratings yet
- Self-Directed LearningDocument3 pagesSelf-Directed Learningapi-479716004No ratings yet
- Week 4 Portfolio QuestionsDocument7 pagesWeek 4 Portfolio Questionsapi-479716004No ratings yet
- Study Guide Questions: 10.4: Exemplar For This Activity and Create A Management Plan For This PatientDocument5 pagesStudy Guide Questions: 10.4: Exemplar For This Activity and Create A Management Plan For This Patientapi-479716004No ratings yet
- Portfolio Exercises Week 9 & 10: Exercise 1 Differential Chart Location DDX Hip Pain DescriptionDocument6 pagesPortfolio Exercises Week 9 & 10: Exercise 1 Differential Chart Location DDX Hip Pain Descriptionapi-479716004No ratings yet
- Study Guide Questions Week 5Document3 pagesStudy Guide Questions Week 5api-479716004No ratings yet
- Exercise 1: CHIR12007 Clinical Assessment and Diagnosis Portfolio Exercises Week 7Document4 pagesExercise 1: CHIR12007 Clinical Assessment and Diagnosis Portfolio Exercises Week 7api-479716004No ratings yet
- Portfolio Rubric Reflective Portfolio 2020 Assessment 1 2Document2 pagesPortfolio Rubric Reflective Portfolio 2020 Assessment 1 2api-479716004No ratings yet
- Exercise 1Document13 pagesExercise 1api-479716004No ratings yet
- Reflection - Edward AtkinsDocument2 pagesReflection - Edward Atkinsapi-479716004No ratings yet
- Study Guide Questions: 9.4: Magee D, Edition (2014), Page 759-759 Provided As An ExemplarDocument9 pagesStudy Guide Questions: 9.4: Magee D, Edition (2014), Page 759-759 Provided As An Exemplarapi-479716004No ratings yet
- Week 7 QuestionsDocument5 pagesWeek 7 Questionsapi-479716004No ratings yet
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Caseih 956 1056 XL WSMDocument887 pagesCaseih 956 1056 XL WSMArek ZerebeckiNo ratings yet
- Sasot Vs PeopleDocument13 pagesSasot Vs PeopleUnsolicited CommentNo ratings yet
- 375x Full Capture XBOX Hits (UHQ) - @SpawnGoStockDocument44 pages375x Full Capture XBOX Hits (UHQ) - @SpawnGoStockbeyeb58041No ratings yet
- 350 Series Broce Broom Parts Catalog 88650 901871Document53 pages350 Series Broce Broom Parts Catalog 88650 901871Mariano David Pons Merino100% (4)
- 05 - DD Tools1Document27 pages05 - DD Tools1Slim.BNo ratings yet
- Units BTS Wiki FandomDocument1 pageUnits BTS Wiki Fandombrenda vergaraNo ratings yet
- Nyssra Sprint Biathlon ChampionshipDocument8 pagesNyssra Sprint Biathlon ChampionshipRyan ScottNo ratings yet
- HurlingDocument100 pagesHurlingMáirtín Ó hUallacháinNo ratings yet
- ScorpioDocument2 pagesScorpioAmrit PrasadNo ratings yet
- Concise parts list for Model 31200x11A chassis and hood repairDocument14 pagesConcise parts list for Model 31200x11A chassis and hood repairBruno DenolleNo ratings yet
- m8 Dirtywave GuideDocument1 pagem8 Dirtywave Guidekqwt2z8qcxNo ratings yet
- Majest TKD Study - PDF Version - V123Document104 pagesMajest TKD Study - PDF Version - V123SSNo ratings yet
- One Page Dungeon - Eric Diaz - The Wretched HiveDocument1 pageOne Page Dungeon - Eric Diaz - The Wretched HiveAndy HaydenNo ratings yet
- Beginners Guide CrossFitDocument5 pagesBeginners Guide CrossFitAdam 'Buddha' McGrath100% (2)
- Basic Fantasy Character Sheet 3 PDFDocument1 pageBasic Fantasy Character Sheet 3 PDFasiriNo ratings yet
- September 2018 Events, Days and PeopleDocument23 pagesSeptember 2018 Events, Days and PeopleMrutyunjaya BeheraNo ratings yet
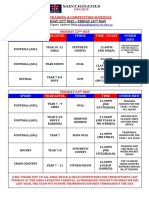
- Sport Year Level Venue Time / Staff Other Info: Sport Training & Competition ScheduleDocument5 pagesSport Year Level Venue Time / Staff Other Info: Sport Training & Competition ScheduleSusannah HewittNo ratings yet
- Aseball: Short Essay On Baseball: Category: On February 15, 2019 by TeamworkDocument2 pagesAseball: Short Essay On Baseball: Category: On February 15, 2019 by TeamworkshettyNo ratings yet
- Star Wars Edge of The Empire - Dice Roll ProbabilityDocument3 pagesStar Wars Edge of The Empire - Dice Roll ProbabilityStevenP125492% (13)
- Vehicle Coverage 10B0Ver Asian 1 (PERODUA)Document2 pagesVehicle Coverage 10B0Ver Asian 1 (PERODUA)daniel_ting_10% (1)
- Exploded View ExhaustDocument4 pagesExploded View Exhaustapi-3710514No ratings yet
- Celine Dion biography under 40 charsDocument1 pageCeline Dion biography under 40 charsDeny AhmadNo ratings yet
- Efectividad de Tratamiento en Pubalgia 1999Document5 pagesEfectividad de Tratamiento en Pubalgia 1999Maximiliano GaticaNo ratings yet
- HINO TRUCKS 2011-2013 VIN SETUP GUIDEDocument2 pagesHINO TRUCKS 2011-2013 VIN SETUP GUIDEABDUL SAMADNo ratings yet
- UntitledDocument86 pagesUntitledKartik SinglaNo ratings yet
- Tire Price ListDocument18 pagesTire Price ListreggieguapoNo ratings yet
- Paladin Press - 2010 - FallDocument100 pagesPaladin Press - 2010 - Fallsamestories100% (6)
- Black Eyed Peas LyricsDocument12 pagesBlack Eyed Peas LyricsDaniel CastleNo ratings yet
- 2010 NFL Tier - Tiering Fantasy Football Excel Spreadsheet Player RankingsDocument1 page2010 NFL Tier - Tiering Fantasy Football Excel Spreadsheet Player RankingsFantasy Football Information (fantasy-info.com)0% (1)
- 450-43le Aisin Seiki PDFDocument6 pages450-43le Aisin Seiki PDFBillyNo ratings yet