You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (842)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5807)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Guide To Pigging PDFDocument127 pagesGuide To Pigging PDFyrrossirda100% (1)
- II.a. Cell The Basic Unit of LifeDocument27 pagesII.a. Cell The Basic Unit of LifeDarwin NoolNo ratings yet
- Art Hemorragia PulmonarDocument12 pagesArt Hemorragia Pulmonarheidy acostaNo ratings yet
- Urinary Biomarkers For Acute Kidney Injury in DogsDocument13 pagesUrinary Biomarkers For Acute Kidney Injury in Dogsheidy acostaNo ratings yet
- Canine HyperlipidaemiaDocument11 pagesCanine Hyperlipidaemiaheidy acostaNo ratings yet
- Laboratory Evaluation of The LiverDocument1 pageLaboratory Evaluation of The Liverheidy acostaNo ratings yet
- 114140032Document1 page114140032Johnmar AquinoNo ratings yet
- Earth Sci 2 SG Unit 2 PDFDocument28 pagesEarth Sci 2 SG Unit 2 PDFbaileyNo ratings yet
- Terms of Reference - WASH in School ConsultantDocument8 pagesTerms of Reference - WASH in School ConsultantilyasabibhNo ratings yet
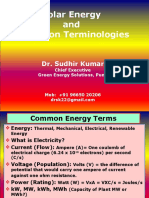
- Solar Energy and Radiation Terminologies: Dr. Sudhir KumarDocument24 pagesSolar Energy and Radiation Terminologies: Dr. Sudhir KumarAyman OsamaNo ratings yet
- Peer Tutoring Survey QuestionnaireDocument1 pagePeer Tutoring Survey QuestionnairekcapuzNo ratings yet
- Possibilities and ProbabilitiesDocument50 pagesPossibilities and ProbabilitiesChuckry Daligdig Maunes50% (2)
- SDP - 10 - Sustainable Agriculture in IndiaDocument60 pagesSDP - 10 - Sustainable Agriculture in IndiavjvarNo ratings yet
- ThesisDocument19 pagesThesisrichie sNo ratings yet
- E 945 - 96 Determination of Zinc in Zinc Ores and Concentrates byDocument4 pagesE 945 - 96 Determination of Zinc in Zinc Ores and Concentrates byJOSE ABADNo ratings yet
- Why Is Strategic Planning Important To An OrganizationDocument3 pagesWhy Is Strategic Planning Important To An OrganizationAtia Khalid100% (1)
- Radiamatic Detectors and Accessories Specification: FunctionDocument8 pagesRadiamatic Detectors and Accessories Specification: FunctionKatty MenaNo ratings yet
- Biuret Test For ProteinDocument1 pageBiuret Test For ProteinKal BuenaflorNo ratings yet
- IFAT Facts and Figures at A GlanceDocument6 pagesIFAT Facts and Figures at A GlanceArindam_SardarNo ratings yet
- DS LAB-3 Rahul Singh (191B317)Document7 pagesDS LAB-3 Rahul Singh (191B317)Rahul Singh100% (1)
- Wawancara Bahasa InggrisDocument20 pagesWawancara Bahasa InggrisYana Chaeru Taufik IsmailNo ratings yet
- Gabungan SemuaDocument38 pagesGabungan SemuaSawawa EgatyaNo ratings yet
- Administrative ManagementDocument10 pagesAdministrative Managementpriyveer chauhanNo ratings yet
- 44 Hemmings 2020-Owners Corporation Meeting SGM - 7064187-7064561-81S-200714 PDFDocument51 pages44 Hemmings 2020-Owners Corporation Meeting SGM - 7064187-7064561-81S-200714 PDFRayner MihailovNo ratings yet
- Mr. Chips Chapterwise QuestionsDocument16 pagesMr. Chips Chapterwise QuestionsMuhammad AtifNo ratings yet
- October NewsletterDocument1 pageOctober NewsletterJORDAN SANTOSNo ratings yet
- Senior Secondary Mathematics Syllabus - Grades 10-12 (Zambia)Document27 pagesSenior Secondary Mathematics Syllabus - Grades 10-12 (Zambia)STEVEN MDINGANo ratings yet
- Udoh Anthony JosephDocument4 pagesUdoh Anthony JosephDAVIDNo ratings yet
- K & B Industries: Welding Procedure Specification (WpsDocument4 pagesK & B Industries: Welding Procedure Specification (WpsRaja HoneNo ratings yet
- Brand Management: Role of Brand ElementsDocument22 pagesBrand Management: Role of Brand ElementsChibi RajaNo ratings yet
- MSC In: Machine Learning, Systems and ControlDocument2 pagesMSC In: Machine Learning, Systems and ControlMirza HassanNo ratings yet
- Arxiv 2Document10 pagesArxiv 2LUIS JESUS APAZA RODRIGUEZNo ratings yet
- Science 100: Science, Technology and Society: Lesson 2: Nature of TechnologyDocument9 pagesScience 100: Science, Technology and Society: Lesson 2: Nature of Technology이시연No ratings yet
- Hans Rosling Population Growth Video ActivityDocument2 pagesHans Rosling Population Growth Video Activityapi-655303552No ratings yet