You might also like
- Anatomy of The Shoulder Girdle and Scapulohumeral RhythmDocument30 pagesAnatomy of The Shoulder Girdle and Scapulohumeral RhythmthwisemanNo ratings yet
- PWB 2003Document19 pagesPWB 2003UnnatiNo ratings yet
- Bubble Inclinometer Measurement Chart PDFDocument2 pagesBubble Inclinometer Measurement Chart PDFsyedqutub16No ratings yet
- OMT Range of MotionDocument1 pageOMT Range of MotionMedShare100% (2)
- Chapter 48, Factors Influencing GaitDocument26 pagesChapter 48, Factors Influencing GaitShruti100% (14)
- Cardiorespiratory Case Presentation Sem 8Document29 pagesCardiorespiratory Case Presentation Sem 8Mika Araxia100% (1)
- Mulligan Therapy: What Is It and How Does It WorkDocument33 pagesMulligan Therapy: What Is It and How Does It WorkAgus SantosoNo ratings yet
- 5.6 Muscle Energy Techniques For The Pelvis 167-171Document5 pages5.6 Muscle Energy Techniques For The Pelvis 167-171maricartiNo ratings yet
- Orthopedic Physiotherapy Assignment: 1. Patient HistoryDocument4 pagesOrthopedic Physiotherapy Assignment: 1. Patient HistoryarushiNo ratings yet
- Spinal TractionDocument37 pagesSpinal TractionDibyendunarayan BidNo ratings yet
- Role of Physiotherapy in Antenatal and Post-Natal Care: Dr. Venus Pagare (PT)Document96 pagesRole of Physiotherapy in Antenatal and Post-Natal Care: Dr. Venus Pagare (PT)Haneen Jehad Um MalekNo ratings yet
- Physiotherapy Guidelines For Manual HyperinflationDocument5 pagesPhysiotherapy Guidelines For Manual HyperinflationAhmed Abd Elrauf100% (2)
- Elbow ComplexDocument11 pagesElbow ComplexAnita GajariNo ratings yet
- Chapter 47, Posture & GaitDocument18 pagesChapter 47, Posture & GaitShruti100% (11)
- Role of Physiotherapy in Antenatal and Post-Natal Care: Dr. Venus Pagare (PT)Document74 pagesRole of Physiotherapy in Antenatal and Post-Natal Care: Dr. Venus Pagare (PT)Haneen Jehad Um Malek100% (1)
- Antenatal Physiotherapy Care GuideDocument77 pagesAntenatal Physiotherapy Care Guides_saikalyanNo ratings yet
- Basics of Soft - Tissue ExaminationDocument32 pagesBasics of Soft - Tissue ExaminationGurudutt PaiNo ratings yet
- The Spencer TechniqueDocument11 pagesThe Spencer TechniqueDavidAgelliNo ratings yet
- Baseline Bubble Inclinometer User ManualDocument2 pagesBaseline Bubble Inclinometer User Manualphcproducts100% (2)
- Manual of Myokintics PDFDocument24 pagesManual of Myokintics PDFgiribalaji11100% (1)
- Special Tests of The Spine 1Document33 pagesSpecial Tests of The Spine 1Charles Jefferson Yamogan JiongcoNo ratings yet
- Icf C.P. AssessmentDocument5 pagesIcf C.P. AssessmentAnonymous cCy8GpNo ratings yet
- Range of MotionDocument17 pagesRange of MotionJim Cariaga100% (2)
- Clinical Guidelines For The Physiotherapy Management of Females Aged 16-65 With Stress Urinary IncontinenceDocument72 pagesClinical Guidelines For The Physiotherapy Management of Females Aged 16-65 With Stress Urinary IncontinenceAndré RodriguesNo ratings yet
- Kaltenbornmanualmobilizationsrs 150329041247 Conversion Gate01Document35 pagesKaltenbornmanualmobilizationsrs 150329041247 Conversion Gate01차성기No ratings yet
- Obstretics AssessmentDocument6 pagesObstretics AssessmentToli kkakrNo ratings yet
- Range of Motion Exercises &Document47 pagesRange of Motion Exercises &Nikita Sharma100% (1)
- Biomechanics of Cervical SpineDocument25 pagesBiomechanics of Cervical SpineNithya NithyaNo ratings yet
- Limb Length DiscrepancyDocument8 pagesLimb Length DiscrepancyManish Prasad100% (1)
- The Efficacy of Brotzman Physiotherapy Protocol On Pain and Knee Range of Motion in Post Surgical Total Knee Arthroplasty Subjects With ObesityDocument6 pagesThe Efficacy of Brotzman Physiotherapy Protocol On Pain and Knee Range of Motion in Post Surgical Total Knee Arthroplasty Subjects With ObesityInternational Journal of Physiotherapy and ResearchNo ratings yet
- Gait AnalysisDocument22 pagesGait AnalysisKumar RanjanNo ratings yet
- PROLOG: Obstetrics, Ninth Edition (Assessment & Critique)From EverandPROLOG: Obstetrics, Ninth Edition (Assessment & Critique)No ratings yet
- Bicipital TendinitisDocument19 pagesBicipital TendinitisRonak PatelNo ratings yet
- Range of Motion StandardsDocument2 pagesRange of Motion StandardsJulesNo ratings yet
- AnthropometricDocument60 pagesAnthropometricTrimayunika Julia100% (1)
- Anatomy and Physiology Terms: Brief Definitions, Roots & Morphology; An Abecedary; Vol 2-Planes & DirectionsFrom EverandAnatomy and Physiology Terms: Brief Definitions, Roots & Morphology; An Abecedary; Vol 2-Planes & DirectionsNo ratings yet
- MC Ken Ize Method A RomanoDocument12 pagesMC Ken Ize Method A RomanoDibyendunarayan Bid100% (1)
- Geriatric Rehabilitation: Prepared By: Floriza P. de Leon, PTRPDocument36 pagesGeriatric Rehabilitation: Prepared By: Floriza P. de Leon, PTRPFloriza de LeonNo ratings yet
- Lumbar Strain: Dr. Lipy Bhat PT Faculty, Physiotherapy SrhuDocument38 pagesLumbar Strain: Dr. Lipy Bhat PT Faculty, Physiotherapy SrhuKapil LakhwaraNo ratings yet
- Physiotherapy For PoliomyelitisDocument16 pagesPhysiotherapy For Poliomyelitisabdalsucs100% (1)
- Cervical RibDocument15 pagesCervical RibArko duttaNo ratings yet
- Cyriax IntroDocument14 pagesCyriax IntrodrrajmptnNo ratings yet
- The Convex Concave Rule and The Lever LawDocument4 pagesThe Convex Concave Rule and The Lever LawOwais KhanNo ratings yet
- Peripheral Nerve LesionDocument11 pagesPeripheral Nerve LesionBalaKrishnaNo ratings yet
- Week 2 - Elements of Physical Therapy ProcessDocument58 pagesWeek 2 - Elements of Physical Therapy ProcessMicah Victoria Banes100% (1)
- Physical Therapy Board Review 1e by Brad Fortinberry PT DPT Scs Michael Dunaway PT 1560534974Document5 pagesPhysical Therapy Board Review 1e by Brad Fortinberry PT DPT Scs Michael Dunaway PT 1560534974Ivan CasaresNo ratings yet
- MPT PDFDocument141 pagesMPT PDFSWATHI G ANo ratings yet
- Research Methodology: For All Physiotherapy and Allied Health Sciences StudentsDocument1 pageResearch Methodology: For All Physiotherapy and Allied Health Sciences StudentsProductivity 100No ratings yet
- Basic Neurophysiologic Principles For PNFDocument5 pagesBasic Neurophysiologic Principles For PNFdramitsainiNo ratings yet
- How Manipulation WorksDocument5 pagesHow Manipulation WorksRajeev TiwariNo ratings yet
- Proc RangeOfMotionDocument4 pagesProc RangeOfMotionSri KuspartianingsihNo ratings yet
- TKR ProtocolDocument8 pagesTKR ProtocolSandeep SoniNo ratings yet
- CTEVDocument27 pagesCTEVJevisco LauNo ratings yet
- Examination of The Hip Joint - RP's Ortho NotesDocument5 pagesExamination of The Hip Joint - RP's Ortho NotesSabari NathNo ratings yet
- Physiotherapy in Disaster MenegementDocument82 pagesPhysiotherapy in Disaster MenegementAtiKa YuLiantiNo ratings yet
- Physical Agent ModalitiesDocument13 pagesPhysical Agent ModalitiesLeonardo MustopoNo ratings yet
- Myossitis OssificansDocument16 pagesMyossitis OssificansMegha PataniNo ratings yet
- Case of Peripheral Vascular Disease: Dr. Shresth ManglikDocument18 pagesCase of Peripheral Vascular Disease: Dr. Shresth ManglikShresth ManglikNo ratings yet
- Peripheral NeuropathyDocument13 pagesPeripheral NeuropathyMohan KrishabiNo ratings yet
- Entrapment NeuropathyDocument10 pagesEntrapment NeuropathyMohan KrishabiNo ratings yet
- Alzheimer's DiseaseDocument4 pagesAlzheimer's DiseaseMohan KrishabiNo ratings yet
- Myotonic Dystrophy Type I (Steinert's Disease)Document3 pagesMyotonic Dystrophy Type I (Steinert's Disease)Mohan KrishabiNo ratings yet
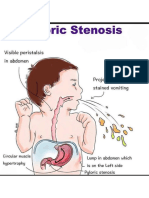
- Pyloric StenosisDocument1 pagePyloric StenosisMohan KrishabiNo ratings yet
- Pathophysiology of Pulmonary EmbolismDocument1 pagePathophysiology of Pulmonary EmbolismMohan Krishabi100% (1)
- Weber and Rinne TestDocument1 pageWeber and Rinne TestMohan KrishabiNo ratings yet
- Burns JournalDocument3 pagesBurns JournalMohan KrishabiNo ratings yet
- Divided Into Upper Part & Lower PartDocument20 pagesDivided Into Upper Part & Lower PartMohan KrishabiNo ratings yet