Professional Documents
Culture Documents
Smith Article
Uploaded by
ineedsheetzCopyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
Smith Article
Uploaded by
ineedsheetzCopyright:
Available Formats
Research Report
Physical Therapists Make Accurate and
Appropriate Discharge
Recommendations for Patients
Who Are Acutely Ill
Beth A. Smith, Christina J. Fields, Natalia Fernandez
B.A. Smith, PT, DPT, PhD, is Post-
doctoral Fellow, Balance Disorders
Background. Acute care physical therapists contribute to the complex process Laboratory, Departments of Neu-
of patient discharge planning. As physical therapists are experts at evaluating func- rology and Behavioral Neuro-
tional abilities and are able to incorporate various other factors relevant to discharge science, Oregon Health and
planning, it was expected that physical therapists’ recommendations of patient Science University, Portland, Ore-
discharge location would be both accurate and appropriate. gon. During the data collection
for this project, she was a PhD
candidate in the Developmental
Objective. This study determined how often the therapists’ recommendations Neuromotor Control Laboratory,
for patient discharge location and services were implemented, representing the School of Kinesiology, University
accuracy of the recommendations. The impact of unimplemented recommenda- of Michigan, and a per diem staff
tions on readmission rate was examined, reflecting the appropriateness of the member, Division of Physical
Therapy, University of Michigan
recommendations.
Hospital, Ann Arbor, Michigan. In-
stitutional mailing address: NSI,
Design. This retrospective study included the discharge recommendations of 40 OHSU West Campus, 505 NW
acute care physical therapists for 762 patients in a large academic medical center. The 185th Ave, Beaverton, OR 97006
frequency of mismatch between the physical therapist’s recommendation and the (USA). Address all correspondence
to Dr Smith at: smitbeth@
patient’s actual discharge location and services was calculated. The mismatch vari-
ohsu.edu.
able had 3 levels: match, mismatch with services lacking, or mismatch with different
services. Regression analysis was used to test whether mismatch status, patient age, C.J. Fields, PT, MPT, is Physical
Therapy Clinical Specialist, Car-
length of admission, or discharge location predicted patient readmittance.
diovascular Team, University of
Michigan Hospital.
Results. Overall, physical therapists’ discharge recommendations were imple-
mented 83% of the time. Patients were 2.9 times more likely to be readmitted when N. Fernandez, PT, Master of
Health Science (Physical Therapy),
the therapist’s discharge recommendation was not implemented and recommended is Staff Physical Therapist, Cardio-
follow-up services were lacking (mismatch with services lacking) compared with vascular Team, University of
patients with a match. Michigan Hospital.
[Smith BA, Fields CJ, Fernandez N.
Limitations. This study was limited to one facility. Limited information about the Physical therapists make accurate
patients was collected, and data on patient readmission to other facilities were not and appropriate discharge recom-
collected. mendations for patients who are
acutely ill. Phys Ther. 2010;
90:693–703.]
Conclusions. This study supports the role of physical therapists in discharge
planning in the acute care setting. Physical therapists demonstrated the ability to © 2010 American Physical Therapy
make accurate and appropriate discharge recommendations for patients who are Association
acutely ill.
Post a Rapid Response to
this article at:
ptjournal.apta.org
May 2010 Volume 90 Number 5 Physical Therapy f 693
Downloaded from https://academic.oup.com/ptj/article-abstract/90/5/693/2737769
by guest
on 11 January 2018
Acute Care Physical Therapists’ Discharge Recommendations
D
ischarge planning is the de- patients still often reported these discharge disposition,8 physical ther-
velopment of a discharge plan and other needs were unmet after apists and hospitals do not rely solely
for follow-up services for a pa- discharge. The study did not exam- on standardized tests in regard to dis-
tient prior to leaving the hospital, ine how the discharge planning pro- charge planning.9,10 Standardized
with the aim of containing costs and cess failed to accurately identify or screening forms are often used to
improving patient outcomes.1 Dis- meet the needs of the patients, but as identify patients at high risk of poor
charge planning is a complex pro- many health care professionals par- outcomes in order to initiate the for-
cess, and many health care disci- ticipate in the multifactorial process, mal multidisciplinary discharge plan-
plines may contribute to the plan, the final decision on discharge place- ning process, but they are not used
including formal discharge planning ment may not take into consider- to make the decision on discharge
coordinators, nurses, social workers, ation each professional’s recommen- location and services.3,5,6,11
physical therapists, occupational dation. Important information from
therapists, and physicians. Reviews one discipline may be overlooked or The need for comprehensive assess-
of discharge planning processes excluded from the final discharge ment of functional status is one fac-
showed that they consistently in- plan, leading to failure of the plan. tor in discharge planning that is di-
volve the assessment of many fac- rectly related to the practice of
tors, including cognitive, physical Poor discharge planning and the fail- physical therapy. One study quanti-
and social/financial status, environ- ure to provide necessary services fied change in functional status, re-
mental concerns, and access to for- may have an impact at several levels: porting that 35% of patients aged 70
mal and informal care.2,3 failure of the patient to reach opti- years and older showed a decline in
mal health and functional status, in- activities of daily living function be-
In an effort to assess these many fac- creased cost to the hospital and de- tween hospital admission and dis-
tors, formal discharge planning in creased resource availability to charge.12 Patients experiencing a de-
the United States often is practiced others due to increased length of cline in functional status while in the
as a collaborative, multidisciplinary stay and readmission, or possible ad- hospital may no longer be able to
effort led by a case manager, partic- verse events or conditions causing function adequately in the environ-
ularly for patients identified as hav- harm to the patient.7 In an effort to ment they lived in prior to admis-
ing an increased risk for poor out- better understand failure of the plan, sion, and are less likely to recover
comes.4,5 Although the shift toward several factors have been associated baseline function and health status.13
collaborative discharge planning has with poor postdischarge outcomes: There is an association between de-
improved patient outcomes, there aged 80 years and older; inadequate creased functional status and trans-
remains room for further improve- support system; multiple, active, fers to and from acute care set-
ment. A study by Mamon and col- chronic health problems; history of tings.14 There also is an association
leagues6 showed that multidisci- depression; moderate to severe func- between decreased functional status
plinary discharge planning efforts tional impairment; multiple hospital- and complicated posthospital care
led by formal case managers ap- izations during the prior 6 months; transitions.15
peared to be significantly more effec- hospitalization within the past 30
tive in arranging home nursing care days; fair or poor self-rating of The studies described above show
and rehabilitation services than infor- health; or history of nonadherence that level of functional ability is re-
mal discharge planning; however, to the therapeutic regimen.7 lated to discharge location; however,
other studies demonstrate that the
It is clear from the large number relationship, consistent with the
Available With and broad nature of factors associ- theme of discharge planning, is com-
This Article at ated with poor discharge outcomes plex. Although patients returning
ptjournal.apta.org that discharge planning is a com- home had a higher level of function
plex process requiring the assess- than those who were discharged
• Discussion Podcast: Participants ment and assimilation of multiple elsewhere, some patients who were
to be determined. factors. Additional evidence of dis- significantly impaired returned
• The Bottom Line Podcast charge planning as a complex pro- home with family support. Patients
• Audio Abstracts Podcast cess is the lack of use of standardized who had family support but were
quantitative measures to determine discharged to facilities were the
This article was published ahead of
print on March 18, 2010, at
discharge recommendations. De- most impaired.8 Additionally, re-
ptjournal.apta.org. spite the validation of measures such searchers studying the effect of func-
as the Berg Balance Scale to predict tional level on length of hospital ad-
694 f Physical Therapy Volume 90 Number 5 May 2010
Downloaded from https://academic.oup.com/ptj/article-abstract/90/5/693/2737769
by guest
on 11 January 2018
Acute Care Physical Therapists’ Discharge Recommendations
mission found that patients with a ate follow-up or referral.”19(p46) Fur- disability, patients’ wants and needs,
higher level of function demon- thermore, physical therapists are patients’ ability to participate in
strated a shorter length of stay than health care professionals who diag- care, and patients’ life context. The
average, but patients with a low level nose and treat individuals of all ages therapists gathered and integrated
of function who were discharged to who have medical problems or other information from multiple con-
a supportive environment also had a health-related conditions that limit structs before making their dis-
shorter-than-average length of stay.16 their ability to move and perform charge recommendation, showing
These findings highlight the com- functional activities in their daily consideration of what the patients
plex relationship between functional lives,19 and the assessment of func- required and what was available in
ability and discharge needs and fur- tional abilities is a particularly impor- their environment.9
ther support physical therapist eval- tant and complex aspect in deter-
uation of functional abilities, assis- mining discharge needs. Building upon previous descriptions
tance required for safety, and of the complexities of the decision-
recommendations for discharge loca- Having established that physical making process and the idea that
tion based on what the patient re- therapists are well qualified to par- physical therapists are uniquely
quires and what is available to them. ticipate in the complex discharge suited to contribute useful insight
planning process, how do they come through their evaluation and assess-
Physical therapists in the acute care to a decision on a discharge recom- ment skills, we wanted to validate
setting play an important role in the mendation? According to a qualita- the participation of acute care phys-
multidisciplinary discharge planning tive study by Jette et al,9 physical ical therapists in the discharge plan-
process. “Discharge to the appropri- therapists appeared to use a patient’s ning process. Because we hypothe-
ate level of care” often is a goal in level of functioning and disability as sized that therapists are able to
acute care physical therapy,17 and the core dimension in their initial successfully incorporate all of the
therapists routinely make recom- decision-making process. In general, various factors involved in the dis-
mendations regarding discharge they were guided by 4 constructs charge planning process and that
placement and any continuing ther- when making a discharge recom- there is value placed on the thera-
apy services for patients. Due to mendation: patients’ functioning and pist’s recommendation by the final
short average lengths of admission in
acute care, patients often need con-
tinued physical therapy services af- The Bottom Line
ter leaving acute care, and therapists
may recommend that continued ser-
vices take place in the home, a What do we already know about this topic?
skilled nursing facility (SNF), a reha- Acute care discharge planning is a complex process that involves clini-
bilitation center, or an outpatient
cians from varied disciplines and the assessment of many factors. Physical
setting.18
therapists often are involved in discharge planning and make recommen-
Although creating a discharge plan is dations for follow-up services, but the accuracy and appropriateness of
a multidisciplinary process, physical their recommendations have not been studied.
therapists practicing in acute care What new information does this study offer?
are in a unique position to assess the
discharge needs of a patient. This is This study indicates that physical therapists are able to integrate multiple
well described within the scope of patient factors to make accurate and appropriate discharge recommen-
practice in the Guide to Physical dations. When the physical therapist’s recommendation was not imple-
Therapist Practice: “The plan of care mented and follow-up services were lacking, patients were more likely to
identifies anticipated goals and ex- be readmitted to the hospital.
pected outcomes, taking into consid-
eration the expectations of the If you’re a patient, what might these findings mean
patient/client and appropriate oth- for you?
ers. . . . The plan of care includes the
anticipated discharge plans. In con- If you are in the hospital and have any concern that you will not be fully
sultation with appropriate individu- functional at discharge, you should seek a physical therapist’s recommen-
als, the physical therapist plans for dation for the most appropriate discharge destination.
discharge and provides for appropri-
May 2010 Volume 90 Number 5 Physical Therapy f 695
Downloaded from https://academic.oup.com/ptj/article-abstract/90/5/693/2737769
by guest
on 11 January 2018
Acute Care Physical Therapists’ Discharge Recommendations
discharge plan decision maker, we tion they read from the medical/sur- velop and implement discharge
anticipated that the therapist’s dis- gical team, unit nurses, and, when plans.19(p21)
charge recommendations for pa- consulted, occupational therapists
tients in the acute care setting would and social workers. In this basic pro- The physical therapist documents his
match the patient’s actual discharge cess, the coordinator may or may not or her evaluation in the computerized
location and services a majority of seek additional information from patient medical record. At the top of
the time. Furthermore, supporting other members of the health care every therapist evaluation and any sub-
the idea that therapists are appropri- team. If a consensus has been iden- sequent documentation, information
ate in their recommendations, we tified, the coordinator proceeds to is highlighted that is particularly rele-
expected an increased likelihood of arrange insurance benefits and nec- vant to discharge recommendations,
hospital readmissions when recom- essary services. If there is not a con- specifically therapist recommenda-
mendations were not implemented. sensus, the coordinator will elicit ad- tions for discharge location, the
ditional information from the other amount of assistance required for pa-
Method members of the health care team, tient safety, necessary assistive de-
The University of Michigan Hospital usually using the hospital alphanu- vices, and the need for ongoing phys-
is a 700-bed acute care teaching hos- meric paging and telephone systems. ical therapy and the appropriate
pital. Our facility is a level 1 trauma A lack of consensus can occur, for setting. This information is consis-
center offering and receiving heli- example, if the patient’s preferences tently provided by therapists, regard-
copter transfers for patients from change or if insurance benefits are less of whether or not patients are re-
Michigan and its surrounding states not available. ceiving formal discharge planning.
who are in critical and complex sit- Follow-up physical therapy treatments
uations; many of our patients are Physical therapist involvement in the are provided as appropriate through-
transferred from outside hospitals discharge planning process starts out the patient’s acute care stay, and
for ongoing care. when the medical/surgical team discharge recommendations are up-
sends an electronic consult to the dated and documented each time a
Discharge Planning Process Division of Physical Therapy through therapist works with the patient.
The discharge planning process in our online medical charting system.
our facility occurs in a fairly, but not The therapist does an initial evalua- Although all physical therapist rec-
completely, standardized manner. tion, with the exact procedures vary- ommendations are consistently doc-
The initial parts of the process are ing according to the ability of the umented in the medical record in a
standard; practice management co- patient to participate. The overall standard manner, the remaining dis-
ordinators use a screening form process is best described in the Guide charge process varies in how com-
based on the factors associated with to Physical Therapist Practice: munication is exchanged. Beyond
poor discharge outcomes to screen the basic discharge planning pro-
all admitted patients and identify [Physical therapists] engage in an ex- cess, some service areas of the hos-
those who are at increased risk for amination process that includes tak- pital follow additional procedures
ing the patient/client history, con- that increase in-person communica-
poor discharge outcomes. Patients
ducting a systems review, and
who are not identified as high risk by tion between health care providers.
performing tests and measures to
the screening process have dis- identify potential and existing prob-
Three of the services hold additional
charge planning done by their staff lems. To establish diagnoses, prog- daily or weekly “discharge rounds”
nurse, unless formal discharge plan- noses, and plans of care, physical interdisciplinary meetings, attended
ning is later requested. For patients therapists perform evaluations, syn- by the resident physician, practice
who are identified as high risk, for- thesizing the examination data and management coordinator, occupa-
mal discharge planning is initiated, determining whether the problems to tional therapist, physical therapist,
with practice management coordi- be addressed are within the scope of and social worker. In addition, some
nators taking the lead role in the physical therapist practice. Based on coordinators work with 1 or 2 spe-
discharge planning process. They read their judgments about diagnoses and cific services and make it a point to
prognoses and based on patient/cli- meet in person with the therapists,
the documentation on discharge
ent goals, physical therapists provide
recommendations from the physical whereas other coordinators float
interventions (the interactions and
therapist evaluation and any sub- procedures used in managing and in-
among services and do not do so.
sequent physical therapist docu- structing patients/clients), conduct
mentation and incorporate it into a reexaminations, modify interventions Data Collection
multidisciplinary discharge planning as necessary to achieve anticipated To conduct our retrospective study
process, including any documenta- goals and expected outcomes, and de- of the outcomes of the discharge
696 f Physical Therapy Volume 90 Number 5 May 2010
Downloaded from https://academic.oup.com/ptj/article-abstract/90/5/693/2737769
by guest
on 11 January 2018
Acute Care Physical Therapists’ Discharge Recommendations
planning process, we obtained Uni- were those we could not contact, therapist who documented the final
versity of Michigan Privacy Board who were no longer employed at the discharge recommendation.
approval for waiver of informed university, or who were temporary • Physical therapist discharge recom-
consent to access patient medical staff who did not evaluate patients mendation—the discharge location
records and institutional review during the 4 weeks we analyzed. and services that were determined by
board approval for the use of physi- One of the 3 primary investigators the therapist as necessary to promote
cal therapists as human participants. discussed the study with each thera- patient safety and any recovery, as
We accessed the medical records of pist before the informed consent based on the patient’s current level
all patients who received a physical form was signed. After consent, par- of function and available resources
therapist evaluation during our study ticipating therapists were asked to at discharge, coded as home without
period. We also collected data about provide the following background physical therapy, home with outpa-
career history from consenting ther- information: total months of practice tient therapy, home with home thera-
apists to further describe therapist as an acute care physical therapist, pist, subacute rehabilitation/SNF, acute
practice at our facility. total months and setting of other, rehabilitation, or extended care facility
nonacute care physical therapist ex- without therapy.
We created a secure database and perience, and total months of prac-
separated identifying information tice as an acute care physical thera- • Match—when the actual discharge lo-
about patients and therapists from pist at University of Michigan cation and services were the same as
de-identified, coded data collection Hospital. the discharge recommendation in the
forms. We selected one week (Sun- final therapist documentation.
day–Saturday) in each season of the We used hospital billing records to • Mismatch—when the actual discharge
preceding year. The weeks were in identify that 780 patients received a location or services were not the same
December 2007 and March, June, physical therapist evaluation during as the discharge recommendation in
and September 2008 and did not in- our specified 4 one-week periods, the final therapist documentation.
clude any holidays. and we included all of them in our
䡩 Mismatch with services lacking—
study. We specified the following
the patient did not receive
Two research assistants were operational definitions and collected
follow-up services when a home
trained, using case studies, to access the following data from patient med-
therapist was recommended.
medical records and find the rele- ical records:
䡩 Mismatch with different services
vant information and enter it into the
than recommended or extra servic-
database. Information was collected • Age of patient, in years.
es—the patient received home
primarily from physical therapist • Patient’s primary service at dis- physical therapy instead of recom-
evaluations and treatment notes, charge—service team of attending mended outpatient therapy or the
physician discharge notes, and prac- physician at the time of discharge, patient received home therapy
tice management coordinator evalu- listed by abbreviation code. when no follow-up therapy was rec-
ations and notes. Occasionally, data
were found in emergency depart- • Date of admission, in MM/DD/YYYY ommended.
ment documentation, physician ad- format.
• Reason for mismatch, categorized as:
mitting history and physical docu- • Date of discharge, in MM/DD/YYYY
ments, social work notes, nursing format. 䡩 Patient refusal of placement—the
notes, and outpatient or rehabilita- • Date of physical therapy evaluation, in therapist recommended placement
tion facility documentation from our MM/DD/YYYY format. or services, and the patient or his or
health system. Any questions related her legal representative declined,
to data collection were resolved by • Discharge location—the physical loca- 䡩 Insurance issues—the therapist rec-
consensus of the 3 primary investi- tion the patient was sent to at the end ommended placement or services,
gators (B.A.S., C.J.F, and N.F.). of the hospital admission, coded as and the patient did not receive them
home without physical therapy, home due to lack of insurance or insur-
Variables and Inclusion Criteria with outpatient therapy, home with ance denial of services,
We identified 51 physical therapists home therapist, subacute rehabilita- 䡩 Medical complexity of the patient
who were working in acute care dur- tion/SNF, acute rehabilitation, ex- precludes placement—the patient is
ing our selected weeks. Forty out of tended care facility without therapy, on a ventilator or receiving enteral/
the possible 51 therapists consented or expired. parental feedings, for example, or
to participate in our study. The 11 • Physical therapist at discharge—phys- 䡩 Other—any other reason.
therapists who were not included ical therapist identifier code of the
May 2010 Volume 90 Number 5 Physical Therapy f 697
Downloaded from https://academic.oup.com/ptj/article-abstract/90/5/693/2737769
by guest
on 11 January 2018
Acute Care Physical Therapists’ Discharge Recommendations
Table 1. 14 days, and ⱖ15 days. Mismatch
Patient Baseline Demographics status and discharge location were
Variable X SD Range
categorized as previously defined.
Patient age (y) 63 17 0–83
We used this analytic approach
Length of admission (d) 11 19 1–136
rather than the more common
Time from admission to physical therapist 4 4 0–37 method of linear regression for 2 rea-
evaluation (d)a
sons. First, our response variable (re-
Time from physical therapist evaluation to 7 22 0–122 admission) is a dichotomous out-
discharge (d)
come. Second, it allowed us to
a
Length of time to physical therapist evaluation was calculated from admission and did not take into control for the fact that each physi-
consideration when the consult was sent.
cal therapist made discharge recom-
mendations for multiple patients and
Table 2.
outcomes for a given therapist were
Mismatch Status by Discharge Location
not independent.21,22 Preliminary
Discharge Location Match Mismatch Total models tested for correlation of out-
Home without physical therapy 275 (83%) 58 (17%) 333 comes by physical therapy, but the
Home with outpatient physical therapy 13 (93%) 1 (7%) 14 observed correlation was not sig-
nificant. The reported results speci-
Home with home physical therapy 150 (76%) 47 (24%) 197
fied an independent correlation
Subacute rehabilitation/skilled nursing 129 (88%) 18 (12%) 147
facility
structure.
Acute rehabilitation 42 (100%) 0 (0%) 42
Results
Extended care facility, no physical therapy 10 (100%) 0 (0%) 10
Patient Demographics
Total 619 (83%) 124 (17%) 743 Of the 780 patients we identified as
having received physical therapist
evaluations in the specified 4 weeks,
we successfully collected data from
• Readmission—if the patient was admit- which variables were associated the medical records of 762 patients.
ted to our acute care facility within 30 with an increased risk of readmis- Eighteen patients were excluded be-
days of discharge, a time period con- sion. An alpha level of .05 was used cause their discharge location or the
sistent with similar studies.11,20 for all hypothesis testing. therapist recommendation could not
be determined. This situation oc-
Data Analysis We did logistic regression analysis curred when information was miss-
We used Microsoft Excel software using generalized estimating equa- ing from the medical record or cler-
(Microsoft Office 2007)* for database tions to control for correlation of the ical errors led to an inability to locate
formation and SPSS software (ver- outcomes by physical therapy and to the patient’s medical record. Of the
sions 16.0 and 17.0)† for statistical predict the probability that a patient 762 patients from whom we col-
analyses. We used descriptive statis- would be readmitted. The predictor lected data, 743 were eventually dis-
tics to summarize physical therapist variables we included in the model charged from acute care, and 19 ex-
and patient characteristics. We cal- were mismatch status, patient age, pired. Patients tended to be older
culated the frequency of occurrence length of admission, and discharge adults who were distributed across
of patient discharge locations, mis- location. These are all of the vari- medical (48%), surgical (27%), neu-
match, and readmission. Patients ables we collected that could have rology (7%) and trauma/orthopedic
who expired were included in demo- had an effect on readmission. Patient (18%) services. Although the ranges
graphic and descriptive data but ex- age and length of admission were were broad, the patients had an av-
cluded from statistical analyses of collapsed from continuous variables erage hospital admission of 11 days
mismatches or readmission. We used into categories to allow for more and were evaluated by a physical
a general linear modeling technique, meaningful analysis. Age was catego- therapist around day 4 of their admis-
explained below, to determine rized as ⱕ35 years, 36 to 55 years, 56 sion (Tab. 1). The discharge loca-
to 70 years, 71 to 84 years, and ⱖ85 tions of the patients from whom
* Microsoft Corp, One Microsoft Way, Red- years. Length of admission was cate- we collected data were as follows:
mond, WA 98052-6399.
†
SPSS Inc, 233 S Wacker Dr, Chicago, IL gorized as less than 2 days, 2 to 4 home without physical therapy
60606. days, 5 to 7 days, 8 to 10 days, 11 to (44%), home with home therapy
698 f Physical Therapy Volume 90 Number 5 May 2010
Downloaded from https://academic.oup.com/ptj/article-abstract/90/5/693/2737769
by guest
on 11 January 2018
Acute Care Physical Therapists’ Discharge Recommendations
Table 3.
Reason for Mismatch by Discharge Location
Discharge Location
Home With Home With Subacute
Home Without Outpatient Home Physical Rehabilitation/Skilled
Reason for Mismatch Physical Therapy Physical Therapy Therapy Nursing Facility Total
Patient refusal of placement 8 (57%) 0 (0%) 4 (29%) 2 (14%) 14
Insurance issues 2 (100%) 0 (0%) 0 (0%) 0 (0%) 2
Missing home physical therapy with 40 (100%) 0 (0%) 0 (0%) 0 (0%) 40
recommendation
Received home physical therapy without 0 (0%) 0 (0%) 32 (100%) 0 (0%) 32
recommendation
Other 8 (22%) 1 (3%) 11 (31%) 16 (44%) 36
Total 58 (47%) 1 (1%) 47 (38%) 18 (15%) 124
(26%), subacute rehabilitation/SNF unnecessary use of resources. Pa- Our overall readmission rate is con-
(19%), acute rehabilitation (5.5%), tient refusal of placement or services sistent with that of other studies.20,23
expired (2.5%), home with outpa- was the third largest category, and In our logistic regression analysis to
tient therapy (2%), and extended lack of insurance or insurance denial predict the probability that a patient
care facility without therapy (1%). of services caused very few would be readmitted, mismatch sta-
mismatches. tus, discharge location, and length of
Mismatches admission were significant predictor
There was a mismatch between Although most mismatches occurred variables. Patient age was not a sig-
physical therapist recommendation in patients who were ultimately dis- nificant predictor variable.
and patient discharge location in 124 charged home, mismatches in the
of 743 cases, or 17% of the time. The “other” category of reasons for mis- Table 5 shows the results of
breakdown by service groups was: match did include patients who follow-up hypothesis testing. Hold-
neurology/neurosurgery, 21%; medi- were subsequently discharged to a ing all other variables constant, a pa-
cine, 19%; surgery, 16%; and trauma/ subacute rehabilitation facility or tient was 2.9 times more likely to be
orthopedics, 7%. Mismatches are cat- SNF. These cases were scenarios readmitted when the therapist dis-
egorized by discharge location in where no beds were available at the charge recommendation was not im-
Table 2 and by reason for mismatch recommended level of care in the plemented and services were lacking
in Table 3. The majority of mis- patient’s preferred geographical area compared with patients with a match
matches occurred in patients who or where patients were denied ad- (mismatch with services lacking ver-
were discharged home. The most mittance to an acute rehabilitation sus match, odds ratio [OR]⫽2.89,
frequent reason for mismatch was facility despite the recommendation. 95% confidence interval [CI]⫽1.57–
patients who did not receive home 5.30). Patients whose therapist dis-
therapy when recommended. The Readmission charge recommendations were not
second largest group of mismatches As shown in Table 4, 139 patients implemented and who received dif-
were patients who received home (approximately 18% of our sample) ferent services or extra services were
therapy services that were not rec- were readmitted to our hospital not significantly more likely to be
ommended, a condition that reflects within 30 days of their discharge. readmitted than patients with a
Table 4.
Patient Readmission by Mismatch Status
Not Odds Ratio
Variable Readmitted Readmitted Total (95% Confidence Interval)
Match 103 (17%) 516 (83%) 619 (100%) 1
Mismatch: services lacking 22 (35%) 41 (65%) 63 (100%) 2.89 (1.57–5.30)a
Mismatch: different services 14 (23%) 47 (77%) 61 (100%) 1.42 (0.79–2.56)
a
Significantly different risk of readmission compared with match at P⬍.01.
May 2010 Volume 90 Number 5 Physical Therapy f 699
Downloaded from https://academic.oup.com/ptj/article-abstract/90/5/693/2737769
by guest
on 11 January 2018
Acute Care Physical Therapists’ Discharge Recommendations
Table 5. match (mismatch with different ser-
Odds of Readmission vices versus match, OR⫽1.42, 95%
95%
CI⫽0.79 –2.56).
Confidence
Predictor Variables Odds Ratio Interval Follow-up testing also revealed that
Mismatch patients discharged to an extended
Match Reference care facility were 6.9 times more
Mismatch: services lackinga 2.89 1.57–5.30
likely to be readmitted (OR⫽6.89,
95% CI⫽2.23–21.32) as compared to
Mismatch: different services 1.42 0.79–2.56
patients discharged home without
Discharge location
therapy. The results for patients dis-
Home without physical therapy Reference charged to an acute rehabilitation
Extended care facility, no physical therapya 6.89 2.23–21.32 setting approached significance in
Home with outpatient physical therapy 1.36 0.45–4.13 the direction of lower risk of read-
Home with home physical therapy 1.21 0.74–1.98
mission (OR⫽0.41, 95% CI⫽0.16 –
1.02) as compared to patients dis-
Subacute rehabilitation/skilled nursing facility 1.22 0.72–2.07
charged home without therapy. In
Acute rehabilitation 0.41 0.16–1.02
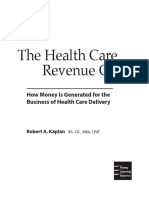
Figure 1 we show the different read-
Length of admission mission rates by discharge location.
0–1 d Reference
2–4 d 0.89 0.32–2.46 Physical Therapists
5–7 d 1.50 0.56–3.99
The 40 therapists included in the
sample had a mean of 110 months of
8–10 d 2.55 0.87–7.51
total experience as a practicing
11–14 d 0.91 0.26–3.15
physical therapist (range⫽3⫺354
ⱖ15d 0.85 0.33–2.20 months). As 23 of the physical ther-
a
Significant compared with reference at P⬍.05. apists had career experience beyond
the acute care setting, the range of
acute care experience was the same;
however, the mean was lower (mean
of 57.5 months of acute care
experience).
Discussion
Overall, patients were discharged in
accordance with the physical thera-
pist discharge recommendation 83%
of the time. When the discharge
recommendation was not imple-
mented and recommended follow-
up services were not received, pa-
tients were 2.9 times more likely to
be readmitted to our hospital within
30 days of discharge. Together, these
results indicate that therapists are able
to integrate multiple factors contrib-
Figure.
uting to the discharge needs of the
Rate of readmission by discharge location. Overall readmission rate was 18%, and
patients discharged to extended care facilities without physical therapy were signifi- patient to make accurate and appro-
cantly more likely to be readmitted to the hospital within 30 days. priate discharge recommendations.
An overall match rate of 83% be-
tween the therapist discharge rec-
ommendation and the patient’s ac-
tual discharge location and services
700 f Physical Therapy Volume 90 Number 5 May 2010
Downloaded from https://academic.oup.com/ptj/article-abstract/90/5/693/2737769
by guest
on 11 January 2018
Acute Care Physical Therapists’ Discharge Recommendations
indicates therapists are able to suc- though physical therapist recom- hospital. This challenge is difficult
cessfully incorporate all of the vari- mendations were not reported in for a number of reasons. Therapists
ous factors involved in the discharge their study, the findings indicate that often are consulted to work with the
planning process. This finding indi- there seem to be a number of pa- patients who are more medically and
cates that there is value placed on tients being discharged with unmet functionally compromised—patients
the therapist recommendation by needs. Perhaps practice manage- who are more likely to have negative
the final discharge plan decision ment coordinators need to screen outcomes than their less compro-
maker. It is possible, however, that patients for formal discharge plan- mised peers. In addition, therapists
in some cases the discharge recom- ning needs at discharge or after dis- often are advocating for additional
mendation happened to match the charge, not just at admission. Pa- services for patients, such as dis-
patient’s actual discharge location tients lacking necessary follow-up charge to a rehabilitation facility, and
without actually influencing the de- services are a problem that needs to the patient’s length of stay often in-
cision making of the nurse or prac- be addressed, as our findings show creases as he or she waits for ad-
tice management coordinator mak- that when physical therapist dis- mission to another facility. These
ing the final decision. It is difficult charge recommendations were not findings demonstrate that therapists
for us to explain the patients who implemented and recommended benefit both the patient and the hos-
did not receive home physical ther- follow-up services were not re- pital through their crucial role in the
apy when recommended or the pa- ceived, patients were 2.9 times more discharge planning process. When
tients who received home therapy likely to be readmitted to our therapist discharge recommenda-
services that were not recommend- hospital. tions were implemented and recom-
ed— by far the largest causes of a mended follow-up services were re-
mismatch. Either situation is a poor As the United States struggles to bal- ceived, the patient and the hospital
outcome, as it leads to a patient lack- ance efficiency and quality of health had an increased likelihood of posi-
ing in necessary services or unneces- care, the ability of physical therapists tive outcomes through a decreased
sary use of limited resources. These to provide accurate and appropriate risk of readmission.
cases ultimately reflect a lack of com- discharge recommendations becomes
munication between the physical even more important. Discharge plan- In addition to whether or not the
therapist and the practice manage- ning is increasingly becoming part of therapist recommendation was im-
ment coordinator, even though the an integrated package of health care, plemented, risk of readmission also
therapist recommendations were and even small reductions in readmis- was partially predicted by the pa-
clearly documented in the electronic sion rates could free up capacity for tient’s actual discharge location. Pa-
medical record. subsequent admissions in a health care tients discharged to an extended
system where there is a shortage of care facility without physical therapy
In the case of patients not receiving acute hospital beds.1 Decreases in re- were 6.9 times more likely to be re-
home physical therapy that was rec- admission rates, appropriate allocation admitted, whereas patients discharged
ommended, it is possible that the of resources, and avoidance of unnec- to acute rehabilitation approached a
therapist documentation was not essary services can help contain esca- significantly lower risk of 0.4 times
completed before the discharge plan lating health care costs. as likely to be readmitted. This find-
was in place and no verbal exchange ing probably reflects the nature of
about the recommendation took Another aspect of containing health illness and reason for admission of
place, or that the practice manage- care costs relates to the employment these patients, and possibly reflects
ment coordinator did not value the of physical therapists in the acute the quality of follow-up care they re-
information. Alternatively, it is possi- care setting. Since the initiation of ceive. Patients usually are discharged
ble that the patient was not receiving the Medicare prospective payment to an extended care facility without
formal discharge planning and, de- system and its use of diagnosis- a recommendation for continued
spite the therapist identifying the pa- related groups, payments to hospi- physical therapy because they are
tient’s need for services, no one fol- tals have been determined based on very ill with a poor prognosis for
lowed up to set up home therapy the patient’s diagnosis, regardless of functional gains, whereas patients
services. Interestingly, Mamon et al6 whether the patient receives ser- are discharged to an acute rehabilita-
reported a similar finding that 43% of vices such as physical therapy. Acute tion setting because it is believed
patients over the age of 60 years who care physical therapists have the that they will tolerate and benefit
were discharged home reported that challenge of justifying their salary from at least 3 hours per day of in-
they had an unmet need for physical cost to the hospital as outweighed by terdisciplinary rehabilitation. Acute
therapy or rehabilitation services. Al- the benefit to the patient and the rehabilitation patients also continue
May 2010 Volume 90 Number 5 Physical Therapy f 701
Downloaded from https://academic.oup.com/ptj/article-abstract/90/5/693/2737769
by guest
on 11 January 2018
Acute Care Physical Therapists’ Discharge Recommendations
to receive 24-hour nursing care and Limitations and Further lower than an overall readmission
the other benefits (and drawbacks) Questions rate, as there are almost certainly pa-
of a hospital setting, whereas pa- The major limitation of our study is tients discharged from our facility
tients discharged home do not. that it is unique to our facility and who were readmitted to facilities
Patients discharged to subacute reha- may have limited generalizability to closer to their home. Although our
bilitation or an SNF also receive 24- other acute care settings. The large readmission rate needs to be inter-
hour nursing care and daily rehabili- size of our hospital leads to many preted in context, the proportion of
tation, but, for a variety of reasons, staff members in each discipline, mismatches should be accurate. Pa-
have not been admitted to acute re- each of whom practices in an indi- tients who were part of a mismatch
habilitation or discharged home. Fur- vidual manner within the commu- should have been equally likely to be
ther speculation on the relationship nity of their discipline and within the readmitted to our hospital compared
between discharge location and risk larger hospital community. Resident with an outside hospital. By not as-
for readmission is beyond the scope physicians and physical therapists ro- sessing the reason for readmission,
and design of our study. tate between service areas of the we may have included patients who
hospital, interacting with different were readmitted for purely medical,
Of further interest, although we ac- members of the health care team and and not functional, reasons. Overall,
knowledge this information is spe- providing care to different types of readmission for any reason reflects a
cific to our facility, the frequency of patients within each area. As an aca- failure of the discharge plan, which
mismatch was not evenly distributed demic medical center and level 1 may have been avoided with proper
across the different primary attend- trauma center, the facility tends to supportive postdischarge care. A de-
ing services that discharged the pa- care for patients who are more se- cline in physical function is known
tients. Some services had a higher verely ill and complex, which cer- to contribute to emergency depart-
rate of mismatch than others. The tainly influences discharge locations ment visits in older adults.24
rate was highest for neurology/neu- and readmission rates.
rosurgery and lowest for trauma/or- Future research, with a larger sample
thopedics. One contributing factor In addition to the facility-specific as- size, could investigate how clinical
may be the nature of admissions; the pects of our study, other limitations experience influences the accuracy
orthopedic surgeons perform a high were that we collected limited infor- of discharge recommendations of
volume of planned surgeries com- mation on the patients who received acute care physical therapists. We
pared with the trauma/orthopedics physical therapist evaluations. We also think it would be interesting to
and neurology/neurosurgery ser- did not address readmission of pa- follow up with patients and gather
vices, which have a lesser volume of tients to hospitals other than our their perception of their recovery
patients and larger proportion of un- own and we did not assess the rea- and functional status in relation to
planned admissions. Planned admis- son for readmission. We did not their discharge services and location.
sions allow patients adequate time to collect information on reason for ad- We are particularly interested in the
confirm insurance benefits and con- mission, severity of illness, comor- patients who were functioning at a
sider discharge needs ahead of time. bidities, or functional level of the pa- level where both subacute rehabili-
tients, which is information that tiation/SNF and home with home
Different frequency of mismatch also would allow us to understand more physical therapy were viable op-
is likely related to the culture of each about patterns of recommendation tions. In addition, we were not able
service and differential value placed for discharge location or rates of re- to address how frequency of acute
on the physical therapist recommen- admission. In a cognizant effort to care physical therapist treatments in-
dation, as well as the slightly differ- respect patient privacy, we did not fluences discharge locations, which
ent processes by which communica- collect information on patient sex, may be of particular relevance in
tion is exchanged (eg, the presence race, or ethnicity, as we felt a discus- these “borderline” situations.
or absence of formal interdiscipli- sion of how these variables might
nary meetings). Within our 4 weeks relate to discharge location and read- Conclusions
of representative data, evaluations mission rates was beyond the scope Overall, our data strongly support
provided by each physical therapist of our report. the role of physical therapists in dis-
were distributed across the different charge planning in acute care. Phys-
services, avoiding undue influence In regard to tracking readmission ical therapists demonstrated the
of this phenomenon on our final re- only to our own hospital, our read- ability to make accurate discharge
sults but still reflecting the service- mission rate reflects only readmis- recommendations for patients with
specific rates of mismatch. sion to our hospital and is likely complex clinical presentations who
702 f Physical Therapy Volume 90 Number 5 May 2010
Downloaded from https://academic.oup.com/ptj/article-abstract/90/5/693/2737769
by guest
on 11 January 2018
Acute Care Physical Therapists’ Discharge Recommendations
are acutely ill; these patients were This article was received May 22, 2009, and 13 Boyd C, Landefeld CS, Counsell S, et al.
was accepted January 3, 2010. Recovery of activities of daily living in
discharged in accordance with the older adults after hospitalization for acute
therapist discharge recommendation DOI: 10.2522/ptj.20090164 medical illness. J Am Geriatr Soc. 2008;
56:2171–2179.
83% of the time. More important, we
14 Covinsky KE, Palmer RM, Fortinsky RH,
showed that the therapist discharge et al. Loss of independence in activities of
References
recommendations were appropriate, 1 Shepperd S, Parkes J, McClaran JJ, Phillips
daily living in older adults hospitalized
with medical illnesses: increased vulnera-
as patients were 2.9 times more C. Discharge planning from hospital to bility with age. J Am Geriatr Soc. 2003;51:
likely to be readmitted when the dis- home. Cochrane Database Syst Rev. 451– 458.
2003;3:CD000313.
charge recommendations were not 2 Jackson MF. Discharge planning: issues
15 Coleman EA, Min SJ, Chomiak A, Kramer
AM. Posthospital care transitions: pat-
implemented and recommended and challenges for gerontological nursing: terns, complications, and risk identifica-
follow-up services were lacking. a critique of the literature. J Adv Nurs. tion. Health Serv Res. 2004;39:
1994;19:492–502. 1449 –1465.
3 Haddock KS. Characteristics of effective 16 Ensberg MD, Paletta MJ, Galecki AT, et al.
discharge planning programs for the frail Identifying elderly patients for early dis-
All authors provided concept/idea/research elderly. J Gerontol Nurs. 1991;17:10 –14. charge after hospitalization for hip frac-
design, writing, data collection, and consul-
4 Hickey ML, Cook EF, Rossi LP, et al. Effect ture. J Gerontol. 1993;48:M187–M195.
tation (including review of manuscript be- of case managers with a general medical 17 Jette DU, Brown R, Collette N, et al. Phys-
fore submission). Dr Smith and Ms Fields patient population. J Eval Clin Pract. ical therapists’ management of patients in
provided data analysis. Dr Smith provided 2000;6:23–29. the acute care setting: an observational
project management. Ms Fields provided 5 Naylor M, Brooten D, Jones R, et al. Com- study. Phys Ther. 2009;89:1158 –1181.
participants. Dr Smith and Ms Fernandez prehensive discharge planning for the hos- 18 Curtis KA, Martin T. Perceptions of acute
provided clerical support. pitalized elderly: a randomized clinical tri- care physical therapy practice: issues for
al. Ann Intern Med. 1994;120:999 –1006. physical therapist preparation. Phys Ther.
The authors thank the physical therapy staff at 6 Mamon J, Steinwachs DM, Fahey M, et al. 1993;73:581–594; discussion 594 –598.
the University of Michigan Hospital for their Impact of hospital discharge planning on 19 Guide to Physical Therapist Practice. 2nd
participation and support, particularly Casan- meeting patient needs after returning ed. Phys Ther. 2001;81:9 –746.
home. Health Serv Res. 1992;27:155–175.
dra Redmon and Lauren Lobert for data col- 20 Einstadter D, Cebul RD, Franta PR. Effect
lection. They also thank Diane Jette, PT, DSc, 7 Bowles KH, Naylor MD, Foust JB. Patient of a nurse case manager on postdischarge
characteristics at hospital discharge and a follow-up. J Gen Intern Med. 1996;11:
for her comments on the initial idea. comparison of home care referral deci- 684 – 688.
sions. J Am Geriatr Soc. 2002;50:
A poster presentation of this research was 336 –342. 21 Pagano M, Gauvreau K. Principles of Bio-
given at the Combined Sections Meeting statistics. Florence, KY: Wadsworth Pub-
8 Wee JY, Wong H, Palepu A. Validation of lishing Co; 1993.
of the American Physical Therapy Association; the Berg Balance Scale as a predictor of
February 17–20, 2010; San Diego, California. length of stay and discharge destination in 22 Resnik L, Liu D, Hart DL, Mor V. Bench-
stroke rehabilitation. Arch Phys Med Re- marking physical therapy clinic perfor-
This publication was made possible with habil. 2003;84:731–735. mance: Statistical methods to enhance in-
support from the Oregon Clinical and Trans- ternal validity when using observational
9 Jette DU, Grover L, Keck CP. A qualitative data. Phys Ther. 2008;88:1078 –1087.
lational Research Institute; grant UL1 study of clinical decision making in recom-
RR024140 01 from the National Center for mending discharge placement from the 23 Bowles KH, Ratcliffe SJ, Holmes JH, et al.
acute care setting. Phys Ther. 2003; Post-acute referral decisions made by mul-
Research Resources, a component of the
83:224 –236. tidisciplinary experts compared to hospi-
National Institutes of Health (NIH); and the tal clinicians and the patients’ 12-week
NIH Roadmap for Medical Research. Dr 10 Potthoff S, Kane RL, Franco SJ. Improving outcomes. Med Care. 2008;46:158 –166.
hospital discharge planning for elderly pa-
Smith is supported by a National Institute of tients. Health Care Financ Rev. 1997;19: 24 Wilber ST, Blanda M, Gerson LW. Does
Aging Institutional Training Grant to Jeri 47–72. functional decline prompt emergency de-
Janowsky (principal investigator). During her partment visits and admission in older
11 Haddock KS. Collaborative discharge plan- patients? Acad Emerg Med. 2006;13:
PhD studies, she was supported by grant ning: nursing and social services. Clin 680 – 682.
H424C010067 from the US Office of Special Nurse Spec. 1994;8:248 –252.
Education and Rehabilitative Services to Dale 12 Gill TM, Williams CS, Tinetti ME. The com-
Ulrich (principal investigator). bined effects of baseline vulnerability and
acute hospital events on the development
of functional dependence among
community-living older persons. J Gerontol
A Biol Sci Med Sci. 1999;54:M377–M383.
May 2010 Volume 90 Number 5 Physical Therapy f 703
Downloaded from https://academic.oup.com/ptj/article-abstract/90/5/693/2737769
by guest
on 11 January 2018
You might also like
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- There's No Way This PDF Exists On Scribd Already 13423513245Document1 pageThere's No Way This PDF Exists On Scribd Already 13423513245ineedsheetzNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Dummy PDFDocument1 pageDummy PDFineedsheetzNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Theories of MotivationDocument3 pagesTheories of MotivationineedsheetzNo ratings yet
- Love Stage!! - Love Stage BGM PDFDocument1 pageLove Stage!! - Love Stage BGM PDFineedsheetzNo ratings yet
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Laputa - Castle in The Sky - Gakkou No UnkaiDocument2 pagesLaputa - Castle in The Sky - Gakkou No UnkaiRodrigo Ivan Henriquez AbalosNo ratings yet
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Luzideus Savant - Waltz of The Lazy Chair Room PDFDocument4 pagesLuzideus Savant - Waltz of The Lazy Chair Room PDFineedsheetzNo ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Fdagbgs PDFDocument1 pageFdagbgs PDFineedsheetzNo ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Rotator CuffDocument11 pagesRotator CuffineedsheetzNo ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Sword Art Online - Yuuki's Theme PDFDocument2 pagesSword Art Online - Yuuki's Theme PDFineedsheetzNo ratings yet
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Lumbar Fusion ProtocolDocument7 pagesLumbar Fusion ProtocolineedsheetzNo ratings yet
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- RTC Strengthening Article PDFDocument14 pagesRTC Strengthening Article PDFineedsheetzNo ratings yet
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Rancho Gait BookDocument36 pagesRancho Gait BookineedsheetzNo ratings yet
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Rancho Gait BookDocument36 pagesRancho Gait BookineedsheetzNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Home Workout PlanDocument13 pagesHome Workout Planineedsheetz83% (6)
- RTC Strengthening ArticleDocument14 pagesRTC Strengthening ArticleineedsheetzNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Rehabilitation Protocol: Total Knee Arthroplasty (TKA) : Department of Orthopaedic SurgeryDocument10 pagesRehabilitation Protocol: Total Knee Arthroplasty (TKA) : Department of Orthopaedic SurgeryineedsheetzNo ratings yet
- Jette Article 2003Document13 pagesJette Article 2003ineedsheetzNo ratings yet
- Wingate ReferencesDocument8 pagesWingate ReferencesineedsheetzNo ratings yet
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Preventing and Managing COVID-19 Across Long-Term Care ServicesDocument8 pagesPreventing and Managing COVID-19 Across Long-Term Care ServicesMark Anthony MadridanoNo ratings yet
- Department of Labor: MIRAS VICTORIA V SOUTH HILLS COUNTRY HOMES 2002INA00142 (SEP 15 2003) 123421 CADEC SDDocument8 pagesDepartment of Labor: MIRAS VICTORIA V SOUTH HILLS COUNTRY HOMES 2002INA00142 (SEP 15 2003) 123421 CADEC SDUSA_DepartmentOfLaborNo ratings yet
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Rebekah Naler: Experience SkillsDocument2 pagesRebekah Naler: Experience SkillsRebekah NalerNo ratings yet
- Home Technical Assistance and Consultation Manual - Effective 1-1-16 509880 7Document187 pagesHome Technical Assistance and Consultation Manual - Effective 1-1-16 509880 7WXYZ-TV Channel 7 DetroitNo ratings yet
- MICHIGAN ZONING ENABLING ACT - Michigan PA 110 of 2006Document23 pagesMICHIGAN ZONING ENABLING ACT - Michigan PA 110 of 2006Stephen BoyleNo ratings yet
- The AOTA Assembly of Student Delegates Newsletter.Document18 pagesThe AOTA Assembly of Student Delegates Newsletter.ASDAOTANo ratings yet
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- 1337109296binder2Document35 pages1337109296binder2CoolerAdsNo ratings yet
- Test Bank For Gerontological Nursing 3rd Edition, TabloskiDocument55 pagesTest Bank For Gerontological Nursing 3rd Edition, TabloskiILL10150% (2)
- Learning PlanDocument7 pagesLearning Planapi-283070240No ratings yet
- Commercialization of Health Care - Good or Bad - Group DiscussionDocument26 pagesCommercialization of Health Care - Good or Bad - Group Discussionmanthan321No ratings yet
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- National Policy On Older Persons, 1999Document14 pagesNational Policy On Older Persons, 1999Latest Laws TeamNo ratings yet
- Assignment 1Document4 pagesAssignment 1mp1757100% (1)
- Revenue CycleDocument240 pagesRevenue CyclePercentage International School100% (2)
- Resignation Leter SamplesDocument3 pagesResignation Leter SamplesjoyrojasNo ratings yet
- ARCHITECTURE AND DESIGN-Guidelines and H (Article) PDFDocument8 pagesARCHITECTURE AND DESIGN-Guidelines and H (Article) PDFNeelam SiddiquiNo ratings yet
- FGI PHAMA Whitepaper 042810 PDFDocument149 pagesFGI PHAMA Whitepaper 042810 PDFbejarhasanNo ratings yet
- Being Mortal: Medicine and What Matters in The EndDocument15 pagesBeing Mortal: Medicine and What Matters in The EndEsteban0% (19)
- House Hearing, 110TH Congress - Elder Justice Act, The Elder Abuse Victims Act of 2008, The School Safety Enhancements Act of 2007, and The A Child Is Missing Alert and Recovery Center ActDocument127 pagesHouse Hearing, 110TH Congress - Elder Justice Act, The Elder Abuse Victims Act of 2008, The School Safety Enhancements Act of 2007, and The A Child Is Missing Alert and Recovery Center ActScribd Government DocsNo ratings yet
- RESUMEDocument4 pagesRESUMEMark Noel MadlambayanNo ratings yet
- Horticulture Therapy: Cultivating Health and Harmony at The Riverview Nursing HomeDocument5 pagesHorticulture Therapy: Cultivating Health and Harmony at The Riverview Nursing HomeKritikou1547No ratings yet
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Nursewriting2 1531889490922Document4 pagesNursewriting2 1531889490922gyby_nairNo ratings yet
- TennCare English ApplicationDocument16 pagesTennCare English ApplicationJorge Machado TencioNo ratings yet
- Bajaj Capital 1Document32 pagesBajaj Capital 1Shahnawaz HussainNo ratings yet
- Cultural Immersion PaperDocument11 pagesCultural Immersion Paperapi-261985540No ratings yet
- Guidelines For The Design and Construction of Health Care FacilitiesDocument370 pagesGuidelines For The Design and Construction of Health Care FacilitiesJay MenaNo ratings yet
- FNW Locum Contract TemplateDocument5 pagesFNW Locum Contract Templateapi-279667195No ratings yet
- Building Capacity To Care and Capability To TreatDocument60 pagesBuilding Capacity To Care and Capability To TreatRuth WilsonNo ratings yet
- Sweden EldersDocument63 pagesSweden Eldersstockholm-arlandaNo ratings yet
- 2010 FGI Guidelines TOCDocument11 pages2010 FGI Guidelines TOCacastromNo ratings yet
- Welcome!: Seh Corporate Golf DayDocument8 pagesWelcome!: Seh Corporate Golf DaysandycastleNo ratings yet