You might also like
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Tetric LineDocument10 pagesTetric LineAndrea LawNo ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- G-Cem Capsule: Prior To Use, Carefully Read The Instructions For UseDocument1 pageG-Cem Capsule: Prior To Use, Carefully Read The Instructions For UseAndrea LawNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Clinical Significance of Accessory Foramina in AduDocument6 pagesClinical Significance of Accessory Foramina in AduAndrea LawNo ratings yet
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Empress Direct - Special - Mahn - en - 678773 - PRINT PDFDocument48 pagesEmpress Direct - Special - Mahn - en - 678773 - PRINT PDFKhalil SalahNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Selection of Articulator For General Dental PractiDocument6 pagesSelection of Articulator For General Dental PractiAayushi VaidyaNo ratings yet
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Dental WaxDocument14 pagesDental WaxAndrea LawNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
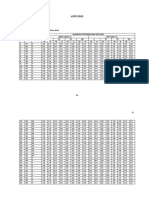
- Appendix: Appendix 1 Master Table Alveolar Bone Resorption DataDocument12 pagesAppendix: Appendix 1 Master Table Alveolar Bone Resorption DataAndrea LawNo ratings yet
- InTech-Bone Quality Assessment For Dental ImplantsDocument17 pagesInTech-Bone Quality Assessment For Dental ImplantsMohamed Abd El-Fattah GalalNo ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Uses of Dental Wax in Clinics and LaboratoriesDocument2 pagesUses of Dental Wax in Clinics and LaboratoriesAndrea LawNo ratings yet
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- 016-Malignant Tumours of The Oral CavityDocument11 pages016-Malignant Tumours of The Oral CavityAndrea LawNo ratings yet
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- 016 Andrea - Smile DesignDocument3 pages016 Andrea - Smile DesignAndrea LawNo ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Analytical Vs Descriptive ResearchDocument2 pagesAnalytical Vs Descriptive ResearchAndrea LawNo ratings yet
- 016-017 Diagnosis of Case 5Document3 pages016-017 Diagnosis of Case 5Andrea LawNo ratings yet
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Daftar PustakaDocument5 pagesDaftar PustakaAndrea LawNo ratings yet
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Bone Resorption Increases with Age and Differs between GendersDocument1 pageBone Resorption Increases with Age and Differs between GendersAndrea LawNo ratings yet
- 5 CementoenamelDocument8 pages5 CementoenamelAndrea LawNo ratings yet
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- PedoDocument12 pagesPedoAndrea LawNo ratings yet
- DSP 9 Case 5 Tooth FractureDocument39 pagesDSP 9 Case 5 Tooth FractureAndrea LawNo ratings yet
- Topic 8Document51 pagesTopic 8Andrea LawNo ratings yet
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- 016 Andrea - Smile DesignDocument3 pages016 Andrea - Smile DesignAndrea LawNo ratings yet
- AdenddumsDocument16 pagesAdenddumsAndrea LawNo ratings yet
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- Index of RefractionDocument3 pagesIndex of RefractionAndrea LawNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Topic 3 Dentoalveolar FractureDocument56 pagesTopic 3 Dentoalveolar FractureAndrea LawNo ratings yet
- Preprosthetic SurgeryDocument4 pagesPreprosthetic SurgeryDentist HereNo ratings yet
- Sex Steroid and The BoneDocument29 pagesSex Steroid and The BoneAndrea LawNo ratings yet
- 016 Andrea - Smile DesignDocument3 pages016 Andrea - Smile DesignAndrea LawNo ratings yet
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Example Adult Maxillary Anterior Occlusal Radiograph.: SourceDocument2 pagesExample Adult Maxillary Anterior Occlusal Radiograph.: SourceAndrea LawNo ratings yet
- 016 ImpactionDocument9 pages016 ImpactionAndrea LawNo ratings yet
- General Technique of Third Molar Removal, Bouloux G.F. 2007Document21 pagesGeneral Technique of Third Molar Removal, Bouloux G.F. 2007Felipe Ronceros100% (1)
- BJMP Dental Referral FormDocument2 pagesBJMP Dental Referral FormRoyce Christian EbitNo ratings yet
- Understanding Anterior Guidance and its Relationship to Arch FormDocument122 pagesUnderstanding Anterior Guidance and its Relationship to Arch Formmentacity100% (1)
- Dental FormDocument22 pagesDental FormJhon Niño BaguioNo ratings yet
- Mcguire 1991Document8 pagesMcguire 1991Angela RamirezNo ratings yet
- April 2017-1 MJDFDocument24 pagesApril 2017-1 MJDFsajna1980No ratings yet
- Radii Plus +: Your Choice of Accessories yDocument2 pagesRadii Plus +: Your Choice of Accessories yDimas NavarroNo ratings yet
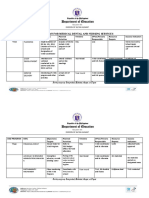
- Sample WINS Action PLanDocument3 pagesSample WINS Action PLanJEANYVIE ESPINOSANo ratings yet
- Sem2 NanoparticlesDocument35 pagesSem2 NanoparticlesgujjugullygirlNo ratings yet
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Running Head: Digital Custom Implant Impression: Version of Record Doi: 10.1111/jopr.13200Document16 pagesRunning Head: Digital Custom Implant Impression: Version of Record Doi: 10.1111/jopr.13200Roja AllampallyNo ratings yet
- Radiographic Evaluation of Periapical Healing After Obturation of Infected Root Canals in Vivo Katebzadeh Trope 2000Document7 pagesRadiographic Evaluation of Periapical Healing After Obturation of Infected Root Canals in Vivo Katebzadeh Trope 2000abcder1234No ratings yet
- Tongue Tie - Classification - Poster - 2014 Premier HealthDocument1 pageTongue Tie - Classification - Poster - 2014 Premier HealthKayla CelentanoNo ratings yet
- BOS Mini ScrewsDocument2 pagesBOS Mini ScrewsWajeeha YounisNo ratings yet
- ART - ATRAUMATIC RESTORATIVE TREATMENT ArchuDocument17 pagesART - ATRAUMATIC RESTORATIVE TREATMENT ArchuMuhammed ThanseehNo ratings yet
- Overdenture Case PresentationDocument76 pagesOverdenture Case PresentationAniket MoneNo ratings yet
- Flapless Dental Implant Surgery With Surgical GuideDocument3 pagesFlapless Dental Implant Surgery With Surgical GuideImplant Surgical GuidesNo ratings yet
- Dental Trauma: Crown Fractures: Mai.A.S.Dama BDS, Mfdsrcsi, High Specialty in Pediatric Dentistry, PLB (Pead), Job (Pead)Document76 pagesDental Trauma: Crown Fractures: Mai.A.S.Dama BDS, Mfdsrcsi, High Specialty in Pediatric Dentistry, PLB (Pead), Job (Pead)Ahmad RiyadNo ratings yet
- Feb 2017 Compilation Juge - DocxDocument24 pagesFeb 2017 Compilation Juge - DocxMohamed AitaNo ratings yet
- M-i-M For DME Matrix-In-A-Matrix Technique For Deep Margin ElevationDocument5 pagesM-i-M For DME Matrix-In-A-Matrix Technique For Deep Margin Elevationfernando vicente100% (1)
- Library Dissertation Topics in PeriodontologyDocument10 pagesLibrary Dissertation Topics in PeriodontologyBuyCustomPaperUK100% (1)
- April 29 8:30AM - Dental Residencies by Mark KodayDocument23 pagesApril 29 8:30AM - Dental Residencies by Mark Kodayjordyn1990No ratings yet
- Open BiteDocument14 pagesOpen Biteفاطمة فالح ضايف مزعلNo ratings yet
- Ferraris Et Al IJED PIAR ARG 2 20212Document24 pagesFerraris Et Al IJED PIAR ARG 2 20212khaled emadNo ratings yet
- Force Systems From An Ideal Arch Burstone 1974Document1 pageForce Systems From An Ideal Arch Burstone 1974Verônica Polo PerezNo ratings yet
- Peri-Implantitis: Srijana Heka Bds Iv Year Roll No: 17Document60 pagesPeri-Implantitis: Srijana Heka Bds Iv Year Roll No: 17cz22naNo ratings yet
- 2 - англ 2012Document92 pages2 - англ 2012AlexcheckNo ratings yet
- Zirconio ImpresoDocument8 pagesZirconio ImpresoLinda Garcia PNo ratings yet
- Three-Dimensional Assessment of Transverse Skeletal Changes After Surgically Assisted Rapid Maxillary Expansion and Orthodontic Treatment - A Prospective Computerized Tomography StudyDocument9 pagesThree-Dimensional Assessment of Transverse Skeletal Changes After Surgically Assisted Rapid Maxillary Expansion and Orthodontic Treatment - A Prospective Computerized Tomography StudySoe San KyawNo ratings yet
- Medicine: Implants For Orthodontic AnchorageDocument8 pagesMedicine: Implants For Orthodontic AnchorageMilena RamirezNo ratings yet
- Advlocalanaesthesia IsenDocument153 pagesAdvlocalanaesthesia IsenResa YudhistiNo ratings yet
- Apex Loctor 2021Document7 pagesApex Loctor 2021nandani kumariNo ratings yet
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionFrom EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionRating: 4 out of 5 stars4/5 (402)
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (15)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeNo ratings yet
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsFrom EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsRating: 5 out of 5 stars5/5 (1)
- The Obesity Code: Unlocking the Secrets of Weight LossFrom EverandThe Obesity Code: Unlocking the Secrets of Weight LossRating: 5 out of 5 stars5/5 (4)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsFrom EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNo ratings yet