Professional Documents
Culture Documents
TNBC PMRT 1
Uploaded by
Med MedOriginal Description:
Copyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
TNBC PMRT 1
Uploaded by
Med MedCopyright:
Available Formats
Review
Radiation therapy in the locoregional treatment of
triple-negative breast cancer
Meena S Moran
This Review assesses the relevant data and controversies regarding the use of radiotherapy for, and locoregional Lancet Oncol 2015; 16: e113–22
management of, women with triple-negative breast cancer (TNBC). In view of the strong association between BRCA1 Yale University School of
and TNBC, knowledge of baseline mutation status can be useful to guide locoregional treatment decisions. TNBC is Medicine, Department of
Therapeutic Radiology, New
not a contraindication for breast conservation therapy because data suggest increased locoregional recurrence risks
Haven, CT, USA (M S Moran MD)
(relative to luminal subtypes) with breast conservation therapy or mastectomy. Although a boost to the tumour bed
Correspondence to:
should routinely be considered after whole breast radiation therapy, TNBC should not be the sole indication for post- Dr Meena S Moran, Yale
mastectomy radiation, and accelerated delivery methods for TNBC should be offered on clinical trials. Preliminary University School of Medicine,
data implying a relative radioresistance for TNBC do not imply radiation omission because radiation provides an Department of Therapeutic
Radiology, New Haven, CT
absolute locoregional risk reduction. At present, the integration of subtypes in locoregional management decisions is
06520-8040, USA
still in its infancy. Until level 1 data supporting treatment decisions based on subtypes are available, standard Meena.Moran@yale.edu
locoregional management principles should be adhered to.
Introduction patients undergoing mastectomy who are at high risk,
The general principles for locoregional management of post-mastectomy radiation therapy (PMRT) diminishes
early-stage, invasive breast cancer have increased in locoregional relapses and provides a survival benefit in
complexity in the past decade because of the introduction selected patients.6 Few phase 3 data or consensus
of breast cancer classification by molecular subtypes. guidelines recommendations that categorise patients by
Although the prognostic and predictive value of breast breast cancer subtype are available to help to guide
cancer subtypes are widely recognised and clinically locoregional treatment decisions. In the absence of these
applicable to decisions regarding systemic treatment, data and guidelines, hormone-receptor negativity versus
their value for locoregional management needs further positivity has been used as a surrogate measure to
elucidation. For triple-negative breast cancer (TNBC), estimate breast cancer subtype.4 In the setting of
decisions with respect to locoregional management have neoadjuvant chemotherapy, the principles for breast
increased in complexity because of its inherent rapid conservation therapy are not modified and all patients
natural history, aggressive clinicopathological features, should receive WBRT irrespective of their pathological
high propensity for relapse, and the absence of targeted response. Decisions with respect to PMRT in the setting
treatments. Additionally, because of the substantial of neoadjuvant chemotherapy followed by mastectomy,
heterogeneity within TNBC, there are no consensus which are already complex because of an absence of
criteria when defining basal-like or triple-negative level 1 data, have been further complicated by breast
subtypes, and conflicting results from studies of cancer subtyping. Despite the enthusiasm for faster
locoregional outcomes have further complicated the radiation delivery methods—eg, accelerated partial breast
general principles of locoregional management. In this irradiation (APBI) and hypofractionated WBRT—their
Review, pertinent data, strategies, and controversies application needs to be considered in the context of
associated with the locoregional management of TNBC breast cancer subtype before their routine use in the
are assessed. treatment for TNBC.
Locoregional management Classification and characteristics of TNBC
The two main locoregional treatment pathways for early- Gene expression profiling, based on RNA expression
stage, invasive breast cancer are either breast conservation arrays of breast cancer samples with similar patterns of
therapy (defined as lumpectomy followed by whole breast gene expression, has led to the classification of
radiation therapy [WBRT] delivered with conventional five distinct molecular subtypes (luminal A or B, HER2-
fractionation) or simple mastectomy, both with positive, basal-like, and normal) of breast cancer.7,8 The
appropriate axillary nodal assessment and management. basal-like subtype was described by molecular absence or
Findings from several phase 3 studies1–3 have shown the minimum expression of receptors either for oestrogen
long-term equivalence of breast conservation therapy (ER), progesterone (PR), and HER2 (EGFR2), in addition
and mastectomy, and a meta-analysis4 of these data to high expression of c-Kit, myoepithelial cytokeratins 5,
suggested locoregional and survival benefits with the 6, and 17, and HER1 (EGFR1). For practical clinical
addition of WBRT to patients undergoing lumpectomy.4 purposes, the basal-like subtype has been defined by
Use of a radiation boost to dose-escalate a restricted area immunohistochemistry with ER, PR, and HER2 (the so-
surrounding the lumpectomy site provides an additional called triple-negative disease). As a result, although
reduction in local relapse after WBRT.5 Similarly for basal-like and triple-negative are often used
www.thelancet.com/oncology Vol 16 March 2015 e113
Review
interchangeably, they are not synonymous, with a likenesses between sporadic TNBC and BRCA1-
25–30% discordance between molecular profiling associated cancers suggest some shared similarities in
and routine three-marker immunohistochemistry the defects of underlying biological pathways, possibly a
classification.9 For example, the claudin-low subtype was fundamental defect in the BRCA1 pathway of sporadic
recently identified as a subgroup of TNBC with low TNBC.13,22,23
expression of the claudin genes, which are involved in Thus, determination of the germ-line BRCA mutation
epithelial cell interactions and junctions. This TNBC status is crucial in making decisions for locoregional
subtype, characterised by an intense immune cell management. In view of the strong association of
infiltrate, has stem-cell features and characteristics of BRCA1-associated breast cancer with TNBC, present
epithelial–mesenchymal transition (EMT) and is also guidelines for genetic screening have incorporated
thought to be triple-negative, yet is regarded as distinct TNBC so that all patients younger than 60 years with this
from basal-like cancers.10 Thus, in this Review, the term form of cancer, irrespective of family history, should be
TNBC will pertain to relevant studies classified with the considered for genetic testing.26,27 Patients should be
three-marker clinical assays and the term basal-like used clearly informed about the distinction between the risks
for classifications based on tissue microarrays, more of breast conservation therapy for BRCA carriers, which
comprehensive immunohistochemistry methods, or has an overall increased lifetime risk of both ipsilateral
molecular profiling. and contralateral local recurrence,28 by comparison with
TNBC, which comprises 15–20% of breast cancers, has patients with sporadic TNBC in which this increased risk
aggressive clinicopathological features that result in worse does not seem to be present after breast conservation
outcomes compared with other subtypes of breast therapy.12 However, cause-specifıc and overall survival
cancer.11–13 TNBC is associated with young age, BRCA1 outcomes are similar for BRCA-associated breast cancers
mutations, the black population, less mammographic with either breast conservation therapy or mastectomy.28
detection, aggressive morphological features (tumour Thus, the presence of a BRCA mutation is not a con-
necrosis, high mitotic indices, nuclear–cytoplasmic ratios, traindication for breast conservation in otherwise
high grade difference), and worse outcomes that do not appropriately selected candidates. Nevertheless, only
always correlate with traditional prognostic features, such BRCA carriers who are highly motivated to preserve their
as stage, tumour size, or nodal involvement.14–17 Data are breasts will typically choose breast conservation therapy,
conflicting as to whether patients with TNBC have a with most carriers of BRCA mutation electing to undergo
higher propensity for axillary node metastasis at definitive ipsilateral mastectomy, often with simul-
presentation than other cancer subtypes.18,19 In relation to taneous prophylactic contralateral mastectomy.
local relapses in luminal subtypes (ranges between 5 and
15 or more years), local relapses in TNBC tend to occur Locoregional relapse outcomes
much earlier (typically <5 years), presenting more In the assessment of locoregional outcomes for TNBC,
frequently with simultaneous distant metastasis than there are two crucial and distinct questions that need to
isolated local recurrences, a higher frequency of brain and be addressed. First is the determination of locoregional
pulmonary metastasis, and worse post-recurrence survival outcomes after breast conservation therapy or
outcomes.9,12,16 mastectomy for TNBC in relation to other subtypes.
Second, the more clinically relevant question is to
Association with BRCA1 mutations establish whether the more aggressive natural history of
Although only 10–20% of sporadic TNBCs harbour germ- TNBC warrants mastectomy instead of breast
line BRCA1 mutations,20 75% or more of breast cancers conservation therapy to provide an advantage in
associated with BRCA1 present the basal-like subtype of outcomes.
TNBC.21,22 Furthermore, there are striking clinicopatho-
logical similarities between BRCA1-associated breast Outcomes relative to other breast cancer subtypes
cancers and sporadic TNBC, such as high grade, high Although randomised trials of both breast conservation
proliferative indices, lymphocytic infiltrate and pushing therapy and PMRT predated classification by breast cancer
margins (a pathological characteristic) resembling subtype, a growing body of data from retrospective studies
medullary disease, a greater propensity for visceral than have classified outcomes of patients who have had breast
bone or lymphatic metastases, and notable overlaps in conservation therapy and mastectomy by breast cancer
gene expression assays, TP53 mutations, and other subtype using clinical assays. For breast conservation
chromosome abnormalities.23 Although the exact therapy, although data are conflicting, an overall temporal
mechanisms of action of BRCA1 are not yet fully trend (from 2006 up to now) suggests that TNBC (and
understood, it is involved in various cellular functions, HER2-positive disease) have higher risks of locoregional
including crucial roles in DNA repair via homologous relapses than the luminal subtypes (table 1). In 2006, when
recombination, cell-cycle checkpoint control and initial reports of outcomes for TNBC were investigated,
transcriptional regulation, X-chromosome inactivation, similar 5-year local relapses (12–17%) were reported for
and mammary gland development.24,25 Collectively, the TNBC and non-TNBC subtypes.12,29 On the basis of these
e114 www.thelancet.com/oncology Vol 16 March 2015
Review
initial studies, TNBC was concluded not to be a
n with Ntotal Median follow- Local or locoregional outcomes
contraindication for breast conservation therapy. TNBC up (years)
Additional series30 that have subsequently, but not
Haffty et al29 (2006) 117 482 7·9 TNBC 17%; non-TNBC 17%
consistently, analysed outcomes with four or more
Dent et al12 (2007) 180 1601 8·1 TNBC 12%; non-TNBC 13%
subtypes of breast cancer have suggested more locoregional
Nguyen et al30 (2008) 89 793 5·8 Luminal A 1·8%; luminal B 1·5%;
relapses after breast conservation therapy for TNBC (and HER2 8·4%; basal or TNBC 7·1%
HER2-positive disease) than for luminal subtypes, and Millar et al31 (2009) 52 482 7 Luminal A 5·1%; luminal B 8·7%;
collectively suggest about a 50% higher local or locoregional HER2-enriched 15·4%; basal-like 17·3%
relapse risk for TNBC relative to luminal subtypes. Voduc et al32 (2010) 556 2985 12 Luminal A 8%; luminal B 10%;
Differences between conclusions of series during the past luminal-HER2 9%; HER2-enriched 21%;
few years might be attributed to improved classification basal-like 14%; TNBC non-basal 8%
with guidelines to define HER2-positive disease and Billar et al33 (2010) 123 1061 2·6 Luminal A 1%; luminal B 2·9%;
HER2-enriched 2·9%; TNBC 5·7%
increased routine use of gene amplifıcation (fluorescence
Arvold et al34 (2011) 171 1434 7·1 Luminal A 0·8%; luminal B 2·3%;
in-situ hybridisation) to test for equivocal HER2 HER2-enriched 10·8%; TNBC 6·7%
immunohistochemistry,36 and analysis of outcomes by Gangi et al35 (2014) 234 1851 5·0 Luminal A 5%; luminal B 4%;
more than two subtype groups (not only by TNBC vs non- HER2-enriched 4%; TNBC 7%
TNBC). An additional factor that might contribute to the
TNBC=triple-negative breast cancer.
differences between earlier and later studies is the
development and widespread use of targeted therapies, Table 1: Selected breast conservation therapy studies that reported outcomes of triple-negative breast
such as trastuzumab and aromatase inhibitors, the effects cancer relative to other subtypes
of which decrease the risk of local relapse for patients with
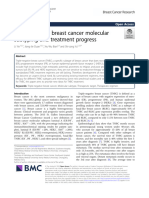
HER2-positive or ER-positive disease.37,38 Therefore, use of similarly raised risks of locoregional relapses.32 Of three
these targeted therapies in later studies might have meta-analyses40–42 that analysed locoregional outcomes in
contributed to differences in outcomes between breast TNBC, the primary focus of two was outcomes of TNBC
cancer subtypes reported by the series. .Although the in relation to other subtypes of breast cancer. One of
HER2-positive subtype was historically associated with these42 analysed 15-year outcomes in nearly 22 000 patients
poor locoregional relapse similar to TNBC, most of these treated with breast conservation therapy from 15 studies,
data were from the pre-trastuzumab era.30 Advances in and showed that TNBC, by comparison with non-TNBC,
receptor-specifıc antibody therapy and newer EGFR- had significantly worse local relapse (hazard ratio [HR]
pathway inhibitors have substantially improved loco- 3·31, 95% CI 1·69–6·45, p<0·01) and overall recurrence
regional relapse outcomes for women with HER2-positive (3·19, 1·91–5·31, p<0·01). The third meta-analysis40
disease.39 Outcomes from cohorts in which patients with included more than 12 000 patients from 15 studies
HER2-positive disease were routinely treated with treated with either breast conservation therapy or
trastuzumab suggest significantly more locoregional mastectomy and reported lower risk of locoregional
relapses only in the TNBC subgroup; patients with HER2- relapse for non-TNBC than for TNBC with breast
positive disease had similar or fewer locoregional relapses conservation therapy (relative risk [RR] 0·49, 95% CI
than those with luminal tumours.33 0·33–0·73, p=0·0005) and with mastectomy (0·66,
Worse outcomes for TNBC with breast conservation 0·53–0·83, p=0·0003). The authors concluded that
therapy are also alluded to by the latest Oxford meta- patients with TNBC are at an increased risk of developing
analysis4 of 17 randomised controlled trials of breast locoregional relapses (compared with other subtypes)
conservation therapy. An analysis of outcomes of patients irrespective of breast conservation therapy or mastectomy
who received WBRT by hormone receptor status (figure 1).
stratified by T stage, age, and grade showed that
locoregional relapse was more common in ER-poor than Breast conservation therapy versus mastectomy
in ER-rich cohorts (29% vs 14%).4 The poor prognosis of TNBC suggests the need for an
Similarly, outcomes for mastectomy (with or without aggressive locoregional surgical approach, possibly
radiation) by subtype suggest a higher locoregional necessitating removal of all breast tissue. As a result, the
relapse risk for basal-like TNBC than luminal subtypes. general longstanding principle that outcomes after
For example, a large study32 analysed locoregional breast conservation therapy and mastectomy are
relapses after precise classification into six subtypes that equivalent has been challenged in the context of patients
included distinguishing basal-like tumours from those with early-stage TNBC. Although knowledge of TNBC is
with triple-negative phenotype (with analysis of EGFR rapidly increasing, outcomes data from phase 3 studies
and cytokeratins 5 or 6) and reported the highest risk of for TNBC with breast conservation therapy in
local relapse after mastectomy in basal-like and HER2- comparison with mastectomy are scarce. In fact,
positive groups; the TNBC phenotype did not have this emerging data paradoxically suggest that breast
raised risk. Patients with basal-like or HER2-positive conservation therapy might provide improved
disease who received breast conservation therapy had locoregional outcomes compared with mastectomy for
www.thelancet.com/oncology Vol 16 March 2015 e115
Review
early-stage TNBC. For instance, investigators of a large for patients with TNBC.54 Steward and colleagues55
series analysing locoregional relapse outcomes for compared survival outcomes of TNBC by type of surgery
patients with T1–2, N0 TNBC treated with either breast and showed that treatment with radiation significantly
conservation therapy or mastectomy (no PMRT) reported improved survival in the lumpectomy group (HR 0·30,
a 6% absolute benefit in reducing locoregional relapses 95% CI 0·16–0·58, p=0·001), but PMRT did not improve
with breast conservation therapy compared with survival in the mastectomy cohort (0·38, 95% CI
mastectomy (p<0·001).40 This result suggests that breast 0·05–3·04, p=0·34), suggesting an increased biological
conservation therapy, which routinely incorporates responsiveness of TNBC to radiation (when breast tissue
radiation, might be more appropriate than mastectomy is present). Lastly, findings from two meta-analyses40,41 of
outcomes by subtype for breast conservation therapy in
A comparison with mastectomy indicated fewer loco-
Breast conserving Non-TNBC vs TNBC Relative risk (95% Cl) regional relapses after breast conservation therapy than
treatment trial mastectomy in early-stage TNBC. One41 of these meta-
Straver et al43 0·22 (0·04–1·24) analyses did a direct statistical comparison between
breast conservation therapy and mastectomy for TNBC,
Voduc et al32 0·73 (0·56–0·97)
showing fewer locoregional relapses (16·9% vs 21·9%;
31
Millar et al 0·36 (0·22–0·63) RR 0·75, 95% CI 0·65–0·87, p<0·0001) and fewer
Solin et al44 0·51 (0·23–1·18) distant metastases (23·6% vs 34·4%; RR 0·68, 95% CI
Freedman et al 45
0·85 (0·27–2·69)
0·60–0·76, p<0·00001) with breast conservation therapy
than with mastectomy. Furthermore, in the adjusted
Arvold et al34 0·26 (0·15–0·48)
analysis of only stage I or II TNBC, locoregional relapses
Haffty et al 29
0·99 (0·64–1·58) were 2·5 times more common and distant metastases
Ihemelandu et al46 0·57 (0·17–2·01) were twice as common with mastectomy than with
47
breast conservation therapy. The authors concluded that
Gabos et al 2·46 (0·46–14·41)
although TNBC is associated with worse locoregional
Meyers et al48 0·18 (0·00–1·63)
relapse outcomes than luminal subtypes, locoregional
Wong et al 49
0·09 (0·03–0·28) relapses in TNBC are diminished to a greater extent with
Siponen et al50 0·58 (0·19–1·78) breast conservation therapy than with mastectomy.41
Ultimately, the decision for patients with TNBC to have
Combined (random) 0·49 (0·33–0·73)
breast conservation therapy or mastectomy should
0·01 0·1 0·2 0·5 1 2 5 10 100 incorporate their personal preference after an in-depth
discussion about the implications of their treatment
B options in context of their individual disease specifics.
Mastectomy Non-TNBC vs TNBC Relative risk (95% Cl) Patients should be made aware that the existing data
Straver et al43 0·37 (0·07–2·08) suggest that although locoregional relapses are more
common in TNBC by comparison with luminal subtypes
Voduc et al32 0·75 (0·55–1·03) after breast conservation therapy, this risk is similarly
raised with mastectomy. Optimisation of systemic therapy
Ihemelandu et al46 0·47 (0·13–1·73) for TNBC will inevitably result in improved survival
outcomes, especially in view of their high risk of harbouring
Kyndi et al51 0·78 (0·54–1·15) micrometastasis at the time of diagnosis and competing
risk of distant relapse simultaneously with locoregional
Gabos et al47 0·38 (0·18–0·83)
relapses. On the basis of the present outcome data, the risk
of isolated locoregional relapses is low enough to support
Wang et al52 0·76 (0·47–1·27)
either breast conservation therapy or mastectomy for
Meyers et al48 0·27 (0·09–0·89)
patients with TNBC.
Mersin et al53 0·32 (0·11–0·93) PMRT
PMRT reduces the risk of locoregional relapses and
Combined (random) 0·66 (0·53–0·83) provides a survival benefit in selected patients.6,56
Traditional indications for PMRT include positive nodes,
0·01 0·1 0·2 0·5 1 2 5
positive margins, or a tumour size of more than 5 cm.57
Relative risk The higher risk for locoregional relapses in TNBC after
mastectomy raises the question as to whether the
Figure 1: Forest plots showing locoregional outcomes with breast conserving treatment (A) and mastectomy
(B) for non-TNBC relative to TNBC presence of this subtype should affect decisions to use
TNBC=triple-negative breast cancer. Figure adapted from Lowery and colleagues,40 by permission of PMRT in the absence of other high-risk features. A
Breast Cancer Research and Treatment. phase 3 trial58 of 681 patients from China with
e116 www.thelancet.com/oncology Vol 16 March 2015
Review
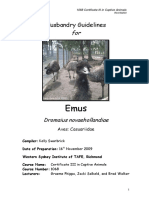
A B C
D E F
Figure 2: Radiation delivery techniques
(A) Right whole breast radiation therapy (WBRT) showing the medial tangent beam. (B) Skin rendition WBRT, medial and lateral beams. Pink section represents the
lumpectomy cavity with a margin of normal tissue. Orange line represents radiation field borders on skin. (C) Treatment-planning scan (WBRT volume), medial and
lateral beams. Axial image of treatment planning scan through the mid-chest. (D) Radiation boost. (E) Treatment-planning scan (post-mastectomy radiation therapy
volume), several beamlets generate conformal plan on chest wall. (F) Treatment-planning scan (accelerated partial breast irradiation volume): 2 cm around
lumpectomy excluding ribs; methods for delivery vary. Red sections represent areas receiving high-dose volume. Other colours represent the so-called drop-off of
radiation dose, with blue as lowest (negligible) aggregate dose.
stage I–II TNBC, all treated with mastectomy plus Use of a radiation boost (after WBRT)
chemotherapy and randomly assigned to receive PMRT A radiation boost is usually given to the area surrounding
or no radiation, reported data after a median follow-up of the tumour bed after WBRT to dose-escalate the region at
longer than 7 years. Of note, more than 80% of patients highest risk of local recurrence (figure 2). Although a
were node-negative, and more than 70% had tumours of radiation boost is regarded as optional in breast
2 cm or smaller in size. The 5-year relapse-free survival conservation therapy for early-stage invasive breast cancer,
(88·3% vs 74·6%; HR 0·77, 95% CI 0·72–0·98, p=0·02) level 1 data with long-term follow-up have shown its direct
and overall survival (90·4% vs 78·7%; HR 0·79, 0·74–0·97, effect in further reducing local relapse beyond the benefit
p=0·03) were significantly improved with the addition of reported with WBRT.5 This additional benefit was
PMRT compared with no radiation.58 Unfortunately, the significant for all age groups, with the largest proportional
clinical applicability of this study58 is limited by the benefit in women younger than 50 years and in patients
absence of detailed reporting of locoregional outcomes with high-grade tumours.61 Patients with TNBC, who are
and radiation methods, and the findings should therefore characteristically young with high-grade tumours, have an
be regarded as hypothesis generating. increased risk of harbouring microscopic disease after
Present guidelines for PMRT do not incorporate lumpectomy.62 Thus, especially for TNBC, incorporation of
subtypes of breast cancer in their recommendations. For a radiation boost to the tumour bed after WBRT is highly
example, the use of PMRT “solely based on HER2+ or likely to provide an additional benefit in reducing the risk
TNBC” has been rejected by the St Gallen International of local relapse and should be strongly considered in
Expert Consensus.59 The American Society of Clinical treatment.
Oncology has recommended PMRT for patients with four
or more positive nodes, stage T3, or stage III tumours, Faster radiation delivery methods
but state insufficient evidence to make recommendations Although a complete overview of accelerated partial
for modification of the guideline based on other tumour, breast irradiation (APBI) and hypofractionated WBRT is
patient, or treatment-related factors.60 Although PMRT beyond the scope of this Review, the widespread use of
might improve outcomes in TNBC, data reporting these approaches warrants their mention in the context
outcomes for these patients in the absence of other PMRT of TNBC. Both APBI and hypofractionated WBRT have
indications are sparse. Additional confirmatory level 1 shorter delivery times than the standard 5–6·5 weeks of
studies with adequate long-term follow-up are needed conventionally fractionated WBRT, and could improve
before TNBC subtype alone should affect standard PMRT convenience for patients and lower treatment costs.
locoregional management decisions. APBI is typically used to deliver therapeutic doses to a
www.thelancet.com/oncology Vol 16 March 2015 e117
Review
focal 2–3 cm area around the lumpectomy cavity in a even among those receiving WBRT from the trials of
treatment time typically of 5 days or less, and uses breast conservation therapy,4 the low accrual for patients
various high-dose rate brachytherapy, external beam, or with hormone receptor-poor disease was probably an
intraoperative delivery methods. By contrast, expected conservative bias of treating physicians.
hypofractionated WBRT delivers higher daily fractions Existing APBI consensus guidelines from various
and a lower (but biologically equivalent) total dose to the organisations have subtle differences in eligibility
whole breast, thus shortening time of radiation criteria, but notably only differentiate by ER status and
treatment typically to 3–4 weeks or less. Hypofractionated not by subtypes of breast cancer. Although conclusions
WBRT is based on theoretical radiobiological modelling are difficult to make about the efficacy or safety of APBI
of the underlying sensitivities of normal cells and for TNBC from the existing data, the overall poor
tumours to changes in fractionation schedules.63 outcomes of TNBC and association with young age
warrant restraint. In the absence of outcomes by breast
APBI cancer subtypes from mature phase 3 trials, APBI should
Data suggest a higher residual tumour burden for TNBC only be used, at present, for TNBC in the context of a
after lumpectomy than for other subtypes, raising clinical trial.
concerns regarding the use of APBI for this subtype. For
example, patients with TNBC have shown more so-called Hypofractionated WBRT
true recurrences (within 3 cm of the lumpectomy cavity) In many countries, hypofractionated WBRT has become
after breast conservation therapy,64 whereas the recur- the standard of care for appropriately selected patients
rences of hormone-enriched tumours present more with early-stage cancer after breast conservation therapy,
often as so-called new primaries (developing remotely with mature phase 3 data supporting its safety and
from the original lumpectomy site).65 Furthermore, effıcacy for replacing conventional fractionation. Because
analysis of the re-excision specimens suggests a higher the preponderance of existing data supporting
risk of residual invasive disease for TNBC than with hypofractionated WBRT is derived from ER-positive
other subtypes of breast cancer (odds ratio [OR] 3·28, tumours, the outcomes for hypofractionated WBRT have
95% CI 1·56–6·89, p=0·002).62 not been adequately assessed for TNBC. Present guide-
Prospective data for clinical outcomes for TNBC treated line recommendations for hypofractionated WBRT also
with APBI are scarce and conflicting. Most are do not specifically factor breast cancer subtypes into their
retrospective reviews or single-group, single-institutional recommendations to identify the most appropriate
studies with relatively short follow-up. The American patients. In view of the potential for breast cancer subtype
Society of Breast Surgeons MammoSite Registry Trial66 to have differences in underlying sensitivities to changes
reported that ER-negative disease was associated with a in radiation fractionation schedules (which forms the
higher risk of ipsilateral recurrence after APBI than with basis of hypofractionation schemas), assessment with
ER-positive tumours (OR 4·01, 95% CI 1·87–8·57, radiobiological modelling and clinical trials needs to be
p=0·0003). Similarly, single-institutional studies have done before routine use of this treatment for TNBC.
reported significantly higher in-breast failure rates in Until then, hypofractionated WBRT should be used with
patients with ER-negative breast cancer than in patients some caution for TNBC. Irrespectively, the high frequency
with ER-positive disease who were treated with APBI.67,68 of chemotherapy, often young age, and advanced disease
A single-institutional prospective APBI study69 recorded of patients with TNBC often precludes the clinical
an excessive 5-year actuarial in-breast local recurrence applicability of hypofractionated WBRT for this subtype.
rate of 33% in the group with TNBC. Similarly, the ELIOT
(electron intra-operative radiation therapy) off-protocol, Increased radiosensitivity or radioresistance?
retrospective APBI study70 reported higher risks of true An area of controversy that might affect decisions for the
failures and elsewhere failures (breast failures) in patients locoregional management of TNBC pertains to whether
with TNBC after APBI. the subtype is biologically radioresistant or predisposed
By contrast, other single-institutional, retrospective to radiosensitivity. These concerns regarding radio-
APBI series71,72 have reported excellent 5-year actuarial in- resistance stem from interpretation of data from patients
breast failure of 0–3% for TNBC. These conflicting data treated on the PMRT trials and, to a lesser extent, trials of
are difficult to interpret because of the diversity in delivery breast conservation therapy. In a subset of patients with
techniques, patient selection, and level of expertise for available tissue from the Danish post-mastectomy trials
delivering APBI. Of note, ongoing phase 3 trials have yet 82b/c73 treated with and without PMRT, breast cancer
to report long-term outcomes, and the NSABP B-39/ subtypes were retrospectively established by clinical
RTOG 0413 trial (WBRT vs APBI), which is now closed to assays and outcomes were analysed as a function of these
accrual and in active follow-up, was slowest to accrue subtypes. Although the baseline (without PMRT)
patients with ER-negative disease (ClinicalTrials.gov probability of locoregional relapse for TNBC was signi-
NCT00103181). In view of the documented increased risk ficantly increased by comparison with luminal subtypes,
of locoregional relapse in patients with ER-poor disease, and the addition of PMRT resulted in a significant
e118 www.thelancet.com/oncology Vol 16 March 2015
Review
improvement in locoregional relapses for every subtype A possible explanation for these opposing theories for
(table 2), the proportional benefit was substantially less differential responses with radiation might be related to
for the triple-negative subtype than for the luminal and the present clinical categorisation of TNBCs into one
hormone-receptor positive cohorts. This finding was general subtype, which might be an oversimplification of
interpreted to suggest a relative radioresistance in a diverse subgroup of cancers with different underlying
patients with TNBC (and HER2-positive) disease.73 Data tumorigenic pathways. This concept has similarly been
from the 2011 Oxford meta-analysis4 of breast suggested for the differential responses noted with
conservation therapy trials similarly suggested an neoadjuvant systemic chemotherapy, in which TNBCs
inherent difference in radio-response based on the extent are generally thought to be chemo-sensitive with
of hormone receptor expression. Patients stratified by relatively high pathological complete response rates
receipt of radiotherapy, T stage, ER status, age, and grade relative to luminal subtypes. For example, despite the
were analysed by outcomes. Concordant with the high proportion of patients achieving pathological
findings from PMRT trials, the overall relapse risk was complete response (nearly 30%) for TNBC, this subtype
higher for patients with ER-poor than ER-enriched has a substantially higher frequency of distant metastasis
disease after lumpectomy alone; with the addition of and worse survival outcomes than other subtypes of
radiation, the benefit in local relapse was proportionally breast cancer. Although the proportion of patients who
less in patients with ER-poor disease, which has been achieve a pathological complete response have outcomes
suggested to be a relative radioresistance for patients
with poor expression of hormone receptors.4
LRR (%) Absolute difference
Although these reported differences in radiation
response from the PMRT and breast conservation Without PMRT With PMRT
therapy trials are striking, these analyses have not been Lum A 32% 3% 29%
validated in other cohorts and thus should be interpreted Lum B 48% 3% 48%
with caution. Importantly, for the TNBC analysis from TNBC 32% 15% 17%
PMRT trials, the addition of radiation did provide a HER2+ 33% 21% 12%
significant benefit of more than 50% in reducing isolated
Greater relative benefit of radiation is suggested for luminal subtypes or those
locoregional relapses (32% with no PMRT vs 15% with with oestrogen receptors, than for those with the TNBC subtype. Data are from
PMRT; p<0·001; table 2). Thus, radiation should not be Kyndi and colleagues73 (patients treated in the Danish post-mastectomy trials).
omitted in TNBC on the basis of these data, particularly LRR=locoregional relapses. PMRT=post-mastectomy radiation therapy.
Lum A=luminal A. Lum B=luminal B. TNBC=triple-negative breast cancer.
when the conflicting hypothesis that patients with TNBC
have a defect in the BRCA1 pathway (which should make Table 2: Radiation treatment for patients of different breast cancer
them inherently more radiosensitive) in combination subtypes who had a mastectomy
with clinical data that suggested a benefit with radiation
with TNBC in both breast conservation therapy and
PMRT settings, are taken into consideration.41,55,58 At A B
present, the traditional general principles of adjuvant Cell cycle or Androgen, oestrogen, or Pathological complete response
DNA repair genes steroid metabolism genes rate by subtype
radiation should be applied for TNBC until its predictive Luminal 10% Luminal androgen receptor
value by breast cancer subtype is better understood. androgen 33% Unstable
The opposing theory of radiosensitivity is from 30% Immunomodulatory
Basal-like 31% Mesenchymal
theoretical and preclinical data that suggest the inherent Unstable 23% Mesenchymal stem-like
inability of BRCA carriers to repair treatment-induced 52% Basal-like 1
0% Basal-like 2
damage, which would potentially provide a benefit in
tumour-cell killing, but simultaneously would make
surrounding normal tissue susceptible to radiation- Immunomodulatory
related complications. TNBC, sharing clinical-
pathological similarities with BRCA1 carriers, is often Mesenchymal-like
Immune
characterised by an impaired DNA repair process. As response
such, the increased sensitivity to specific chemo- genes
therapeutic drugs (ie, platinum-based drugs) and
radiotherapy has been extrapolated from BRCA carriers Cellular differentiation,
to include sporadic TNBC. However, the preclinical data motility, or growth
factor pathways
for increased radiosensitivity (with respect to increased
toxic effects on normal tissues) are conflicting,74,75 and Figure 3: Proposed triple-negative breast cancer subtypes that are predictors of neoadjuvant chemotherapy
from a clinical standpoint there is a paucity of data to response
Data are from Lehmann and colleagues79 and from Masuda and colleagues.80 (A) Relative frequency of basal triple-
support the suggestion that BRCA carriers or patients negative breast cancer (TNBC) subtypes. (B) Proportion of patients with every subtype who have a pathological
with TNBC have worsened acute or chronic radiation complete response rate. Pathological complete response rates vary significantly (p=0·043) by TNBC subtype
toxic effects with the use of this treatment.76,77 (adjusted for age, clinical stage treatment type, and nuclear grade).
www.thelancet.com/oncology Vol 16 March 2015 e119
Review
patient outcomes. Although the associations between
Search strategy and selection criteria subtypes of breast cancer and locoregional relapses are
References for this Review were identified through searches equally compelling, integration of these subtypes into
of PubMed for papers published before Aug 10, 2014, and in the decision making for local management is lagging
English with the search terms “triple-negative”, “radiation because of the paucity of level 1 data to support
therapy”, and “local relapse”. Articles were also identified treatment decisions. Although TNBC poses a great
through searches of the author’s personal files. The final challenge because of its aggressive nature, the absence
reference list was generated on the basis of relevance to the of targeted drugs, heterogeneity within this subtype,
broad scope of this Review; those articles deemed not and our understanding of this subtype still in its infancy,
pertinent were excluded. the general principles of locoregional management with
radiation should not be changed. Individualised care is
expected to be based on phenotypic markers of
that are nearly identical to patients who do not have the individual tumour characteristics and might, one day,
TNBC subtype (non-TNBC), the overall unfavourable direct adjuvant treatment decisions by taking into
outcomes of TNBC subtype are attributed to the subset of account the intrinsic risks of locoregional relapses. For
patients whose disease is relatively chemo-resistant and TNBC, subclassification based on underlying defects
who have residual disease after neoadjuvant chemo- could provide more targeted treatments that might
therapy.78 directly enhance local control and possibly provide
On the basis of findings from gene-expression profiling radiosensitising effects. Present data discussed in this
of breast cancer reported in 2011, at least seven distinct Review should be regarded as hypothesis-generating,
subtypes of TNBC have been defined (figure 3): two basal- because no single locoregional management approach
like (BL1/BL2), two mesenchymal (mesenchymal and has consistently been reproduced to show benefits over
mesenchymal stem-like), one immunomodulatory, one another approach. Thus, at this juncture, TNBC subtype
luminal, and an unstable variant.79 Although the initial alone should not guide locoregional treatment decisions
clinical relevance of this subclassification for TNBC was as it does for systemic treatment. Patients with TNBC
unclear, pivotal studies have made progress towards their should be encouraged to participate in clinical trials to
clinical application. For example, these TNBC subtypes further elucidate the many unanswered questions
have been correlated to the likelihood of pathological surrounding the management of this aggressive subtype
complete response with standard neoadjuvant chemo- of breast cancer. Until phase 3 trials provide data to
therapy regimens (p=0·04379).66 Furthermore, data from a adequately redirect present standard locoregional
trial81 suggest a direct association between the quantities management principles based on subtypes of breast
of tumour-infiltrating lymphocytes in individual TNBC cancer, major deviations from the existing clinical
tumours and improved survival outcomes in the setting practices should be avoided outside of a clinical trial
of adjuvant anthracycline-based chemotherapy. Different setting.
subtypes of TNBC might be sensitive to different Contributors
therapeutic regimens based on their main underlying MSM researched and reviewed the existing literature and wrote the
defects;82 if so, novel therapeutic strategies using targeted manuscript.
drugs directed towards underlying defects of the TNBC Declaration of interests
subtype (eg, immune modulation in tumour-infiltrating I declare no competing interests.
lymphocyte-depleted TNBC) might provide better References
1 Fisher B, Anderson S, Bryant J, et al. Twenty-year follow-up of a
responses to improve overall outcomes for patients. randomized trial comparing total mastectomy, lumpectomy, and
Similarly, the different radiosensitivities of TNBC could lumpectomy plus irradiation for the treatment of invasive breast
be associated with differences in underlying biological cancer. N Engl J Med 2002; 347: 1233–41.
mechanisms and, with further elucidation, the addition 2 Poggi M, Danforth D, Sciuto L, et al. Eighteen-year results in the
treatment of early breast carcinoma with mastectomy versus breast
of radiosensitising drugs to radiation therapy might help conservation therapy: the National Cancer Institute Randomized
to provide additional reductions in locoregional relapse. Trial. Cancer 2003; 98: 697–702.
However, with respect to present clinical practices, 3 Veronesi U, Cascinelli N, Mariani L, et al. Twenty-year follow-up of
a randomized study comparing breast-conserving surgery with
contemporary series show that absolute local recurrence radical mastectomy for early breast cancer. N Engl J Med 2002;
risk of TNBC is acceptable and only slightly increased 347: 1227–32.
relative to the other subtypes,35 which supports the view 4 Early Breast Cancer Trialists’ Collaborative Group. Effect of
radiotherapy after breast-conserving surgery on 10-year recurrence
that TNBC (and BRCA1-associated) tumours are, in fact, and 15-year breast cancer death: meta-analysis of individual patient
responsive to DNA-damaging drugs. data for 10 801 women in 17 randomised trials. Lancet 2011;
378: 1707–16.
5 Bartelink H, Horiot JC, Poortmans PM, et al. Impact of a higher
Conclusions radiation dose on local control and survival in breast-conserving
Classification of breast cancers by molecular subtype therapy of early breast cancer: 10-year results of the randomized
has proven to be prognostic, allows for tailoring of boost versus no boost EORTC 22881-10882 trial. J Clin Oncol 2007;
25: 3259–65.
systemic therapy, and has led to improvements in
e120 www.thelancet.com/oncology Vol 16 March 2015
Review
6 Overgaard M. Overview of randomized trials in high risk breast 29 Haffty BG, Yang Q, Reiss M, et al. Locoregional relapse and distant
cancer patients treated with adjuvant systemic therapy with or metastasis in conservatively managed triple negative early-stage
without postmastectomy irradiation. Semin Radiat Oncol 1999; breast cancer. J Clin Oncol 2006; 24: 5652–57.
9: 292–99. 30 Nguyen PL, Taghian AG, Katz MS, et al. Breast cancer subtype
7 Perou C, Sorlie T, Eisen M, et al. Molecular portraits of human approximated by estrogen receptor, progesterone receptor, and
breast tumours. Nature 2000; 406: 747–52. HER-2 is associated with local and distant recurrence after
8 Sorlie T, Perou CM, Tibshirani R, et al. Gene expression patterns of breast-conserving therapy. J Clin Oncol 2008; 26: 2373–78.
breast carcinomas distinguish tumor subclasses with clinical 31 Millar EK, Graham PH, O’Toole SA, et al. Prediction of local
implications. Proc Natl Acad Sci USA 2001; 98: 10869–74. recurrence, distant metastases, and death after breast-conserving
9 Nielsen TO, Hsu FD, Jensen K, et al. Immunohistochemical and therapy in early-stage invasive breast cancer using a five-biomarker
clinical characterization of the basal-like subtype of invasive breast panel. J Clin Oncol 2009; 27: 4701–08.
carcinoma. Clin Cancer Res 2004; 10: 5367–74. 32 Voduc KD, Cheang MCU, Tyldesley S, Gelmon K, Nielsen TO,
10 Perou CM. Molecular stratification of triple-negative breast cancers. Kennecke H. Breast cancer subtypes and the risk of local and
Oncologist 2010; 15 (suppl 5): 39–48. regional relapse. J Clin Oncol 2010; 28: 1684–91.
11 Boyle P. Triple-negative breast cancer: epidemiological 33 Billar JA, Dueck AC, Stucky CC, et al. Triple-negative breast
considerations and recommendations. Ann Oncol 2012; cancers: unique clinical presentations and outcomes.
23 (suppl 6): vi7–vi12. Ann Surg Oncol 2010; 17 (suppl 3): 384–90.
12 Dent R, Trudeau M, Pritchard KI, et al. Triple-negative breast 34 Arvold ND, Taghian AG, Niemierko A, et al. Age, breast cancer
cancer: clinical features and patterns of recurrence. Clin Cancer Res subtype approximation, and local recurrence after breast-conserving
2007; 13: 4429–34. therapy. J Clin Oncol 2011; 29: 3885–91.
13 Sorlie T, Tibshirani R, Parker J, et al. Repeated observation of breast 35 Gangi A, Chung A, Mirocha J, Liou DZ, Leong T, Giuliano AE.
tumor subtypes in independent gene expression data sets. Breast-conserving therapy for triple-negative breast cancer.
Proc Natl Acad Sci USA 2003; 100: 8418–23. JAMA Surg 2014; 149: 252–58.
14 Bauer KR, Brown M, Cress RD, Parise CA, Caggiano V. 36 Wolff AC, Hammond ME, Hicks DG, et al. Recommendations for
Descriptive analysis of estrogen receptor (ER)-negative, human epidermal growth factor receptor 2 testing in breast cancer:
progesterone receptor (PR)-negative, and HER2-negative American Society of Clinical Oncology/College of American
invasive breast cancer, the so-called triple-negative phenotype: Pathologists clinical practice guideline update. J Clin Oncol 2013;
a population-based study from the California cancer registry. 31: 3997–4013.
Cancer 2007; 109: 1721–28. 37 Romond EH, Perez EA, Bryant J, et al. Trastuzumab plus adjuvant
15 Fulford LG, Easton DF, Reis-Filho JS, et al. Specific morphological chemotherapy for operable HER2-positive breast cancer.
features predictive for the basal phenotype in grade 3 invasive N Engl J Med 2005; 353: 1673–84.
ductal carcinoma of breast. Histopathology 2006; 49: 22–34. 38 Fisher B, Bryant J, Dignam JJ, et al. Tamoxifen, radiation therapy, or
16 Carey LA PC, Livasy CA, Dressler LG, et al. Race, breast cancer both for prevention of ipsilateral breast tumor recurrence after
subtypes, and survival in the Carolina Breast Cancer Study. JAMA lumpectomy in women with invasive breast cancers of one
2006; 295: 2492–503. centimeter or less. J Clin Oncol 2002; 20: 4141–49.
17 Moran MS, Yang Q, Harris LN, Jones B, Tuck DP, Haffty BG. Long- 39 Romond E, Perez E, Bryant J, et al. Trastuzumab plus adjuvant
term outcomes and clinicopathologic differences of African- chemotherapy for operable HER2-positive breast cancer.
American versus white patients treated with breast conservation N Engl J Med 2005; 353: 1673–84.
therapy for early-stage breast cancer. Cancer 2008; 113: 2565–74. 40 Lowery A, Kell M, Glynn R, Kerin M, Sweeney K. Locoregional
18 Jones T, Neboori H, Wu H, et al. Are breast cancer subtypes recurrence after breast cancer surgery: a systematic review by
prognostic for nodal involvement and associated with receptor phenotype. Breast Cancer Res Treat 2012; 133: 831–41.
clinicopathologic features at presentation in early-stage breast 41 Wang J, Xie X, Wang X, et al. Locoregional and distant
cancer? Ann Surg Oncol 2013; 20: 2866–72. recurrences after breast conserving therapy in patients with
19 Lin NU, Vanderplas A, Hughes ME, et al. Clinicopathologic triple-negative breast cancer: a meta-analysis. Surg Oncol 2013;
features, patterns of recurrence, and survival among women with 22: 247–55.
triple-negative breast cancer in the National Comprehensive Cancer 42 Chen J, Jiang P, Wang H, et al. The efficacy of molecular
Network. Cancer 2012; 118: 5463–72. subtyping in predicting postoperative recurrence in breast-
20 Gonzalez-Angulo AM, Timms KM, Liu S, et al. Incidence and conserving therapy: a 15-study meta-analysis. World J Surg Oncol
outcome of BRCA mutations in unselected patients with triple 2014; 12: 212.
receptor-negative breast cancer. Clin Cancer Res 2011; 17: 1082–89. 43 Straver ME, Rutgers EJ, Rodenhuis S, et al. The relevance of breast
21 Lakhani S, Reis-Filho J, Fulford L, et al. Prediction of BRCA1 status cancer subtypes in the outcome of neoadjuvant chemotherapy.
in patients with breast cancer using estrogen receptor and basal Ann Surg Oncol 2010; 17: 2411–18.
phenotype. Clin Cancer Res 2005; 11: 5175–80. 44 Solin LJ, Hwang WT, Vapiwala N. Outcome after breast
22 Foulkes WD, Smith IE, Reis-Filho JS. Triple-negative breast cancer. conservation treatment with radiation for women with
N Engl J Med 2010; 363: 1938–48. triplenegative early-stage invasive breast carcinoma.
23 Yehiely F, Moyano JV, Evans JR, Nielsen TO, Cryns VL. Clin Breast Cancer 2009; 9: 96–100.
Deconstructing the molecular portrait of basal-like breast cancer. 45 Freedman GM, Anderson PR, Li T, et al. Locoregional recurrence of
Trends Mol Med 2006; 12: 537–44. triple-negative breast cancer after breast-conserving surgery and
24 James C, Quinn J, Mullan P. BRCA1, a potential predictive radiation. Cancer 2009; 115: 946–51.
biomarker in the treatment of breast cancer. Oncologist 2007; 46 Ihemelandu CU, Naab TJ, Mezghebe HM, et al. Treatment and
12: 142–50. survival outcome for molecular breast cancer subtypes in black
25 Scully R, Livingston DM. In search of the tumour-suppressor women. Ann Surg 2008; 247: 463–469
functions of BRCA1 and BRCA2. Nature 2000; 408: 429–32. 47 Gabos Z, Thoms J, Ghosh S, et al. The association between
26 American Society of Clinical Oncology. American Society of Clinical biological subtype and locoregional recurrence in newly diagnosed
Oncology policy statement update: genetic testing for cancer breast cancer. Breast Cancer Res Treat 2010; 124: 187–94.
susceptibility. J Clin Oncol 2003; 21: 2397–406. 48 Meyers MO, Klauber-Demore N, Ollila DW, et al. Impact of breast
27 Robson ME, Storm CD, Weitzel J, Wollins DS, Offit K. American cancer molecular subtypes on locoregional recurrence in patients
Society of Clinical Oncology policy statement update: genetic and treated with neoadjuvant chemotherapy for locally advanced breast
genomic testing for cancer susceptibility. J Clin Oncol 2010; cancer. Ann Surg Oncol 2011; 18: 2851–57.
28: 893–901. 49 Wong FY, Chin FK, Lee KA, Soong YL, Chua ET. Hormone
28 Pierce LJ, Phillips KA, Griffith KA, et al. Local therapy in BRCA1 receptors and HER-2 status as surrogates for breast cancer
and BRCA2 mutation carriers with operable breast cancer: molecular subtypes prognosticate for disease control in node
comparison of breast conservation and mastectomy. negative Asian patients treated with breast conservation therapy.
Breast Cancer Res Treat 2010; 121: 389–98. Ann Acad Med Singapore 2011; 40: 90–97.
www.thelancet.com/oncology Vol 16 March 2015 e121
Review
50 Siponen ET, Vaalavirta L, Joensuu H, Vironen J, Heikkilä P, 66 Shaitelman SF, Vicini FA, Beitsch P, Haffty B, Keisch M, Lyden M.
Leidenius MH. Ipsilateral breast recurrence after breast conserving Five-year outcome of patients classified using the American Society
surgery in patients with small (B2 cm) breast cancer treated with for Radiation Oncology consensus statement guidelines for the
modern adjuvant therapies. Eur J Surg Oncol 2011; 37: 25–31. application of accelerated partial breast irradiation: an analysis of
51 Kyndi M, Sørensen FB, Knudsen H, et al. Estrogen receptor, patients treated on the American Society of Breast Surgeons
progesterone receptor, HER-2, and response to postmastectomy MammoSite Registry Trial. Cancer 2010; 116: 4677–85.
radiotherapy in high-risk breast cancer: the Danish Breast Cancer 67 McHaffie DR, Patel RR, Adkison JB, Das RK, Geye HM,
Cooperative Group. J Clin Oncol 2008; 26: 1419–26. Cannon GM. Outcomes after accelerated partial breast irradiation
52 Wang SL, Li YX, Song YW, et al. Triple-negative or HER2-positive in patients with ASTRO consensus statement cautionary features.
status predicts higher rates of locoregional recurrence in node- Int J Radiat Oncol Biol Phys 2011; 81: 46–51.
positive breast cancer patients after mastectomy. 68 Stull TS, Goodwin CM, Gracely EJ, et al. A single-institution review
Int J Radiat Oncol Biol Phys 2010; 80: 1095–101. of accelerated partial breast irradiation in patients considered
53 Mersin H, Gülben K, Berberoğlu U, et al. Prognostic factors “cautionary” by the American Society for Radiation Oncology.
affecting postmastectomy locoregional recurrence in patients with Ann Surg Oncol 2012; 19: 553–59.
early breast cancer: are intrinsic subtypes effective? World J Surg 69 Pashtan IM, Recht A, Ancukiewicz M, et al. External beam
2011; 35: 2196–202. accelerated partial-breast irradiation using 32 gy in 8 twice-daily
54 Abdulkarim BS, Cuartero J, Hanson J, Deschenes J, Lesniak D, fractions: 5-year results of a prospective study.
Sabri S. Increased risk of locoregional recurrence for women with Int J Radiat Oncol Biol Phys 2012; 84: e271–77.
T1-2N0 triple-negative breast cancer treated with modified radical 70 Veronesi U, Orecchia R, Luini A, et al. Intraoperative radiotherapy
mastectomy without adjuvant radiation therapy compared with during breast conserving surgery: a study on 1,822 cases treated
breast-conserving therapy. J Clin Oncol 2011; 29: 2852–58. with electrons. Breast Cancer Res Treat 2010; 124: 141–51.
55 Steward LT, Gao F, Taylor MA, Margenthaler JA. Impact of radiation 71 Wilkinson JB, Reid RE, Shaitelman SF, et al. Outcomes of breast
therapy on survival in patients with triple-negative breast cancer. cancer patients with triple negative receptor status treated with
Oncol Lett 2014; 7: 548–52. accelerated partial breast iradiation. Int J Radiat Oncol Biol Phys
56 EBCTCG (Early Breast Cancer Trialists’ Collaborative Group). Effect 2011; 81: e159–64.
of radiotherapy after mastectomy and axillary surgery on 10-year 72 Wilder RB, Curcio LD, Khanijou RK, et al. Results with accelerated
recurrence and 20-year breast cancer mortality: meta-analysis of partial breast irradiation in terms of estrogen receptor, progesterone
individual patient data for 8135 women in 22 randomised trials. receptor, and human growth factor receptor 2 status.
Lancet 2014; 383: 2127–35. Int J Radiat Oncol Biol Phys 2010; 78: 799–803.
57 Truong P, Olivotto I, Whelan T, Levine M, Steering Committee on 73 Kyndi M, Sorensen FB, Knudsen H, et al. Estrogen receptor,
Clinical Practice Guidelines for the Care and Treatment of Breast progesterone receptor, HER-2, and response to postmastectomy
Cancer. Clinical practice guidelines for the care and treatment of radiotherapy in high-risk breast cancer: the Danish Breast Cancer
breast cancer: 16. locoregional post-mastectomy radiotherapy. Cooperative Group. J Clin Oncol 2008; 26: 1419–26.
CMAJ 2004; 170: 1263–73. 74 Baeyens A, Thierens H, Claes K, Poppe B, De Ridder L, Vral A.
58 Wang J, Shi M, Ling R, et al. Adjuvant chemotherapy and Chromosomal radiosensitivity in BRCA1 and BRCA2 mutation
radiotherapy in triple-negative breast carcinoma: a prospective carriers. Int J Radiat Oncol Biol Phys 2004; 80: 745–56.
randomized controlled multi-center trial. Radiother Oncol 2011; 75 Trenz K, Lugowski S, Jahrsdorfer U, Jainta S, Vogel W, Speit G.
100: 200–04. Enhanced sensitivity of peripheral blood lymphocytes from women
59 Goldhirsch A, Winer EP, Coates AS, et al. Personalizing the carrying a BRCA1 mutation towards the mutagenic effects of
treatment of women with early breast cancer: highlights of the various cytostatics. Mutat Res 2003; 544: 279–88.
St Gallen International Expert Consensus on the Primary Therapy 76 Gaffney DK, Brohet RM, Lewis CM, et al. Response to radiation
of Early Breast Cancer 2013. Ann Oncol 2013; 24: 2206–23. therapy and prognosis in breast cancer patients with BRCA1 and
60 Recht A, Edge SB, Solin LJ, et al. Postmastectomy radiotherapy: BRCA2 mutations. Radiother Oncol 1998; 47: 129–36.
clinical practice guidelines of the American Society of Clinical 77 Pierce LJ, Strawderman M, Narod SA, et al. Effect of radiotherapy
Oncology. J Clin Oncol 2001; 19: 1539–69. after breast-conserving treatment in women with breast cancer and
61 Jones HA, Antonini N, Hart AA, et al. Impact of pathological germline BRCA1/2 mutations. J Clin Oncol 2000; 18: 3360–69.
characteristics on local relapse after breast-conserving therapy: 78 Liedtke C, Mazouni C, Hess KR, et al. Response to neoadjuvant
a subgroup analysis of the EORTC boost versus no boost trial. therapy and long-term survival in patients with triple-negative
J Clin Oncol 2009; 27: 4939–47. breast cancer. J Clin Oncol 2008; 26: 1275–81.
62 Sioshansi S, Ehdaivand S, Cramer C, Lomme MM, Price LL, 79 Lehmann BD, Bauer JA, Chen X, et al. Identification of human
Wazer DE. Triple negative breast cancer is associated with an triple-negative breast cancer subtypes and preclinical models for
increased risk of residual invasive carcinoma after lumpectomy. selection of targeted therapies. J Clin Invest 2011; 121: 2750–67.
Cancer 2012; 118: 3893–98. 80 Masuda H, Baggerly KA, Wang Y, et al. Differential response to
63 Rowe B, Moran MS. Accelerated partial breast irradiation and neoadjuvant chemotherapy among 7 triple-negative breast cancer
hypofractionated whole breast radiation. US Oncol Hematol molecular subtypes. Clin Cancer Res 2013; 19: 5533–40.
2011; 7: 31–37. 81 Adams S, Gray RJ, Demaria S, et al. Prognostic value of tumor-
64 Hattangadi-Gluth JA, Wo JY, Nguyen PL, et al. Basal subtype of infiltrating lymphocytes in triple-negative breast cancers from two
invasive breast cancer is associated with a higher risk of true phase III randomized adjuvant breast cancer trials: ECOG 2197 and
recurrence after conventional breast-conserving therapy. ECOG 1199. J Clin Oncol 2014 32: 2959-67.
Int J Radiat Oncol Biol Phys 2012; 82: 1185–91. 82 Chiorean R, Braicu C, Berindan-Neagoe I. Another review on triple
65 Huang E, Buchholz TA, Meric F, et al. Classifying local disease negative breast cancer. Are we on the right way towards the exit
recurrences after breast conservation therapy based on location and from the labyrinth? Breast 2013; 22: 1026–33.
histology. Cancer 2002; 95: 2059–67.
e122 www.thelancet.com/oncology Vol 16 March 2015
You might also like
- Breast Disease: Diagnosis and Pathology, Volume 1From EverandBreast Disease: Diagnosis and Pathology, Volume 1Adnan AydinerNo ratings yet
- Journal Reading (Rizki Hakim Anik)Document13 pagesJournal Reading (Rizki Hakim Anik)Rhandy SeptiantoNo ratings yet
- Literatür 4Document9 pagesLiteratür 4Görkem TürkkanNo ratings yet
- Triple Negative Breast Cancer Therapy Current and Future Perspectives (Review)Document17 pagesTriple Negative Breast Cancer Therapy Current and Future Perspectives (Review)asdffdsaNo ratings yet
- Birkbak 2018Document11 pagesBirkbak 2018adiNo ratings yet
- TNBC PMRTDocument7 pagesTNBC PMRTMed MedNo ratings yet
- 8424365Document8 pages8424365Melody CyyNo ratings yet
- Thesis Projects Call 1 2022 02Document45 pagesThesis Projects Call 1 2022 02Muhammad Nehal KhanNo ratings yet
- Breast Cancer Treatments - Updates and New Challenges - PMCDocument75 pagesBreast Cancer Treatments - Updates and New Challenges - PMCWadood Md ZahedNo ratings yet
- BreastDocument14 pagesBreastAnitei GabrielaNo ratings yet
- Germline Breast Cancer SuspectibiliyDocument13 pagesGermline Breast Cancer SuspectibiliyDominick Dayton FinettiNo ratings yet
- 410-Article Text-1440-1-10-20211018Document7 pages410-Article Text-1440-1-10-20211018silviatengkerNo ratings yet
- TNBCDocument13 pagesTNBCSilvi Zakiyatul IlmiyahNo ratings yet
- Distant Breast CancerDocument10 pagesDistant Breast CancerMarion PootenNo ratings yet
- 10.1186 - s13058 017 0846 1Document14 pages10.1186 - s13058 017 0846 1Ober Van Gómez LópezNo ratings yet
- Triple-Negative Breast Cancer CHEMO PDFDocument13 pagesTriple-Negative Breast Cancer CHEMO PDFVikash SinghNo ratings yet
- 3 254 1 PBDocument5 pages3 254 1 PBbeepboop20No ratings yet
- Afp 20100601 P 1339Document8 pagesAfp 20100601 P 1339xiaojun yangNo ratings yet
- Nihms 954535Document22 pagesNihms 954535Carlos NoronaNo ratings yet
- CommentaryDocument3 pagesCommentaryGodha KiranaNo ratings yet
- Prophylactic Irradiation To The Contralateral BreaDocument6 pagesProphylactic Irradiation To The Contralateral Breaashnamuni07No ratings yet
- Intl Journal of Cancer - 2020 - Chen - Platinum Based Chemotherapy in Advanced Triple Negative Breast Cancer A MulticenterDocument10 pagesIntl Journal of Cancer - 2020 - Chen - Platinum Based Chemotherapy in Advanced Triple Negative Breast Cancer A MulticenterAndrianna NastasyaNo ratings yet
- Advances in Screening, Diagnosis, and Treatment ofDocument7 pagesAdvances in Screening, Diagnosis, and Treatment ofBastomy EkaNo ratings yet
- Dentistry at Best RationaleDocument2 pagesDentistry at Best RationaleObamaNo ratings yet
- BRCA 12-Mutation Related and Sporadic Breast and ODocument15 pagesBRCA 12-Mutation Related and Sporadic Breast and OWojtek JanotaNo ratings yet
- Use of A Tumour Bed Boost As Part of Radiotherapy For Breast CancerDocument2 pagesUse of A Tumour Bed Boost As Part of Radiotherapy For Breast CancerMaria MuñozNo ratings yet
- PMRT TNBCDocument8 pagesPMRT TNBCMed MedNo ratings yet
- Comprehensive Precision Medicine Study Protocol On The Heterogeneity of Taiwanese Breast Cancer PatientsDocument14 pagesComprehensive Precision Medicine Study Protocol On The Heterogeneity of Taiwanese Breast Cancer Patients郭竹瑩No ratings yet
- Howard 2012Document5 pagesHoward 20121alexandra12No ratings yet
- BCTT 8 093Document15 pagesBCTT 8 093Luis SanchezNo ratings yet
- BGRT 1Document10 pagesBGRT 1Nelson Appiah-AgyeiNo ratings yet
- Endometrial CancerDocument12 pagesEndometrial CancermersinonkolojiNo ratings yet
- Journal Synthesis On TumorsDocument2 pagesJournal Synthesis On TumorsKobi Carl MangopotNo ratings yet
- Fuller 2008 Breast Cancer PrevenDocument2 pagesFuller 2008 Breast Cancer PrevenJessica RosarioNo ratings yet
- Editorial: Molecular Imaging in Breast CancerDocument4 pagesEditorial: Molecular Imaging in Breast CancerKurnia AlkatiriNo ratings yet
- البحث الاول Metaplastic BreastDocument10 pagesالبحث الاول Metaplastic Breastsherifref3atNo ratings yet
- Diagnóstico y Tratamiento Del Cáncer Colorrectal MetastásicoDocument17 pagesDiagnóstico y Tratamiento Del Cáncer Colorrectal MetastásicoNICOLÁS DANIEL SANCHEZ HERNANDEZNo ratings yet
- HNF 5 SRO Chera2018Document8 pagesHNF 5 SRO Chera2018Abhinav IngleNo ratings yet
- Systemic Therapy in The Curative Treatment of Head and Neck Squamous Cell Cancer: A Systematic ReviewDocument11 pagesSystemic Therapy in The Curative Treatment of Head and Neck Squamous Cell Cancer: A Systematic ReviewLorena Sánchez PérezNo ratings yet
- 292 2021 Article 946Document12 pages292 2021 Article 946bilou hertNo ratings yet
- Breast Cancer Mrker NatureDocument12 pagesBreast Cancer Mrker Naturerajasekaran_mNo ratings yet
- A Review of Triple-Negative Breast Cancer: Nick Patten. Last Light (Detail) - Oil On Canvas, 44" × 56"Document4 pagesA Review of Triple-Negative Breast Cancer: Nick Patten. Last Light (Detail) - Oil On Canvas, 44" × 56"Kritik KumarNo ratings yet
- EJGO2022054 Cervical CaDocument8 pagesEJGO2022054 Cervical CaRahmayantiYuliaNo ratings yet
- Surgical Management of Axilla of Triple-Negative Breast Cancer in The Z1071 Era: A Propensity Score-Matched Analysis of The National Cancer DatabaseDocument13 pagesSurgical Management of Axilla of Triple-Negative Breast Cancer in The Z1071 Era: A Propensity Score-Matched Analysis of The National Cancer DatabasesamuelNo ratings yet
- Colorectal Cancer StagingDocument14 pagesColorectal Cancer StagingRonnie Alexander Reyes MartínezNo ratings yet
- Pembrolizumab in MSI-H DMMR Advanced Colorectal Cancer A New Standard of CareDocument3 pagesPembrolizumab in MSI-H DMMR Advanced Colorectal Cancer A New Standard of CareasdffdsaNo ratings yet
- Colon Cancer Research Paper OutlineDocument7 pagesColon Cancer Research Paper Outlineafnhcikzzncojo100% (1)
- Research Article CBG AT1Document10 pagesResearch Article CBG AT1Scarlet-Jean BrettNo ratings yet
- Ganguly 2021Document1 pageGanguly 2021Kamila MuyasarahNo ratings yet
- 1 s2.0 S003130251640365X MainDocument9 pages1 s2.0 S003130251640365X MainbrendaNo ratings yet
- Risk of Uterine Cancer For BRCA1 and BRCA2 Mutation CarriersDocument7 pagesRisk of Uterine Cancer For BRCA1 and BRCA2 Mutation CarriersShahzeen Sajid KhanNo ratings yet
- Zaghloul 2017Document9 pagesZaghloul 2017Mauricio MerancioNo ratings yet
- Brca Mast Vs ConservadoraDocument20 pagesBrca Mast Vs ConservadoraVictoria DuqueNo ratings yet
- Neoadjuvant ChemotherapyDocument42 pagesNeoadjuvant ChemotherapyHala FekryNo ratings yet
- MEK Inhibitors in Combination With Immune Checkpoint Inhibition: Should We Be Chasing Colorectal Cancer or The KRAS Mutant CancerDocument2 pagesMEK Inhibitors in Combination With Immune Checkpoint Inhibition: Should We Be Chasing Colorectal Cancer or The KRAS Mutant CancerPeertechz Publications Inc.No ratings yet
- Breast Cancer ChemotherapyDocument7 pagesBreast Cancer Chemotherapydini kusmaharaniNo ratings yet
- Jamaoncology Vinayak 2019 Oi 190028Document9 pagesJamaoncology Vinayak 2019 Oi 190028Noema AmorochoNo ratings yet
- BCTN ChekpointsDocument7 pagesBCTN ChekpointsJESUS EDGAR GONZALES AYASTANo ratings yet
- RG Radiologists' Role in Breast Cancer StagingDocument14 pagesRG Radiologists' Role in Breast Cancer StagingAzucena BCNo ratings yet
- Atchley Et Al 2016 Clinical and Pathologic Characteristics of PatientsDocument7 pagesAtchley Et Al 2016 Clinical and Pathologic Characteristics of PatientsWojtek JanotaNo ratings yet
- Session 538 PDFDocument34 pagesSession 538 PDFMed MedNo ratings yet
- Radiotherapy Treatment Planning: Objectives, Formulations and Clinical ImplicationsDocument32 pagesRadiotherapy Treatment Planning: Objectives, Formulations and Clinical ImplicationsMed MedNo ratings yet
- Ijcem0008 16808 PDFDocument5 pagesIjcem0008 16808 PDFMed MedNo ratings yet
- Brfo193 Radiotherapy Dose Fractionation Third-Edition PDFDocument137 pagesBrfo193 Radiotherapy Dose Fractionation Third-Edition PDFMed MedNo ratings yet
- Piis0140673620309326 PDFDocument14 pagesPiis0140673620309326 PDFMed MedNo ratings yet
- Pe09055 PDFDocument5 pagesPe09055 PDFMed MedNo ratings yet
- 0225 PDFDocument47 pages0225 PDFMed MedNo ratings yet
- Din 2013Document5 pagesDin 2013Med MedNo ratings yet
- Jack2010 PDFDocument3 pagesJack2010 PDFMed MedNo ratings yet
- IESEducationalresources PDFDocument4 pagesIESEducationalresources PDFMed MedNo ratings yet
- JCB Art 30512-10 PDFDocument7 pagesJCB Art 30512-10 PDFMed MedNo ratings yet
- Nejmoa 1112088Document11 pagesNejmoa 1112088Med MedNo ratings yet
- Irrad 0812 FinalDocument9 pagesIrrad 0812 FinalMed MedNo ratings yet
- 2-22-13 Lecture PDFDocument9 pages2-22-13 Lecture PDFMed MedNo ratings yet
- Lactic Acid Training For Fat Loss - T NationDocument4 pagesLactic Acid Training For Fat Loss - T NationMed MedNo ratings yet
- Sarcomas of Soft Tissue: Brian A. Van TineDocument50 pagesSarcomas of Soft Tissue: Brian A. Van TineMed MedNo ratings yet
- Bonesarcomasand Desmoids: Jeremy M. Brownstein,, Thomas F. DelaneyDocument12 pagesBonesarcomasand Desmoids: Jeremy M. Brownstein,, Thomas F. DelaneyMed MedNo ratings yet
- PMRT TNBCDocument8 pagesPMRT TNBCMed MedNo ratings yet
- Osg Catalogue March 2021Document72 pagesOsg Catalogue March 2021Ritvik KhuranaNo ratings yet
- Native Mitral Valve Fungal Endocarditis Caused 2024 International Journal ofDocument4 pagesNative Mitral Valve Fungal Endocarditis Caused 2024 International Journal ofRonald QuezadaNo ratings yet
- Animal Caries ModelsDocument11 pagesAnimal Caries ModelscharitoupchNo ratings yet
- SPM Essay Pandemic Covid-19Document4 pagesSPM Essay Pandemic Covid-19nguyentranthaoan10No ratings yet
- Tacrolimus Ointment Is Used To Treat The Symptoms of EczemaDocument2 pagesTacrolimus Ointment Is Used To Treat The Symptoms of EczemaSharan SahotaNo ratings yet
- Synopsis 20052012Document6 pagesSynopsis 20052012Ajay VinodiaNo ratings yet
- Thorax Drain: Dr. Ririek Parwitasari, SPPDocument13 pagesThorax Drain: Dr. Ririek Parwitasari, SPPrianiNo ratings yet
- The Spine FrequenciesDocument2 pagesThe Spine Frequencieschris adiNo ratings yet
- St. Michael's College: Nursing Care Plan FormDocument3 pagesSt. Michael's College: Nursing Care Plan Formacademic purposesNo ratings yet
- Presentation On Bone DiseaseDocument52 pagesPresentation On Bone DiseaseNoor-E-Khadiza ShamaNo ratings yet
- NSTPDocument11 pagesNSTPCASTRO, JHONLY ROEL C.No ratings yet
- Astrocyte: Structure & FunctionDocument7 pagesAstrocyte: Structure & Functionمحمود الموسويNo ratings yet
- Basal Insulin Versus Premixed Insulin For The Treatment of T2DmDocument98 pagesBasal Insulin Versus Premixed Insulin For The Treatment of T2DmMaya SwariNo ratings yet
- Microcirculation Monitoring - LOCAL GhalebDocument46 pagesMicrocirculation Monitoring - LOCAL GhalebGHALEB A. AlmekhlafiNo ratings yet
- Husbandry Guidelines: Dromaius NovaehollandiaeDocument126 pagesHusbandry Guidelines: Dromaius NovaehollandiaeCitra MaharaniNo ratings yet
- Vitrectomy For Endophthalmitis: 5-Year Study of Outcomes and ComplicationsDocument8 pagesVitrectomy For Endophthalmitis: 5-Year Study of Outcomes and ComplicationsqisthiNo ratings yet
- CHN Rle Pointers and Review NotesDocument6 pagesCHN Rle Pointers and Review NotesKeziah Marie Chua Santa-AnaNo ratings yet
- Handout E4N Unit 1Document4 pagesHandout E4N Unit 1Ratu Aldi NingrumNo ratings yet
- Seven Sirtuins For Seven Deadly Diseases of Aging: Free Radical Biology and Medicine October 2012Document40 pagesSeven Sirtuins For Seven Deadly Diseases of Aging: Free Radical Biology and Medicine October 2012mr dexterNo ratings yet
- 1339-Article Text-24955-2-10-20220330Document6 pages1339-Article Text-24955-2-10-20220330Kevean Kimi LimNo ratings yet
- Manfaat Rendaman Air Hangat Dan Garam Dalam Menurunkan Derajat Edema Kaki Ibu Hamil Trimester IiiDocument6 pagesManfaat Rendaman Air Hangat Dan Garam Dalam Menurunkan Derajat Edema Kaki Ibu Hamil Trimester IiiShinta BalikpapanNo ratings yet
- COVID-19 - Informative EssayDocument1 pageCOVID-19 - Informative EssayRydl Pnp100% (1)
- Clsi H18 A3 PDFDocument52 pagesClsi H18 A3 PDFyandros666100% (2)
- The Different Perspectives of DisasterDocument3 pagesThe Different Perspectives of DisasterJuliane Rebecca PitlongayNo ratings yet
- Almc Part - 2 Ayurvedic Lifestyle ManagementDocument101 pagesAlmc Part - 2 Ayurvedic Lifestyle ManagementUdhayNo ratings yet
- Parental Consent and Waiver Form: Bogo Central School IiDocument2 pagesParental Consent and Waiver Form: Bogo Central School IiMhërvžž CatarataNo ratings yet
- Unit:-3: Presented By: - Deepak Chandra JoshiDocument24 pagesUnit:-3: Presented By: - Deepak Chandra JoshiRahul PalsNo ratings yet
- Kerala State Palliative Care Policy 2019Document24 pagesKerala State Palliative Care Policy 2019ASIF ALI MHNo ratings yet
- Cover Dan AbstrakDocument3 pagesCover Dan AbstrakAndhika DipaNo ratings yet
- Treatment: Chapter 67: TuberculosisDocument3 pagesTreatment: Chapter 67: TuberculosisNina MarlinaNo ratings yet