You might also like
- NANOTECHNOLOGY REVIEW: LIPOSOMES, NANOTUBES & PLGA NANOPARTICLESFrom EverandNANOTECHNOLOGY REVIEW: LIPOSOMES, NANOTUBES & PLGA NANOPARTICLESNo ratings yet
- Hemostasis in Neurosurgery OnlineDocument26 pagesHemostasis in Neurosurgery OnlinekushalNo ratings yet
- Tonicity Calculations An Aid To UnderstandingDocument6 pagesTonicity Calculations An Aid To UnderstandingMuhammad MakkiNo ratings yet
- 1 M840-GalleyProofDocument8 pages1 M840-GalleyProofAna GNo ratings yet
- Hyadent English PDFDocument13 pagesHyadent English PDFSilviu TipleaNo ratings yet
- Alginates As HaemostaticDocument3 pagesAlginates As HaemostaticAgdaOliveiraNo ratings yet
- Cap 158 COSMETIC SURGERYDocument24 pagesCap 158 COSMETIC SURGERYalexxa_1900No ratings yet
- Topicalhemostatic Agents: What The Oral and Maxillofacial Surgeon Needs To KnowDocument10 pagesTopicalhemostatic Agents: What The Oral and Maxillofacial Surgeon Needs To KnowAB MISHRANo ratings yet
- AmbioDisk InformationDocument2 pagesAmbioDisk Informationnurani atikasariNo ratings yet
- Afa 2Document15 pagesAfa 2Ariana ReligiosoNo ratings yet
- Haemostatic AgentsDocument3 pagesHaemostatic Agentsmeenalairan100% (1)
- Facial Burns and Theresienöl®Document9 pagesFacial Burns and Theresienöl®Sabrina JonesNo ratings yet
- 1 s2.0 S0141813024010997 MainDocument16 pages1 s2.0 S0141813024010997 MainasyaroesNo ratings yet
- Hydrophilic Polymers With Potassium Salt and Microporous Polysaccharides For Use As Hemostatic AgentsDocument4 pagesHydrophilic Polymers With Potassium Salt and Microporous Polysaccharides For Use As Hemostatic AgentsAriana ReligiosoNo ratings yet
- A Narrative Review of Different Hemostatic Materials inDocument8 pagesA Narrative Review of Different Hemostatic Materials inhamza najmNo ratings yet
- Dermatological Pharmacology: Topical Agents: Key PointsDocument3 pagesDermatological Pharmacology: Topical Agents: Key PointsIsmail IbrahimNo ratings yet
- The Evaluation of Resorbable Haemostatic Wound DressingsDocument15 pagesThe Evaluation of Resorbable Haemostatic Wound DressingsPavan KumarNo ratings yet
- AmnioMatrix - IntegraDocument2 pagesAmnioMatrix - IntegraZhou WeiJieNo ratings yet
- An Absorbable and Soluble Haemostatic Gauze - Bloodstop: Clinical Trial #2Document7 pagesAn Absorbable and Soluble Haemostatic Gauze - Bloodstop: Clinical Trial #2Angelina RicardoNo ratings yet
- Rhinology 2002 p185Document4 pagesRhinology 2002 p185Rettha SigiroNo ratings yet
- Pressure Ulcers and Hydrocolloids Made EasyDocument6 pagesPressure Ulcers and Hydrocolloids Made EasyJefferson AlexandreNo ratings yet
- An Approach To Structural Facial Rejuvenation With Fillers in WomenDocument15 pagesAn Approach To Structural Facial Rejuvenation With Fillers in WomenJhon RodriguezNo ratings yet
- Topical Hemostatic Agents in Neurosurgery 2011Document35 pagesTopical Hemostatic Agents in Neurosurgery 2011Ardhynata SetiawanNo ratings yet
- Company and Soft Tissue Regeneration ProductsDocument51 pagesCompany and Soft Tissue Regeneration ProductsPaulus LagadanNo ratings yet
- Cicatrização de Feridas Dérmicas Propriedade Do Óleo de Caryocar Brasiliense Carregado (TRADUZIR)Document9 pagesCicatrização de Feridas Dérmicas Propriedade Do Óleo de Caryocar Brasiliense Carregado (TRADUZIR)Igor Ferrari StreitNo ratings yet
- Biomaterials For Hemostasis 2022Document29 pagesBiomaterials For Hemostasis 2022gv941022No ratings yet
- Actinic Cheratosis - A ReviewDocument4 pagesActinic Cheratosis - A ReviewMARIUS-MIRCEA POPESCU-MICLOSANUNo ratings yet
- Dentistry 10 00076 v2Document13 pagesDentistry 10 00076 v2Dev DeviNo ratings yet
- Rusun Hemostatic Product Introduction 0625Document33 pagesRusun Hemostatic Product Introduction 0625Calvin hobbesNo ratings yet
- Dermal Filler 4Document59 pagesDermal Filler 4Ahmed Sad100% (1)
- Review Hemostatic DressingsDocument21 pagesReview Hemostatic DressingsJean CotteNo ratings yet
- Autologous Serum Eye Drops For Ocular Surface Disorders: PerspectiveDocument8 pagesAutologous Serum Eye Drops For Ocular Surface Disorders: PerspectiveBramantya Surya PratamaNo ratings yet
- Putting Injectable Facial Fillers To Their Best Use PDFDocument4 pagesPutting Injectable Facial Fillers To Their Best Use PDFvini_tbNo ratings yet
- ACTOLINDDocument34 pagesACTOLINDmishkat100% (1)
- Styptics KMCDDocument23 pagesStyptics KMCDBishal ChauhanNo ratings yet
- v10 Treatment of Viral Warts With Intralesional BleomycinDocument5 pagesv10 Treatment of Viral Warts With Intralesional BleomycinAlisNo ratings yet
- Haneke-2006-Journal of Cosmetic DermatologyDocument11 pagesHaneke-2006-Journal of Cosmetic DermatologyGuillermo RomeroNo ratings yet
- Prevention of Alveolar Osteitis: A Case Report and Review of LiteratureDocument5 pagesPrevention of Alveolar Osteitis: A Case Report and Review of Literaturechandra auliaNo ratings yet
- Practical Guide To Joint and Soft Tissue Injection TechniquesDocument5 pagesPractical Guide To Joint and Soft Tissue Injection TechniquesHerry HendrayadiNo ratings yet
- Amnion Membrane Hydrogel and Amnion Membrane Powder Accelerate Wound Healing in A Full Thickness Porcine Skin Wound ModelDocument13 pagesAmnion Membrane Hydrogel and Amnion Membrane Powder Accelerate Wound Healing in A Full Thickness Porcine Skin Wound ModelselcanekicierNo ratings yet
- Investigating Wound Healing Potential of Typha Angustata L. InflorescenceDocument10 pagesInvestigating Wound Healing Potential of Typha Angustata L. Inflorescenceyasir aliNo ratings yet
- Formulation and Evaluation of Nail Lacquer Containing Anti Fungal Griseofulvin For The Treatment of OnychomycosisDocument13 pagesFormulation and Evaluation of Nail Lacquer Containing Anti Fungal Griseofulvin For The Treatment of OnychomycosisInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Development and Evaluations of Transdermal Delivery of Selegiline HydrochlorideDocument14 pagesDevelopment and Evaluations of Transdermal Delivery of Selegiline HydrochlorideInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- An Overview of Permanent and Semipermanent Fillers: SummaryDocument8 pagesAn Overview of Permanent and Semipermanent Fillers: SummaryArmin ArceoNo ratings yet
- Biopad BiosprayDocument24 pagesBiopad BiosprayLuci ContiuNo ratings yet
- Adhesives March 2012Document54 pagesAdhesives March 2012Eduardo Leal Salgado100% (1)
- Intracanal Medicaments: Presented By: DR - Suruchi Sisodia Dept. of Conservative Dentistry and EndodonticsDocument106 pagesIntracanal Medicaments: Presented By: DR - Suruchi Sisodia Dept. of Conservative Dentistry and Endodonticsrasagna reddy100% (1)
- Nanoemulsions and Topical Creams For The Safe and Effective Delivery of Lipophilic Antioxidant Coenzyme Q10Document11 pagesNanoemulsions and Topical Creams For The Safe and Effective Delivery of Lipophilic Antioxidant Coenzyme Q10Sandy NCNo ratings yet
- 1 s2.0 0378517396046492 Main PDFDocument15 pages1 s2.0 0378517396046492 Main PDFNatalia FabriNo ratings yet
- Wound-Healing Effects of Human Dermal Components With Gelatin DressingDocument10 pagesWound-Healing Effects of Human Dermal Components With Gelatin Dressingsasibhushanarao poolaNo ratings yet
- Transdermal Drug DeliveryDocument38 pagesTransdermal Drug DeliveryJhansi SattiNo ratings yet
- DressingsDocument16 pagesDressingsJose VergaraNo ratings yet
- Preparation of Human Amniotic Membrane For Transplantation in Different Application AreasDocument18 pagesPreparation of Human Amniotic Membrane For Transplantation in Different Application AreasselcanekicierNo ratings yet
- Polymers 03 00509 v2Document18 pagesPolymers 03 00509 v2Branko BabicNo ratings yet
- Dental Implant As Novel Drug Delivery SystemDocument26 pagesDental Implant As Novel Drug Delivery SystemRajesh KumarNo ratings yet
- Formulation and Evaluation of Transdermal Patch of Diclofenac SodiumDocument4 pagesFormulation and Evaluation of Transdermal Patch of Diclofenac SodiumM Dwiyan RilandiNo ratings yet
- Applications of Biomaterials in Plastic SurgeryDocument18 pagesApplications of Biomaterials in Plastic SurgeryacanahuateNo ratings yet
- Functional Bio-based Materials for Regenerative Medicine: From Bench to Bedside (Part 1)From EverandFunctional Bio-based Materials for Regenerative Medicine: From Bench to Bedside (Part 1)No ratings yet
- Airbus A350-900 Lufthansa New LiveryDocument17 pagesAirbus A350-900 Lufthansa New LiveryfelipeNo ratings yet
- Lufthansa A340-600 D-AIHI PDFDocument19 pagesLufthansa A340-600 D-AIHI PDFandres Pabon50% (2)
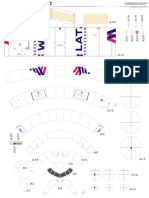
- Boeing 777-300ER Latam PDFDocument18 pagesBoeing 777-300ER Latam PDFandres PabonNo ratings yet
- Boeing 777-300ER United Old Livery PDFDocument18 pagesBoeing 777-300ER United Old Livery PDFandres PabonNo ratings yet
- Boeing 777-300ER Latam PDFDocument18 pagesBoeing 777-300ER Latam PDFandres PabonNo ratings yet
- Preparation of Highly Substituted Carboxymethyl Starch Using A Twin-Screw ExtruderDocument9 pagesPreparation of Highly Substituted Carboxymethyl Starch Using A Twin-Screw Extruderandres PabonNo ratings yet
- Individual CounselingDocument7 pagesIndividual CounselingCarla Dela CruzNo ratings yet
- AishwaryaDocument52 pagesAishwaryamohitNo ratings yet
- Abc Ven 2020Document81 pagesAbc Ven 2020CorneLia JacintaNo ratings yet
- Normative Data For A Spanish Version of The Rey Auditory-Verbal Learning Test in Older PeopleDocument12 pagesNormative Data For A Spanish Version of The Rey Auditory-Verbal Learning Test in Older PeopleeastareaNo ratings yet
- Book StickerDocument4 pagesBook Stickerilanabiela90No ratings yet
- PE and Health 1 Midterm Exam - My Fitness JourneyDocument4 pagesPE and Health 1 Midterm Exam - My Fitness JourneyCedrik AustriaNo ratings yet
- Cardiovascular DiseaseDocument6 pagesCardiovascular Diseasedandana149No ratings yet
- WBC DisordersDocument45 pagesWBC DisordersyalahopaNo ratings yet
- The Miracle of ChocolateDocument10 pagesThe Miracle of ChocolateAmanda YasminNo ratings yet
- Stress and Parents of Children With Autism: A Review of LiteratureDocument12 pagesStress and Parents of Children With Autism: A Review of Literatureana lara SantosNo ratings yet
- 12 2012 TriclabendazoleDocument16 pages12 2012 Triclabendazolenia suwartiningsihNo ratings yet
- Hypo - RT PC TrialDocument37 pagesHypo - RT PC TrialnitinNo ratings yet
- Becas Taiwan ICDFDocument54 pagesBecas Taiwan ICDFlloco11No ratings yet
- Hand in Hand For A Healthier World: Logiq V5 ExpertDocument4 pagesHand in Hand For A Healthier World: Logiq V5 ExpertPablo RamirezNo ratings yet
- Health 10: 3 Quarter Week 7Document10 pagesHealth 10: 3 Quarter Week 7Maria Rose Tariga Aquino50% (2)
- Annual Report of NHRC (2016-17)Document240 pagesAnnual Report of NHRC (2016-17)Shruti Nagvanshi100% (1)
- 2022 Arihant Political Science MCQs Term-1 Sample PapersDocument192 pages2022 Arihant Political Science MCQs Term-1 Sample PapersImran Arshad100% (4)
- English Conversation Discussion About AllergiesDocument3 pagesEnglish Conversation Discussion About AllergiesKevin ScottNo ratings yet
- Social Work MaterialDocument214 pagesSocial Work MaterialBala Tvn100% (2)
- AICTE CorporateBestPracticesDocument13 pagesAICTE CorporateBestPracticesramar MNo ratings yet
- Stanford CWLP HandbookDocument60 pagesStanford CWLP HandbookDon DoehlaNo ratings yet
- Senior Thesis - Corry ArcomanoDocument21 pagesSenior Thesis - Corry Arcomanoapi-407563053No ratings yet
- Nail Psoriasis Treatment Options and Management.99846Document20 pagesNail Psoriasis Treatment Options and Management.99846yuliNo ratings yet
- D-Ox Benefits of Hydrogen WaterDocument10 pagesD-Ox Benefits of Hydrogen WaterGabi Del RosarioNo ratings yet
- HUL275 Environment Development and Society Assignment 2 Victims and SurvivorsDocument3 pagesHUL275 Environment Development and Society Assignment 2 Victims and SurvivorsSachin BatwaniNo ratings yet
- Behaviorism in Daily LifeDocument8 pagesBehaviorism in Daily LifeMichelleTongNo ratings yet
- De La Cruz, Et Al. (2015) Treatment of Children With ADHD and IrritabilityDocument12 pagesDe La Cruz, Et Al. (2015) Treatment of Children With ADHD and Irritabilityjuan100% (1)
- CSR Activities by TATADocument13 pagesCSR Activities by TATAMegha VaruNo ratings yet
- Annual Leave Policy of University of YorkDocument15 pagesAnnual Leave Policy of University of YorkJohn Son100% (1)
- Fever Nursing Care PlanDocument3 pagesFever Nursing Care PlanMarie Anne T85% (39)