You might also like
- An OMERACT Reliability Exercise of in Ammatory and Structural Abnormalities in Patients With Knee Osteoarthritis Using Ultrasound AssessmentDocument5 pagesAn OMERACT Reliability Exercise of in Ammatory and Structural Abnormalities in Patients With Knee Osteoarthritis Using Ultrasound AssessmentArkar SoeNo ratings yet
- Annrheumdis 2014 206774supp Table1Document1 pageAnnrheumdis 2014 206774supp Table1Arkar SoeNo ratings yet
- PIIS106345849890200XDocument7 pagesPIIS106345849890200XArkar SoeNo ratings yet
- OMERACT Patient Remission - Scientific SummaryDocument7 pagesOMERACT Patient Remission - Scientific SummaryArkar SoeNo ratings yet
- OMERACT Patient Remission - Lay SummaryDocument2 pagesOMERACT Patient Remission - Lay SummaryArkar SoeNo ratings yet
- Non-Arthroplasty Treatment of Osteoarthritis of The Knee: AAOS Appropriate Use Criteria SummaryDocument5 pagesNon-Arthroplasty Treatment of Osteoarthritis of The Knee: AAOS Appropriate Use Criteria SummaryArkar SoeNo ratings yet
- RSSCDocument9 pagesRSSCDanish KhanNo ratings yet
- The Kappa Statistic in Reliability Studies: Use, Interpretation, and Sample Size RequirementsDocument12 pagesThe Kappa Statistic in Reliability Studies: Use, Interpretation, and Sample Size RequirementsArkar SoeNo ratings yet
- 3 s2.0 B9781416055341500020Document1 page3 s2.0 B9781416055341500020Arkar SoeNo ratings yet
- All Rights Reserved. No Part of This Publication May Be Reproduced or Transmitted in Any Form or by AnyDocument1 pageAll Rights Reserved. No Part of This Publication May Be Reproduced or Transmitted in Any Form or by AnyArkar SoeNo ratings yet
- A Note On The Linearly Weighted Kappa Coefficient For Ordinal ScalesDocument13 pagesA Note On The Linearly Weighted Kappa Coefficient For Ordinal ScalesArkar SoeNo ratings yet
- Calculating Agreement Correctly Writing: Percentage But Formula IncorrectlyDocument2 pagesCalculating Agreement Correctly Writing: Percentage But Formula IncorrectlyArkar SoeNo ratings yet
- Statistical Methodology: Matthijs J. WarrensDocument5 pagesStatistical Methodology: Matthijs J. WarrensArkar SoeNo ratings yet
- 10 1 1 572 1639Document17 pages10 1 1 572 1639Arkar SoeNo ratings yet
- Measurement Educational and PsychologicalDocument8 pagesMeasurement Educational and PsychologicalNico Pascual IIINo ratings yet
- Jmu 26 194Document6 pagesJmu 26 194Arkar SoeNo ratings yet
- Hoffa's Fat Pad: Evaluation On Unenhanced MR Images As A Measure of Patellofemoral Synovitis in OsteoarthritisDocument5 pagesHoffa's Fat Pad: Evaluation On Unenhanced MR Images As A Measure of Patellofemoral Synovitis in OsteoarthritisArkar SoeNo ratings yet
- Reliability and Validity of Ultrasound Imaging of Features of Knee Osteoarthritis in The CommunityDocument8 pagesReliability and Validity of Ultrasound Imaging of Features of Knee Osteoarthritis in The CommunityCaitlynNo ratings yet
- Assessing Small Study Effects and Publication Bias in Orthodontic Meta-Analyses: A Meta-Epidemiological StudyDocument14 pagesAssessing Small Study Effects and Publication Bias in Orthodontic Meta-Analyses: A Meta-Epidemiological StudyArkar SoeNo ratings yet
- Bmri2018 7469197Document7 pagesBmri2018 7469197Arkar SoeNo ratings yet
- Clinimetrics of Ultrasound Pathologies in Osteoarthritis: Systematic Literature Review and Meta-AnalysisDocument11 pagesClinimetrics of Ultrasound Pathologies in Osteoarthritis: Systematic Literature Review and Meta-AnalysisArkar SoeNo ratings yet
- New LOGIQ e DatasheetDocument10 pagesNew LOGIQ e Datasheetbashir019No ratings yet
- Chung and ChengDocument10 pagesChung and ChengArkar SoeNo ratings yet
- Safari - 19 Sep 2018 at 4:46 PM PDFDocument1 pageSafari - 19 Sep 2018 at 4:46 PM PDFArkar SoeNo ratings yet
- NIH Public Access: Author ManuscriptDocument31 pagesNIH Public Access: Author ManuscriptArkar SoeNo ratings yet
- Electrical Stimulation in The Management of Spasticity: A ReviewDocument5 pagesElectrical Stimulation in The Management of Spasticity: A ReviewArkar SoeNo ratings yet
- Neurorehabilitation and Neural RepairDocument5 pagesNeurorehabilitation and Neural RepairArkar SoeNo ratings yet
- Transcutaneous Electrical Nerve Stimulation Versus Baclofen in SpasticityDocument9 pagesTranscutaneous Electrical Nerve Stimulation Versus Baclofen in SpasticityArkar SoeNo ratings yet
- Al Gabbani PDFDocument107 pagesAl Gabbani PDFArkar SoeNo ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (120)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Kauwe 2017Document15 pagesKauwe 2017Nurfitrianti ArfahNo ratings yet
- QLD TheraSuit Info KitDocument6 pagesQLD TheraSuit Info Kitrevcruz100% (2)
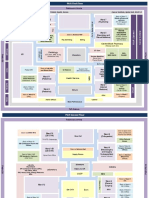
- Topic 3-Health Service Delivery NetworkDocument30 pagesTopic 3-Health Service Delivery NetworkPooja SaravananNo ratings yet
- JCI Reference Guide WRDocument55 pagesJCI Reference Guide WRSanjeev Chougule100% (1)
- Annex - X Rehab ServicesDocument19 pagesAnnex - X Rehab ServicesHema SahuNo ratings yet
- PGH MapDocument2 pagesPGH MapAlyssandra LucenoNo ratings yet
- Cerebral Palsy - Critical Elements of CareDocument25 pagesCerebral Palsy - Critical Elements of CaremarkoNo ratings yet
- TLE BookletDocument4 pagesTLE BookletJulluis DagoNo ratings yet
- Yoga Therapy Info Packet 2.7.21Document40 pagesYoga Therapy Info Packet 2.7.21Nostalgia2340% (1)
- Nursing Care Plan For AppendectomyDocument5 pagesNursing Care Plan For Appendectomyvanessajane0989% (45)
- Rehab U LowbackfixDocument11 pagesRehab U LowbackfixRoberto Barrón100% (5)
- Health10 LM U4Document40 pagesHealth10 LM U4Maureen Pusing100% (2)
- 5HW047 - Holistic Approaches To Healthcare - Assignment LayoutDocument15 pages5HW047 - Holistic Approaches To Healthcare - Assignment LayoutVicky RobiNo ratings yet
- Lisa 2016Document8 pagesLisa 2016druketo vndmatNo ratings yet
- EPI NCSC Course HandbookDocument19 pagesEPI NCSC Course HandbookKarlNo ratings yet
- Jamda: Original StudyDocument8 pagesJamda: Original StudyAndy Delos ReyesNo ratings yet
- UG Curriculum Vol II PDFDocument247 pagesUG Curriculum Vol II PDFRavi Meher67% (3)
- H Clinical Assessment ToolsDocument71 pagesH Clinical Assessment ToolsPaijo SusenoNo ratings yet
- Tree Coding ExamplesDocument6 pagesTree Coding ExampleswecameasromansNo ratings yet
- 9 Safe Nursing Indicators - Safe Staffing For Nursing in Adult Inpatient Wards in Acute Hospitals - Guidance - NICEDocument12 pages9 Safe Nursing Indicators - Safe Staffing For Nursing in Adult Inpatient Wards in Acute Hospitals - Guidance - NICEmiftakhul jannahNo ratings yet
- ConferenceDocument6 pagesConferenceMitali SharmaNo ratings yet
- DGM (SA) Portfolio 24 11 2020 PDFDocument48 pagesDGM (SA) Portfolio 24 11 2020 PDFMitchell GowNo ratings yet
- PTJ CasereportguidelinesDocument16 pagesPTJ CasereportguidelinesC MNo ratings yet
- Julia Dito ResumeDocument3 pagesJulia Dito Resumeapi-253713289No ratings yet
- Jenna Fulks Self DesignedDocument8 pagesJenna Fulks Self Designedapi-299452232No ratings yet
- Dental Health Care at The Disabled Children's Rehabilitation Center in RiyadhDocument5 pagesDental Health Care at The Disabled Children's Rehabilitation Center in RiyadhSaravanan ThangarajanNo ratings yet
- Sample OT Reports Adult AllDocument22 pagesSample OT Reports Adult AllDanielle Stella N'Luca50% (2)
- 2019 Physical Therapy in Adult Inflammmatory Myopathy Patients A Systematic ReviewDocument13 pages2019 Physical Therapy in Adult Inflammmatory Myopathy Patients A Systematic ReviewAngelica OvandoNo ratings yet
- Principles of Cancer RehabDocument15 pagesPrinciples of Cancer RehabnoonoonsNo ratings yet
- Cdu PT Case Presentation de Quervain'sDocument15 pagesCdu PT Case Presentation de Quervain'sKatrina San RamonNo ratings yet