You might also like
- Clinical Cases in Heart FailureFrom EverandClinical Cases in Heart FailureRavi V. ShahNo ratings yet
- Acute Heart Failure and Cardiogenic Shock - 3a A Multidisciplinary Practical GuidanceDocument17 pagesAcute Heart Failure and Cardiogenic Shock - 3a A Multidisciplinary Practical GuidanceAaron Nureña100% (1)
- HF in ElderlyDocument3 pagesHF in ElderlyHadi M.WNo ratings yet
- Control of Hypertension in The Critically Ill: A Pathophysiological ApproachDocument13 pagesControl of Hypertension in The Critically Ill: A Pathophysiological Approachjose torresNo ratings yet
- Acute Heart Failure in Elderly Patients: A Review of Invasive and Non-Invasive ManagementDocument17 pagesAcute Heart Failure in Elderly Patients: A Review of Invasive and Non-Invasive ManagementErika A. Rodriguez JaureguiNo ratings yet
- Crisis HypertensionDocument2 pagesCrisis HypertensionDinar DewiNo ratings yet
- Previous Sectionnext SectionDocument19 pagesPrevious Sectionnext Sectionbaiq_permataNo ratings yet
- Effect of Implementing Clinical Pathway Guidelines On Patients' Clinical Outcomes With Acute Coronary SyndromeDocument17 pagesEffect of Implementing Clinical Pathway Guidelines On Patients' Clinical Outcomes With Acute Coronary SyndromenurulfahmiNo ratings yet
- ADHF ManagementDocument6 pagesADHF ManagementEsti YunitaNo ratings yet
- Vasopressors in ShockDocument8 pagesVasopressors in ShockOrion JohnNo ratings yet
- Transplant IndicationsDocument9 pagesTransplant IndicationsvamshidhNo ratings yet
- European J of Heart Fail - 2010 - Gheorghiade - Assessing and Grading Congestion in Acute Heart Failure A ScientificDocument11 pagesEuropean J of Heart Fail - 2010 - Gheorghiade - Assessing and Grading Congestion in Acute Heart Failure A ScientificVlad RusuNo ratings yet
- Trends in Cardiovascular Medicine: Lauren Sinnenberg, Michael M. GivertzDocument9 pagesTrends in Cardiovascular Medicine: Lauren Sinnenberg, Michael M. GivertzJulio PorrasNo ratings yet
- Cardiovascular Medicine Journals4Document6 pagesCardiovascular Medicine Journals4Praveen GundetiNo ratings yet
- From Acute Heart Failure To Cardiogenic Shock Patients Requiring Admission, 2023Document2 pagesFrom Acute Heart Failure To Cardiogenic Shock Patients Requiring Admission, 2023Jonathan Fierro MedinaNo ratings yet
- TX Iskemik StrokeDocument17 pagesTX Iskemik StrokeNailis Sa'adahNo ratings yet
- Resistant HypertensionDocument11 pagesResistant Hypertensionansel7No ratings yet
- Resistant HypertensionDocument12 pagesResistant Hypertensionsury listinNo ratings yet
- Biomedicines 10 02407 v2Document13 pagesBiomedicines 10 02407 v2akinaNo ratings yet
- JGC 15 07 504 PDFDocument9 pagesJGC 15 07 504 PDFZuhalJanuarNo ratings yet
- Acute Congestive Heart Failure in The Emergency DepartmentDocument9 pagesAcute Congestive Heart Failure in The Emergency DepartmentAlanNo ratings yet
- Biomarker-Based Preoperative Risk Stratification For Patients Undergoing Non-Cardiac Surgery - Yurttas Et Al 2020Document10 pagesBiomarker-Based Preoperative Risk Stratification For Patients Undergoing Non-Cardiac Surgery - Yurttas Et Al 2020santosfer1102No ratings yet
- Acute Heart FailureDocument24 pagesAcute Heart FailureTeddy MauriceNo ratings yet
- Prognostic Significance of Diastolic Dysfunction With Multiple Comorbidities in Heart Failure PatientsDocument11 pagesPrognostic Significance of Diastolic Dysfunction With Multiple Comorbidities in Heart Failure PatientsDefriyan RamziNo ratings yet
- 3390-Article Text-1555-3802-10-20200606Document12 pages3390-Article Text-1555-3802-10-20200606Mayara Bongestab ParteliNo ratings yet
- Advances Management ADHFDocument14 pagesAdvances Management ADHFAnonymous NeRC5JYiSNo ratings yet
- Decompensated Heart Failure: Insuficiência Cardíaca DescompensadaDocument9 pagesDecompensated Heart Failure: Insuficiência Cardíaca DescompensadakunkkonkNo ratings yet
- Ten Questions ICU Specialists Should Address When Managing Cardiogenic Acute Pulmonary OedemaDocument4 pagesTen Questions ICU Specialists Should Address When Managing Cardiogenic Acute Pulmonary OedemaFarmacia Del Bosque100% (1)
- International Journal of Scientific Research: General MedicineDocument4 pagesInternational Journal of Scientific Research: General MedicineTriple ANo ratings yet
- Intracerebral Hemorrhage Medical TreatmentDocument3 pagesIntracerebral Hemorrhage Medical TreatmentDarrel Allan MandiasNo ratings yet
- Ac HF2 PDFDocument6 pagesAc HF2 PDFKocsis IldikoNo ratings yet
- Ehv 066Document9 pagesEhv 066Sidik SyafaatullahNo ratings yet
- JCVTR 11 79Document6 pagesJCVTR 11 79triNo ratings yet
- Perioperative management of patients with coronary artery disease undergoing non cardiac surgery summary of the french society of anaesthesia and intensive care medicine 2017 convention AnestCriCarePainMed 2017Document8 pagesPerioperative management of patients with coronary artery disease undergoing non cardiac surgery summary of the french society of anaesthesia and intensive care medicine 2017 convention AnestCriCarePainMed 2017RicardoNo ratings yet
- Pregunta Del EstudioDocument7 pagesPregunta Del EstudioMarco RodriguezNo ratings yet
- 10.1007@s11906 020 01120 7Document11 pages10.1007@s11906 020 01120 7ivenasabillaNo ratings yet
- Expert Statement For Management Hypovolemia in Sepsis PDFDocument8 pagesExpert Statement For Management Hypovolemia in Sepsis PDFRobi HeryantoNo ratings yet
- DCV PDFDocument25 pagesDCV PDFLeyDi CamposanoNo ratings yet
- Ejhf 2206Document10 pagesEjhf 2206Luis Fernando Morales JuradoNo ratings yet
- FarmakoekonomiDocument11 pagesFarmakoekonomiAbran HadiqNo ratings yet
- SA Hypertension GuidelinesDocument26 pagesSA Hypertension GuidelinesMaleehaNo ratings yet
- Initial Assessment and Management of Acute StrokeDocument41 pagesInitial Assessment and Management of Acute StrokeandresNo ratings yet
- Ejhf 2206Document10 pagesEjhf 2206khangha.ptNo ratings yet
- Initial Assessment and Management of Acute Stroke - UpToDateDocument27 pagesInitial Assessment and Management of Acute Stroke - UpToDateDiego VillacisNo ratings yet
- Insuficiencia Cardiaca e Sind CoraçãoDocument13 pagesInsuficiencia Cardiaca e Sind CoraçãofulvioschiavoNo ratings yet
- Criteria For Surgical Intervention Should Not Be IgnoredDocument9 pagesCriteria For Surgical Intervention Should Not Be IgnoredJorge Álvarez GómezNo ratings yet
- Maloberti 2018Document13 pagesMaloberti 2018Aishah FarihaNo ratings yet
- Heart Failure and Atrial Fibrillation: New Concepts in Pathophysiology, Management, and Future DirectionsDocument10 pagesHeart Failure and Atrial Fibrillation: New Concepts in Pathophysiology, Management, and Future Directionsdr_antonio81No ratings yet
- Ircmj 17 06 20705 PDFDocument7 pagesIrcmj 17 06 20705 PDFUchi SuhermanNo ratings yet
- Ischemicstroke: Advances in Diagnosis and ManagementDocument20 pagesIschemicstroke: Advances in Diagnosis and ManagementPatty MArivel ReinosoNo ratings yet
- Predictive Value of High-Sensitivity Troponin-I For Future Adverse Cardiovascular Outcome in Stable Patients With Type 2 Diabetes MellitusDocument8 pagesPredictive Value of High-Sensitivity Troponin-I For Future Adverse Cardiovascular Outcome in Stable Patients With Type 2 Diabetes MellitusRooban SivakumarNo ratings yet
- Acute Decompensated Heart FailureDocument22 pagesAcute Decompensated Heart Failurediomer123No ratings yet
- Order ID 3416232.edited - EditedDocument5 pagesOrder ID 3416232.edited - Editedngunyijohn001No ratings yet
- Sepsis With Preexisting Heart Failure: Management of Confounding Clinical FeaturesDocument24 pagesSepsis With Preexisting Heart Failure: Management of Confounding Clinical FeaturesKarla HernandezNo ratings yet
- NHAM Heart FailureDocument46 pagesNHAM Heart FailureMei DreeNo ratings yet
- Albumin in aSAH NeuroCrit2023Document11 pagesAlbumin in aSAH NeuroCrit2023Ahida VelazquezNo ratings yet
- Ehad 617Document16 pagesEhad 617Fabi CancholaNo ratings yet
- Oral Heart Failure Medications: An Update For Home Health CliniciansDocument12 pagesOral Heart Failure Medications: An Update For Home Health CliniciansSaraTravassosNo ratings yet
- Tatalaksana GUCH Di ICUDocument12 pagesTatalaksana GUCH Di ICUBima AryaputraNo ratings yet
- Altered Ketones and HFDocument13 pagesAltered Ketones and HFAnonymous NeRC5JYiSNo ratings yet
- Biomarkers in HFDocument17 pagesBiomarkers in HFAnonymous NeRC5JYiSNo ratings yet
- ADHF in HFpEFDocument9 pagesADHF in HFpEFAnonymous NeRC5JYiSNo ratings yet
- Advances Management ADHFDocument14 pagesAdvances Management ADHFAnonymous NeRC5JYiSNo ratings yet
- Acute Kidney Injury in HFDocument14 pagesAcute Kidney Injury in HFAnonymous NeRC5JYiSNo ratings yet
- Clinical Assessment in Acute Heart Failure: Review ArticleDocument17 pagesClinical Assessment in Acute Heart Failure: Review ArticleAnonymous NeRC5JYiSNo ratings yet
- ESC Guidelines On Cardio-Oncology - 2022Document133 pagesESC Guidelines On Cardio-Oncology - 2022nicolasNo ratings yet
- Altered Hemodynamics and End-Organ in HFDocument15 pagesAltered Hemodynamics and End-Organ in HFAnonymous NeRC5JYiSNo ratings yet
- A Randomized Controlled Trial CCMDocument10 pagesA Randomized Controlled Trial CCMAnonymous NeRC5JYiSNo ratings yet
- Target Dose Vs Target HRDocument3 pagesTarget Dose Vs Target HRAnonymous NeRC5JYiSNo ratings yet
- ADHF HFrEFDocument14 pagesADHF HFrEFAnonymous NeRC5JYiSNo ratings yet
- BB AND CCBDocument16 pagesBB AND CCBAnonymous NeRC5JYiSNo ratings yet
- Smoking and CHDDocument19 pagesSmoking and CHDAnonymous NeRC5JYiSNo ratings yet
- Atrial Fibrilasi Dan HF - MekanismeDocument10 pagesAtrial Fibrilasi Dan HF - MekanismeAnonymous NeRC5JYiSNo ratings yet
- Age and Atrial FibrilasiDocument8 pagesAge and Atrial FibrilasiAnonymous NeRC5JYiSNo ratings yet
- Age Risk Factors Heart FailureDocument9 pagesAge Risk Factors Heart FailureAnonymous NeRC5JYiSNo ratings yet
- Ehx493 P5438Document1 pageEhx493 P5438Anonymous NeRC5JYiSNo ratings yet
- SARS COV2 Vaccination and MyocarditisDocument9 pagesSARS COV2 Vaccination and MyocarditisMicaela Belen LuccardiNo ratings yet
- Proposed Diagnostic Brugada SyndromeDocument7 pagesProposed Diagnostic Brugada SyndromecyelzNo ratings yet
- ASCOT Hypertension StudyDocument12 pagesASCOT Hypertension StudyAnonymous NeRC5JYiSNo ratings yet
- Calcium Channel Blockers Report PDFDocument43 pagesCalcium Channel Blockers Report PDFElyza XeNo ratings yet
- Calcium Channel Blockers inDocument15 pagesCalcium Channel Blockers inAnonymous NeRC5JYiSNo ratings yet
- ACS Management and ESC GuidelinesDocument56 pagesACS Management and ESC GuidelinesAnonymous NeRC5JYiSNo ratings yet
- RHDDocument130 pagesRHDDeepu RajendranNo ratings yet
- Pathogenic Mechanisms in Rheumatic Carditis Focus On Valvular EndotheliumDocument5 pagesPathogenic Mechanisms in Rheumatic Carditis Focus On Valvular EndotheliumAnonymous NeRC5JYiSNo ratings yet
- ACLS Rhythms For The ACLS Algorithms: AppendixDocument32 pagesACLS Rhythms For The ACLS Algorithms: Appendixyan_ricci19100% (4)
- Prospect TrialDocument37 pagesProspect TrialAnonymous NeRC5JYiSNo ratings yet
- Acls Algorithms Rapid RatesDocument8 pagesAcls Algorithms Rapid RatesAnonymous NeRC5JYiSNo ratings yet
- Echo Presentation - Endocrine Nefro HematoDocument27 pagesEcho Presentation - Endocrine Nefro HematoAnonymous NeRC5JYiSNo ratings yet
- Anticholinergic Pocket CardDocument2 pagesAnticholinergic Pocket Cardtrompito53No ratings yet
- Gambling Addiction SpeechDocument6 pagesGambling Addiction Speechapi-239318658No ratings yet
- Psychoeducation An Effective Tool As Treatment Modality in Mental HealthDocument9 pagesPsychoeducation An Effective Tool As Treatment Modality in Mental HealthAbu SumayyahNo ratings yet
- Heart Failure Case StudyDocument2 pagesHeart Failure Case StudyRC0% (1)
- Antiemetics and ProkineticsDocument29 pagesAntiemetics and ProkineticsGilbert Girising100% (1)
- Measuring Intake and OutputDocument1 pageMeasuring Intake and OutputCJ AngelesNo ratings yet
- International Journal of Health Sciences and ResearchDocument30 pagesInternational Journal of Health Sciences and ResearchNurul RiskiNo ratings yet
- Clinical Trials BudgetingDocument52 pagesClinical Trials Budgetingjlbabson100% (5)
- Co-Processing of Afr in Euro Cement Industry Cembureau 2009Document16 pagesCo-Processing of Afr in Euro Cement Industry Cembureau 2009Ibnuyusoff77No ratings yet
- Percutaneous Nephrolithotomy - WikipediaDocument7 pagesPercutaneous Nephrolithotomy - WikipediaZaheer UllahNo ratings yet
- Quiz - QuizizzDocument1 pageQuiz - Quizizzapi-384598186No ratings yet
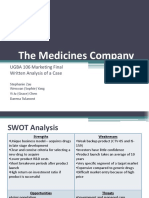
- The Medicines Company Presentation Final OriginalDocument24 pagesThe Medicines Company Presentation Final OriginalVinay100% (1)
- Palliative CarefinalDocument13 pagesPalliative CarefinalPutri Senna RahayuNo ratings yet
- Trauma-Sensitive Mindfulness: Practices For Safe and Transformative Healing - David A. TreleavenDocument5 pagesTrauma-Sensitive Mindfulness: Practices For Safe and Transformative Healing - David A. Treleavenryxeduzo0% (1)
- Ethics and Standards of Practice For Massage TherapistsDocument8 pagesEthics and Standards of Practice For Massage Therapistsapi-243836925No ratings yet
- 9990 - m23 - Ms - 42 ProvDocument17 pages9990 - m23 - Ms - 42 ProvPurpleMyself25No ratings yet
- Exenatide PDFDocument3 pagesExenatide PDFHam SotheaNo ratings yet
- Psychoanalytic Therapy in The Borderline Neuroses - Stern, Adolph - The Psychoanalytic Quarterly, #2, 14, Pages 190-198, 1945Document10 pagesPsychoanalytic Therapy in The Borderline Neuroses - Stern, Adolph - The Psychoanalytic Quarterly, #2, 14, Pages 190-198, 1945NESFHIS UFSCNo ratings yet
- Maternal Health Nursing - 50 Item Without RatioDocument3 pagesMaternal Health Nursing - 50 Item Without RatioDennis Nabor Muñoz, RN,RMNo ratings yet
- Asthma Control Test EnglishDocument1 pageAsthma Control Test Englishkhangsiean89No ratings yet
- Maternity Questions and AnswerDocument5 pagesMaternity Questions and AnswerLovaine WilliamsNo ratings yet
- Treatment in Canine Epilepsy - A Systematic ReviewDocument24 pagesTreatment in Canine Epilepsy - A Systematic ReviewGarcia y Rivera AbogadosNo ratings yet
- Care Plan Data CollectionDocument14 pagesCare Plan Data CollectionmayraNo ratings yet
- Pediatric CapdDocument7 pagesPediatric CapdsagaNo ratings yet
- Healing WonderDocument31 pagesHealing WonderRussiel DagohoyNo ratings yet
- Acute Intestinal ObstructionDocument38 pagesAcute Intestinal ObstructiondinahzrNo ratings yet
- Paediatric Percutaneous Nephrolithotomy (P-PCNL) Reporting ChecklistDocument6 pagesPaediatric Percutaneous Nephrolithotomy (P-PCNL) Reporting ChecklistJad DegheiliNo ratings yet
- Ketamine SpecialistguidelinesonuseDocument12 pagesKetamine SpecialistguidelinesonuseDeboraNainggolanNo ratings yet
- Caldorol (Ibuprofen IV)Document14 pagesCaldorol (Ibuprofen IV)Agus SusantoNo ratings yet
- 2.spondilitis TBDocument27 pages2.spondilitis TBMega MuzdalifahNo ratings yet