You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5808)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (843)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (346)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- History of TandoorDocument3 pagesHistory of Tandoorpiyush100% (2)
- SsangYong Actyon Sports Q149 2011.01 Electrical Wiring DiagramDocument84 pagesSsangYong Actyon Sports Q149 2011.01 Electrical Wiring Diagramcelyoz100% (1)
- Top 25 Food Ideas For Baby Led Weaning: VegetablesDocument1 pageTop 25 Food Ideas For Baby Led Weaning: Vegetablesbecca wiseNo ratings yet
- Reading Questions - Science and BeautyDocument3 pagesReading Questions - Science and BeautyEllen Lam100% (1)
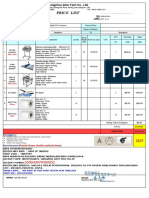
- Price List: With StandDocument1 pagePrice List: With StandAlex TajoNo ratings yet
- The Waves of The Technological InnovationsDocument17 pagesThe Waves of The Technological InnovationsRio AwitinNo ratings yet
- XH260L - XH260V: Dixell Operating InstructionsDocument4 pagesXH260L - XH260V: Dixell Operating InstructionsJennifer Eszter SárközyNo ratings yet
- Download full chapter The First Institutional Spheres In Human Societies Evolutionary Analysis In The Social Sciences 1St Edition Abrutyn pdf docxDocument54 pagesDownload full chapter The First Institutional Spheres In Human Societies Evolutionary Analysis In The Social Sciences 1St Edition Abrutyn pdf docxmarcus.stassinos948No ratings yet
- Use of Stainless Steel CrownsDocument16 pagesUse of Stainless Steel CrownsKaren De la GarzaNo ratings yet
- H BridgeDocument41 pagesH BridgeSheikh IsmailNo ratings yet
- HDES-D0165 General Tolerance in Dimension (Eng)Document1 pageHDES-D0165 General Tolerance in Dimension (Eng)juniorferrari06No ratings yet
- Gear Hobbing Shaping and Shaving A Guide To Cycle Time Estimating and Process Planning PDFDocument183 pagesGear Hobbing Shaping and Shaving A Guide To Cycle Time Estimating and Process Planning PDFvenkat100% (2)
- Vision Document (Template)Document5 pagesVision Document (Template)Andrew MacAulayNo ratings yet
- E SHB 2009 - Vav3Document169 pagesE SHB 2009 - Vav3ictgisNo ratings yet
- Summer Training Finance Project On WORKING CAPITAL MANAGEMENTDocument82 pagesSummer Training Finance Project On WORKING CAPITAL MANAGEMENTPravin chavda100% (2)
- Apxv9r20b C A20 PDFDocument2 pagesApxv9r20b C A20 PDFКонстантин ПетровNo ratings yet
- 8902 LS (Parker)Document20 pages8902 LS (Parker)abdohalim248No ratings yet
- Carbohydrates: MonosaccharidesDocument8 pagesCarbohydrates: MonosaccharidesLily NemphisNo ratings yet
- Non-Mendelian InheritanceDocument12 pagesNon-Mendelian InheritanceBillones Rebalde MarnelleNo ratings yet
- Soal PTS B Inggris 5Document8 pagesSoal PTS B Inggris 5Hasna NurlailiNo ratings yet
- Teens 2 - Resource PackDocument14 pagesTeens 2 - Resource PackGigliane SouzaNo ratings yet
- ArthritisDocument5 pagesArthritismeenuNo ratings yet
- Microprocessor 4th SemDocument316 pagesMicroprocessor 4th SemDaggupatiHarishNo ratings yet
- Critical ResultDocument2 pagesCritical ResultSUSANTONo ratings yet
- Pasler Dufourt PNM2011Document34 pagesPasler Dufourt PNM2011balintkNo ratings yet
- Kode Icd 10Document38 pagesKode Icd 10interna squardNo ratings yet
- Introduction To Biopotential Measurement and Excitation: (Bioelectromagnetism - Jakko Malmivuo, Robert Plonsey)Document23 pagesIntroduction To Biopotential Measurement and Excitation: (Bioelectromagnetism - Jakko Malmivuo, Robert Plonsey)Lynn WankharNo ratings yet
- Redox Reactions: Neet /jee QuestionsDocument27 pagesRedox Reactions: Neet /jee QuestionsAsher LaurierNo ratings yet
- Kothari Sugar Factory Internshipproject SamoleDocument52 pagesKothari Sugar Factory Internshipproject Samolenoobwarrior3No ratings yet
- Identification Tables For Common Minerals in Thin SectionDocument4 pagesIdentification Tables For Common Minerals in Thin SectionTanmay KeluskarNo ratings yet