Professional Documents
Culture Documents
Clinical Practice Guidelines PDF
Clinical Practice Guidelines PDF
Uploaded by
Yerni KarnitaOriginal Title
Copyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
Clinical Practice Guidelines PDF
Clinical Practice Guidelines PDF
Uploaded by
Yerni KarnitaCopyright:
Available Formats
Clinical practice guidelines:
non-Hodgkin's lymphomas
R I C H A R D I. FISHER, MD, A N D M A R T I N M. O K E N , M D
BACKGROUND Despite the common clonal origin of the non-Hodgkin's lymphomas (NHLs), their char-
acteristic diversity contributes to the difficulty of defining comprehensive treatment regimens.
To review and compare historical and current data that define practice guidelines in the
treatment of the NHLs.
»^aiava Early-stage, low-grade NHLs: Irradiation remains the standard treatment. Late-stage, low-
grade NHLs and advanced-stage indolent lymphomas: Alkylating agents (eg, chlorambucil, cyclophos-
phamide) are the standard response, although recent studies suggest maintaining a vigilant,
watch-and-wait course anticipatory of intervention. Some new therapies, alone or in combination,
offer potential for development (eg, the chemotherapeutic agents fludarabine, 2'-deoxycoformycin,
and 2-chlorodeoxyadenosine for low-grade NHLs, and bone marrow transplantation, monoclonal
antibodies, and recombinant interferon-alfa for advanced-stage indolent lymphomas). Intermediate-
grade aggressive and high-grade NHLs: Combination chemotherapy (ie, C H O P ) is the historical treat-
ment, plus regional irradiation, with C N S prophylaxis an additional option in high-grade
lymphoblastic disease, and bone marrow transplantation an additional option in large-cell immuno-
blastic and small noncleaved-cell NHLs.
CONCLUSIONS Presently accepted therapies remain the mainstays in treating the NHLs; however, pro-
gressive therapeutic regimens, such as watching and waiting for intermediate-level disease progres-
sion or employing salvage, high-dose chemotherapeutic regimens, often with bone marrow
transplantation, in intermediate- or high-grade disease stages, have yielded measurable successes in
significant minorities of patients.
INDEX TERMS: LYMPHOMA, NON-HODGKIN'S; ANTINEOPLASTIC AGENTS
CLEVE CLIN J MED 1995; 62:SH-48
From the Division of Hematology/Oncology, Loyola University Medical Center (R.I.F.) and the Virginia Piper Cancer
Institute, Abbott Northwestern Hospital (M.M.O.).
Address reprint requests to R.I.F., Division of Hematology/Oncology, Loyola University Medical Center, 2160 S. First
Avenue, Building 54, Suite 067A, Maywood, IL 60153-5500.
SI-6 CLEVELAND CLINIC JOURNAL OF MEDICINE VOLUME 62 • SUPPLEMENT I
NON-HODGKIIM'S LYMPHOMAS • FISHER AND OKEN
HE NON-HODGKIN'S LYMPHOMAS consti- ries, their origin involves a common theme: they
T tute a diverse group of malignancies of the
lymphoid system, c o l l e c t i v e l y repre-
senting approximately 4% of all cancer
deaths in the United States. 1 T h e incidence of non-
Hodgkin's lymphomas has been increasing during
represent a clonal malignant expansion of lympho-
cytes that appear to be arrested at a specific stage of
normal lymphocytic differentiation. 3 T h e precise
etiology of the non-Hodgkin's lymphomas is un-
known, despite considerable advances in under-
the past two decades, and it has been estimated that standing the biology of this disorder during the past
approximately 51 000 new cases will be diagnosed decade.
and 23 000 deaths will occur during 1995. 1 T h e me- A viral origin is suspected and, indeed, it has
dian age for presentation is 42 years, and the inci- been shown that adult T-cell lymphoma has a viral
dence increases with advancing age. 2 T h e majority etiology. Moreover, Epstein-Barr virus has been
(75%) 2 of non-Hodgkin's lymphomas are of B-cell convincingly related to the etiology of African
origin, although exceptions exist, such as Sézary's Burkitt's lymphoma and to posttransplant lym-
syndrome, mycosis fungoides, adult T-cell leuke- phomas, as well as to some lymphomas arising in
mia/lymphoma, and many cases of lymphoblastic patients with acquired immunodeficiency syn-
lymphoma, which are diseases of T-cell origin. Al- drome ( A I D S ) .
though the non-Hodgkin's lymphomas are diverse T h e clinical behavior of most non-Hodgkin's
in their responses to therapy and their natural histo- lymphomas may be broadly categorized into two
ABBREVIATIONS
ACOP-B: low-dose doxorubicin, cyclophosphamide, GELA: Multicenter Cooperative Groupe d'Etude des Lym-
vincristine, prednisone, and bleomycin phomes de I'AduSte
ABMT: autologous bone marrow transplant Gy: gray
ADA: adenosine deaminase HIV: human immunodeficiency virus
AIDS: acquired immunodeficiency syndrome HLA: human lymphocyte antigen
ara-C: cytosine arabinoside (cytarabine) HTLV-I: human T-cell leukemia/lymphoma type I
BACOP: bleomycin, doxorubicin, cyclophosphamide, l-COPA: cyclophosphamide, doxorubicin, vincristine, pred-
vincristine, and prednisone nisone, and rHulFN-a
bcl-2: B-cell leukemia/lymphoma rHulFN-a: recombinant human interferon alfa
CALGB: Cancer and Leukemia Group B rHulFN-a2a: recombinant human interferon alfa-2a
2-CdA: 2-chlorodeoxyadenosine (cladribine) rHulFN-a2b: recombinant human interferon alfa-2b
CD8 cells: mature T-suppressor/cytotoxic cells rHulFN-an1: highly purified blend of natural human inter-
CD10: common acute lymphoblastic leukemia antigen ferons
(CALLA) LDH: lactic dehydrogenase
CD34 cells: mature T-helper cells MACOP-B: methotrexate with leucovorin rescue, doxoru-
CHOP: cyclophosphamide, doxorubicin, vincristine, and bicin, cyclophosphamide, vincristine, prednisone, and
prednisone bleomycin
CHOP-Bleo: cyclophosphamide, doxorubicin, vincristine, MALTomas: rnucosa-associated /ymphoid tissue lymphomas
prednisone and bleomycin m-BACOD: methotrexate with leucovorin rescue, bleomy-
CHVP: cyclophosphamide, doxorubicin, teniposide, and cin, doxorubicin, cyclophosphamide, vincristine, and dex-
prednisone amethasone,
CLL: chronic lymphocytic leukemia MU: million units
C-MOPP: cyclophosphamide, vincristine, procarbazine, and PCA: polyclonal antibody
prednisone PR: partial response
CNS: central nervous system ProMACE-CytaBOM: prednisone, methotrexate, doxoru-
COMLA: cyclophosphamide, vincristine, methotrexate with bicin, cyclophosphamide, and etoposide, followed by
leucovorin rescue, and ara-C cytarabine, bleomycin, vincristine, and methotrexate
COPA: cyclophosphamide, doxorubicin, vincristine, and with leucovorin rescue
prednisone ProMACE-MOPP: prednisone, methotrexate, doxorubicin,
CR: complete response cyclophosphamide, and etoposide alternating with nitro-
CTi computed tomography gen mustard, vincristine, procarbazine, and prednisone
CTCL: cutaneous T-cell lymphoma SWOG: Southwest Oncology Group
CVP: cyclophosphamide, vincristine, and prednisone VABE: etoposide, doxorubicin, vincristine, prednisone, and
DCF: 2'-deoxycoformycin (pentostatin) bleomycin
DHAP: dexamethasone, high-dose ara-C, and cisplatin VMP: etoposide, mitoxantrone, and prednimustine
ECOG: Eastern Cooperative Oncology Group Working Formulation: National Cancer Institute's Work-
F-ara-ATP: fluoro-arabinofuranosyl-adenosine triphosphate ing Formulation of Non-Hodgkin's Lymphomas for Clini-
2-F-ara-A: 2-fluoro-arabinofuranosyl-adenine cal Usage
VOLUME 62 • SUPPLEMENT I CLEVELAND CLINIC JOURNAL OF MEDICINES I - 37
NON-HODGKIN'S LYMPHOMAS • FISHER AND OKEN
TABLE 1
CLASSIFICATION OF NON-HODGKIN'S LYMPHOMAS
Working Formulation Rappaport classification
Low-grade
Malignant lymphoma, small lymphocytic consistent Diffuse well-differentiated lymphocytic (DWDL)
with chronic lymphocytic leukemia
Malignant lymphoma, follicular predominantly small cleaved cell Nodular poorly differentiated lymphocytic (NPDL)
Malignant lymphoma, follicular mixed, small cleaved and large cell Nodular mixed lymphocytic-histiocytic (NH)
Intermediate-grac/e
Malignant lymphoma, follicular predominantly large cell Nodular histiocytic (NH)
Malignant lymphoma, diffuse small cleaved cell Diffuse poorly differentiated lymphocytic (DPDL)
Malignant lymphoma, diffuse mixed, small and large cell Diffuse mixed lymphocytic-histiocytic (DM)
Malignant lymphoma, diffuse large cell Diffuse histiocytic (DH)
High-grade
Malignant lymphoma, large cell, immunoblastic Diffuse histiocytic (DH)
Malignant lymphoma, lymphoblastic Diffuse lymphoblastic (LL)
Malignant lymphoma, small nondeaved cell Diffuse undifferentiated (DU)
"Adapted from Gaynor and Fisher, reference 3, with permission
groups: the favorable, indolent lymphomas and the subtypes (low, intermediate, and high grades) and
unfavorable, aggressive lymphomas. T h e former categorizes them according to natural history and
group has a longer natural history, with patients potential response to therapy. Despite the consis-
enduring slowly progressive disease over a span of tency provided by the Working Formulation, the
many years. This category of non-Hodgkin's lym- classification of this disease remains imperfect, as is
phoma, which is not usually curable, includes dif- reflected by the fact that several "new" subgroups of
fuse well-differentiated lymphocytic lymphoma, non-Hodgkin's lymphoma have been identified
nodular mixed, and nodular poorly differentiated that do not fit well into the Working Formulation.
lymphocytic lymphomas. O n the other hand, the These include, for example, low-grade lymphomas
unfavorable or aggressive lymphomas tend quickly such as monocytoid B-cell lymphoma 8 ; low- and
to progress to death in the absence of therapy. intermediate-grade lymphomas such as mantle zone
Treatments have recently been developed that can lymphomas 9 ; intermediate- and high-grade lym-
provide long-term (disease-free) survival for many phomas such as anaplastic large-cell lymphoma 1 0 ;
of these patients. T h e unfavorable, aggressive non- and the cutaneous T-cell lymphomas ( C T C L s ) ,
Hodgkin's lymphomas include nodular histiocytic, mycosis fungoides, and Sezary's syndrome. 11
diffuse mixed, diffuse histiocytic, diffuse undifferen- During the past decade, considerable progress
tiated, and diffuse poorly differentiated lympho- has been made in our understanding of the biologic
cytic lymphomas. basis and approach to treatment of non-Hodgkin's
S e v e r a l h i s t o l o g i c c l a s s i f i c a t i o n s of n o n - lymphomas. This diverse group of malignant lym-
Hodgkin's lymphoma 4 " 6 have been widely used dur- phomas exhibits distinctive natural histories and
ing the past several decades. However, this has re- responses to t r e a t m e n t . In general, the non-
sulted in confusion about the diagnosis of the Hodgkin's lymphomas are responsive to treatment,
d i s e a s e . T h e W o r k i n g F o r m u l a t i o n of N o n - although the extent and duration of the responses
Hodgkin's Lymphomas for Clinical Usage 7 ( t h e may vary considerably. It is of great importance to
Working Formulation) was developed in order to establish a correct histologic diagnosis in order to
permit a meaningful correlation among the princi- assure that the most appropriate therapeutic plan is
pal histologic classifications of non-Hodgkin's lym- offered to each individual patient. General treat-
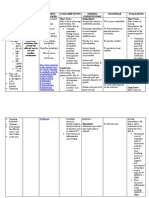
phoma (Table 1). T h e Working Formulation organ- ment options are schematically represented in the
izes the non-Hodgkin's lymphomas into three Figure.
SI-8 CLEVELAND CLINIC JOURNAL OF MEDICINE VOLUME 62 • SUPPLEMENT I
NON-HODGKIIM'S LYMPHOMAS • FISHER A N D OKEN
Diagnosis of non-Hodgkin's lymphoma confirmed
Low grade Intermediate grade High grade
I
Stage I or II Stage III or IV Stage I or II Stage II, bulky Lymphoblastic Small non-
Stage III or IV cleaved cell
Burkitt's
Radiation Cyclophosphamide,
doxorubicin,
vincristine, and
prednisone (CHOP) Combination Combination
± radiation chemotherapy chemotherapy
+ central nervous
system prophylaxis
Asymptomatic Symptomatic ± radiation
(no significant anemia, (significant anemia,
thrombocytopenia, or thrombocytopenia,
splenomegaly) splenomegaly)
Watch and wait Combination chemotherapy
± recombinant human
interferon alfa
vs
Single alkylating agent
± corticosteroid
F I G U R E . Schematic representation of general treatment options for non-Hodgkin's lymphoma. See also Table 6.
P A T H O P H Y S I O L O G Y OF N O N - H O D G K I N ' S To suitably accomplish the process of immune
LYMPHOMAS
recognition, antigen receptor genes (immuno-
globulin and T-cell receptor genes) must undergo
Cytogenetic and molecular genetic analyses of rearrangement of their D N A prior to encoding key
malignant lymphocytes provide strong experimental proteins. Such rearrangement has been described in
evidence for the clonal origin of human lymphoid detail. 26 Rearrangement of immunoglobulin genes is
neoplasms.12"23 Clonal expansion of B cells or T cells generally restricted to cells of the B-cell lineage,
in the non-Hodgkin's lymphomas refers to a situ- whereas gene rearrangement in T cells involves a
ation in which, presumably, a single cell has under- different set of genes, namely those encoding T-cell
gone malignant transformation, giving rise to a antigen receptors. 27 The genomic structure of the
clone of identical B or T cells. The progeny com- T-cell antigen receptor genes is very similar to that
monly recapitulate the functional and phenotypic of the immunoglobulin genes. Accordingly, T-cell
characteristics of the normal B or T cell at the receptor genes undergo rearrangement through
corresponding stage of development. Because the joining of V-J or V-D-J segments during early T-cell
rearrangement of antigen receptor genes takes place differentiation, thereby providing great diversity of
early during the differentiation of B or T lympho- antigen recognition by the T cell. The immuno-
cytes, rearrangements of one or more antigen recep- globulin gene rearrangements may serve as unique
tor genes are found in almost all human lymphoid clonal markers21 in human lymphoid neoplasms be-
neoplasms.19"25 cause, as a clonal expansion, an individual tumor
VOLUME 62 • SUPPLEMENT I CLEVELAND CLINIC JOURNAL OF MEDICINESI-37
NON-HODGKIN'S LYMPHOMAS • FISHER AND OKEN
contains the identically rearranged gene through- the non-Hodgkin's lymphomas is the 14; 18 translo-
out the cell population. Moreover, a gene rear- cation t(14;18), which was first reported in 1979 by
rangement discovered in a lymphoid cell popula- Fukuhara et al,34 who detected this translocation in
tion not only indicates clonality but in most six of nine patients with a diagnosis of poorly differ-
situations may also provide a lineage marker.23 In entiated lymphocytic lymphoma. T h e 14;18
order to detect such gene rearrangements, D N A is translocation is most common in the follicular lym-
extracted from tissue samples such as peripheral phomas, although it may be seen in multiple his-
blood, bone marrow aspirates and biopsies, and tologic subtypes of non-Hodgkin's lymphoma. This
lymph node biopsies. The D N A is cut 15 with a translocation results in the rearrangement of a
restriction endonuclease that identifies recognition proto-oncogene, bcl-2 (B-cell leukemia/lym-
sites that flank a selected part of the gene believed phoma), normally located on chromosome 18, with
to have undergone rearrangement. The D N A that the immunoglobulin heavy chain region on chro-
has been cut with the restriction enzyme and hy- mosome 14. In the study of Yunis et al, 12 the
bridized with selected probes will show altered re- t(14;18) translocation was detected in 60 of the 71
striction fragment sizes if rearrangement has oc- B-cell lymphoma patients (85%) studied. Among
curred. Rearrangements of immunoglobulin genes these patients, 37 were diagnosed with follicular
can be demonstrated using Southern blot analysis small cleaved-cell, 17 with follicular mixed-cell, and
in virtually all B-cell malignancies. 21,28 17 with follicular large-cell lymphoma. The 60 cases
During the past two decades, multiple studies of translocation included all 37 of the patients with
have established that most human lymphoid neo- follicular small cleaved-cell lymphoma. In that
plasms are associated with characteristic chromoso- group, 10 patients presented with t(14;18) as a sin-
mal abnormalities. 12,29-31 A s mentioned above, the gle chromosomal defect and experienced an indo-
chromosomal abnormalities detected in non- lent disease course, with eight of 10 patients not
Hodgkin's lymphoma have a clonal origin; there- requiring any treatment for 1 to 4 years after diagno-
fore, the initial chromosomal variation takes place sis. Those patients who did not exhibit a single
in a single cell, with subsequent cells carrying the chromosomal defect generally had from two to nine
identical variation. Such variations are thus so- chromosomal defects. More than 70% of all the
matic mutations in lymphoma patients with an chromosomal defects detected in patients from this
otherwise normal karyotype. Clearly, non- and the authors' preceding studies30'31 were found to
Hodgkin's lymphoma is a genetic disease. Rowley 14 be recurrent. These defects included 14 distinct
cites several landmark contributions that have nonrandom chromosomal duplications and dele-
paved the way for our understanding of the genetics tions. Most of these 14 defects correlated with a
of non-Hodgkin's lymphoma. These include the specific histopathology, poor prognosis, or leukemic
identification of extra chromosomal material on blood picture, or a combination of these features.
chromosome 14 (14q+) from patients with Burkitt's The authors proposed a model for the general evolu-
lymphoma, 32 the determination that the 14q+ was a tion of follicular lymphomas carrying the 14; 18
result of translocation 33 between chromosomes 8 translocation. The model provides a suggested cor-
and 14, identification of the 14; 18 translocation, 34 relation between histopathology, chromosomal de-
cloning of the translocation breakpoint junction fects, and clinical aggressiveness of the disease. The
from Burkitt's lymphoma, 35,36 and cloning of the bcl-2 oncogene rearrangement was confirmed in
t(14;18) junction. 37 These contributions made it specimens from patients with follicular small
possible to compare multiple characteristics of the cleaved-cell, mixed-cell, and large-cell lymphoma, 12
non-Hodgkin's lymphomas, such as karyotype, his- suggesting that the translocation with accompany-
tology, immunophenotype, and, more recently, ing oncogene rearrangement may be a crucial re-
D N A markers. In combination with data correlat- quirement for the follicular process.
ing these characteristics with the clinical response
Ngan et al17 further demonstrated the consistent
to treatment, it has become possible to demonstrate
expression of a proto-oncogenic protein, bcl-2, in a
that different chromosomal profiles are associated
large proportion of non-Hodgkin's lymphomas and
with different natural histories and overall survival
proposed that t(14;18) translocations might have as
times in the non-Hodgkin's lymphomas. 38
a common consequence the overexpression of the
The most common chromosomal abnormality in bcl-2 protein product. T h e y raised antibodies
SI-10 CLEVELAND CLINIC JOURNAL OF MEDICINE VOLUME 62 • SUPPLEMENT I
NON-HODGKIIM'S LYMPHOMAS • FISHER AND OKEN
against the bcl-2 gene protein product that were myc oncogene. 36 In Burkitt's lymphoma, the most
shown to specifically recognize a human protein common translocation, t(8;14), involves the c-myc
whose presence correlated with transcription of the gene undergoing translocation from its normal loca-
bcl'2 gene. They used the antibodies to demonstrate tion on chromosome 8 to the immunoglobulin
that the bcl-2 protein is expressed in a substantial heavy chain locus on the long arm of chromosome
proportion of non-Hodgkin's lymphomas at levels 14. By contrast, in the other translocations cited
sufficiently high to permit detection by frozen-sec- above (t[2;8] and t[8;22]), an immunoglobulin light
tion immunohistochemistry. The bcl-2 protein was chain locus becomes adjacent to c-myc. It is believed
not detected in all of the malignant lymphomas that such rearrangements expose the c-myc proto-
studied, nor was it found in normal or reactive lym- oncogene to the influence of regulatory sequences in
phoid tissue; expression of the bcl-2 protein was or near the immunoglobulin locus. This event
most commonly associated with non-Hodgkin's might, in turn, deregulate expression of the myc
lymphomas exhibiting the t(14;18) translocation. gene and contribute to potentiation of B-cell neo-
Conversely, a small number of lymphomas lacking plasia. Finally, other translocations involving chro-
evidence of the t(14;18) translocation did express mosome 14 are encountered in human lymphoid
the bcl-2 protein at comparable levels to those asso- neoplasms, 39 such as the t( 11; 14) chromosome
ciated with cells bearing the translocation. It is pos- translocation, which is seen in mantle zone lym-
sible that such neoplasms did actually contain phomas. In such instances, the breakpoint on chro-
t(14;18) translocations with breakpoints outside the mosome 14 occurs in the region carrying the heavy
regions detected by the D N A probes employed. chain locus. Tsujimoto et al39 studied diffuse large-
Also, the expression of bcl-2 was most prevalent in cell lymphomas and chronic lymphocytic leukemia
follicular lymphomas, with measurable bcl-2 protein (CLL) cells of the B-cell type carrying the t ( l l ; 1 4 )
found in virtually all the small cleaved-cell follicular translocation in order to clone the chromosomal
tumors. By contrast, a lesser proportion of follicular breakpoint to obtain nucleic acid probes that would
large-cell tumors expressed measurable bcl-2 pro- permit identification of a putative oncogene that
tein. This is not surprising because a substantially might be activated by translocation to the heavy
lower percentage of follicular large-cell neoplasms chain locus. This gene, named bcl-1, appears to
exhibit the t(14;18) translocation. 16 By preventing have a role in the malignant transformation of hu-
apoptosis or programmed cell death, overproduction man B-cells exhibiting the t( 11; 14) translocation.
of the bcl-2 gene protein product plays a role in
In general terms, the non-Hodgkin's lymphomas
perpetuation of the cancerous cell clone.
constitute a diverse group of diseases involving
The t(14;18) chromosomal translocation is by no clonal expansions of B or T lymphocytes arrested at a
means the only rearrangement of great significance specific stage of cell maturation. Although the mo-
in human lymphoid neoplasia. Chromosomal re- lecular mechanisms underlying these events are not
arrangements involving translocation to the termi- clearly understood, the chromosomal translocations
nal regions of the long arm of chromosome 14 have cited above appear to confer a neoplastic prolifera-
been detected in a variety of tumors with involve- tive advantage in the non-Hodgkin's lymphomas.
ment of chromosomes 8, 11, or 18 as "donor" chro- During the past decade, our understanding of the
mosomes. 15 One of the most thoroughly charac- immunophenotypes of the normal cells of the im-
terized groups of chromosomal abnormalities comes mune system has increased. Lymphocytes may be
from patients with Burkitt's lymphoma. Cytogenetic functionally categorized into specific populations by
and molecular genetic techniques have demon- virtue of their expression of unique cell surface mark-
strated that translocations of chromosomes 8 and 14 ers. Normal B-cell differentiation begins at the level
are very common in this disease, and translocations of the lymphoid stem cell and proceeds through mul-
of genetic material between chromosomes 2 and 8 tiple stages, namely pre-B-cell, mature or resting
and chromosomes 8 and 22 occur much less fre- B-cell, activated or proliferative B-cell, differentiat-
quently. Each of these translocations involves juxta- ing B-cell, and finally, the appearance of the plasma
position of a gene coding for a segment of the immu- cell. These stages of normal B-cell ontogeny are
noglobulin molecule and a gene located on characterized by the expression of unique cell-surface
chromosome 8, which codes for the c-myc proto-on- and cytoplasmic antigens. Some of the antigens are
cogene, the human homologue of the retroviral v- found only at a specific level of B-cell differentiation,
VOLUME 62 • SUPPLEMENT I CLEVELAND CLINIC JOURNAL OF MEDICINESI-37
NON-HODGKIN'S LYMPHOMAS • FISHER AND OKEN
whereas others, so-called pan-B-cell antigens, are Hodgkin's lymphoma, the follicular small cleaved-
present during multiple levels of differentiation. cell lymphomas are believed to correspond to spe-
However, a sequential loss of pan-B-cell antigens cific subpopulations of germinal center B cells, and
occurs during the differentiation process. Certain an- these tumors express C D 10, CD21, B5, and the
tigens are particularly helpful in elaborating B-cell pan-B-cell antigens. By contrast, the low-grade
lineage because their expression is confined to B small lymphocytic subtype of non-Hodgkin's lym-
lymphocytes—for example, C D 1 9 , C D 2 0 , and phoma, which is the tissue counterpart of B-cell
CD24. The pre-B cell typically expresses the C D 10 CLL, corresponds to a subpopulation of activated B
antigen, which is not expressed during further matu- cells expressing CD5, CD21, B5, and the pan-B-cell
ration of the lymphocyte series beyond the pre-B- antigens. Among the intermediate-grade subtype of
cell stage. C D 10 is also referred to as C A L L A , the non-Hodgkin's lymphoma, the follicular large-cell
common acute lymphoblastic leukemia antigen. A t and the diffuse large-cell varieties express multiple
the stage of the resting B lymphocyte, expression of B-cell activation antigens as well as the pan-B-cell
CD19, CD20, and C D 2 4 continues, and these cells antigens. However, the follicular large-cell lym-
begin to express surface immunoglobulins, IgD and phoma expresses C D 10, whereas the diffuse large-
IgM as well as CD21, CD22, and CD35. The CD21 cell intermediate-grade subtype non-Hodgkin's lym-
antigen is the receptor for the Epstein-Barr virus. p h o m a does not express C D 10. A m o n g the
Multiple surface antigen changes occur on lympho- high-grade subtype of non-Hodgkin's lymphoma,
cytes as they traverse the stage of development from the immunoblastic variety is clinically indistin-
the resting B cell to the activated-proliferating B guishable and phenotypically very similar to the
cells. About the time that loss of CD21 and CD22 intermediate-grade B-cell diffuse large-cell lym-
antigens takes place, a host of activation antigens phoma. Also included in the high-grade small non-
appear that are presumed to have a key role in the cleaved-cell subtype is Burkitt's lymphoma, which
further differentiation of B lymphocytes. B-cell-asso- commonly expresses B-cell activation antigens as
ciated activation antigens include, among others, well as C D 10.
CD5, CD23, CD35, and CD71. CD71 is the trans- A s mentioned above, 3 immunophenotypic clon-
ferrin receptor. Finally, at the stage of development ality in the family of B-cell lymphoid neoplasms is
of the secretory B cell, CD38 and PCA-1 appear, usually clear-cut because the majority of cells ex-
whereas by that time there has already been a loss of press a heavy chain and a light chain on their sur-
the B-cell activation antigens and the pan-B-cell faces or in the cytoplasmic compartment, thereby
antigens. providing evidence of a monoclonal nature. Among
The cell surface phenotypic markers described the T-cell lymphomas, there is not an analogous
above are useful in the diagnosis of the non- standard for monoclonality. Numerous monoclonal
Hodgkin's lymphomas. As noted earlier, approxi- antibodies have been developed in order to detect
mately 75% of non-Hodgkin's lymphomas are of and define cell surface antigens expressed on human
B-cell origin. Virtually all of these express the p a n - T cells. T cells derive from the thymic environment,
B-cell antigens such as CD19, CD29, and la, as well where they undergo development prior to expulsion
as one or more B-cell activation antigens. The cell into the circulation and peripheral lymphatic tis-
surface antigenic phenotype has value in the diag- sues. During the three principal stages of T-cell dif-
nosis of B-cell lymphomas; however, it should be ferentiation in the thymus, there is a significant
mentioned that considerable antigenic heterogene- change in the spectrum of cell surface antigens. Dur-
ity is present within the histologically defined sub- ing the first stage of T-cell differentiation (the
groups of this disease. A wide variety of monoclonal prothymocyte stage), CD2, CD7, CD38, and CD71
antibodies has been used in the diagnosis of B-cell are expressed. Transition to stage 2 involves the loss
lymphomas. of expression of CD71 and the appearance of expres-
Even though most researchers typically relate the sion of CD1, CD4, and CD8. During stage 3 of
B-cell non-Hodgkin's lymphomas to the principal T-cell differentiation, the cells may lose C D 1 while
stages of B-lymphocyte development, it is now clear acquiring CD3, CD5, and CD6. Cells at this stage of
that these neoplasms correspond to specific sub- T-cell development also express the T-cell antigen
populations of activated-proliferating B lympho- receptor. Following completion of stage 3 in-
cytes. A m o n g the low-grade subtype of non- trathymic maturation, the T cells depart the thy-
SI-12 CLEVELAND CLINIC JOURNAL OF MEDICINE VOLUME 62 • SUPPLEMENT I
NON-HODGKIIM'S LYMPHOMAS • FISHER AND OKEN
mus, where they are broadly categorized as express- some cases, massive splenomegaly may exist. Also,
ing either C D 4 or CD8. bone marrow involvement in non-Hodgkin's lym-
Mature peripheral T cells that undergo activation phoma occurs in approximately one third of pa-
exhibit other changes in expression of surface anti- tients, although there is significant variation in the
gens. T-cell lymphomas also reflect specific stages of incidence of marrow involvement among the vari-
T-cell differentiation, and in the same sense as B- ous histologic subtypes. During the early clinical
cell lymphoid neoplasms, substantial heterogeneity phases of non-Hodgkin's lymphoma, most patients
may be seen within histologically defined subtypes. present with a normal peripheral blood picture;
High-grade lymphoblastic non-Hodgkin's lym- however, approximately one half of these patients
phomas usually exhibit a T-cell immunophenotype will develop anemia as the disease progresses. The
(approximately 95% of cases) and correspond to anemia seen in non-Hodgkin's lymphoma is typi-
stage 2 thymocytes in the sequence of T-cell differ- cally due to one of or a combination of the following
entiation. Most of the other T-cell lymphomas have causes: hypersplenism, hemorrhage, autoimmune
been reported to correspond to mature T-helper hemolytic anemia, marrow injury due to chemother-
( C D 4 ) cells or mature T-suppressor/cytotoxic apy and/or radiation, and bone marrow replacement
( C D 8 ) cells. Such lymphoblastic non-Hodgkin's due to the disease. Lymphocytosis may be seen in
lymphomas present with a diffuse growth pattern some patients; however, the white blood cell count
and occur in patients with a median age of approxi- is frequently normal in this disease.
mately 17 years, which is considerably younger than The initial clinical presentation in patients with
the median age of patients with low-, intermediate-, non-Hodgkin's lymphoma includes extranodal dis-
or other high-grade non-Hodgkin's lymphomas. ease in approximately 30% to 40% of patients. Only
approximately 10% of patients presenting with in-
dolent lymphomas have localized disease at initial
diagnosis. The diffuse aggressive lymphomas much
Approximately two thirds of patients with non- more commonly are associated with localized dis-
Hodgkin's lymphomas typically present with persist- ease at initial clinical presentation. Compared with
ent and painless superficial lymphadenopathy. Only patients with diffuse aggressive lymphoma, those
approximately 20% of patients with non-Hodgkin's with indolent lymphomas are much more likely to
lymphoma present with systemic symptoms (ie, B present initially with hepatomegaly and bone mar-
symptoms), in contrast to an approximate 40% inci- row involvement. When jaundice is encountered, it
dence of systemic symptoms among patients initially usually reflects infiltration of the liver by malignant
presenting with Hodgkin's disease. Also, approxi- cells, although it may also result from extrahepatic
mately 20% of patients with non-Hodgkin's lym- biliary tract obstruction. Gastrointestinal tract in-
phomas exhibit mediastinal adenopathy. This is, of volvement, whether as a primary or secondary site of
course, much less frequent than the same finding in disease activity, can be reflected by symptoms such
patients with Hodgkin's disease. In many cases of as malabsorption, bleeding, obstruction, abdominal
non-Hodgkin's lymphoma, there is involvement of pain, and accompanying diarrhea. In some cases,
pelvic, mesenteric, and retroperitoneal lymph frank perforation may occur as a result of tumor
nodes, although it is usually not symptomatic. involvement.
Among non-Hodgkin's lymphoma patients who Extranodal involvement in the non-Hodgkin's
present with mediastinal adenopathy, complaints of lymphomas may involve other tissues also; primary
chest pain or an unremitting cough are not uncom- lesions have been described in the testes, thyroid,
mon. Patients with large T-cell lymphomas and me- lung, bone, female reproductive tract, and other tis-
diastinal lymphadenopathy may present with a su- sues. These extranodal presentations are more typi-
perior vena cava syndrome. Lymphatic tissue cally associated with the diffuse histiocytic lym-
throughout the body may be involved in the non- phomas. Renal dysfunction usually reflects the
Hodgkin's lymphomas, including mesenteric, presence of urinary outflow tract obstruction by tu-
epitrochlear, and preauricular lymph nodes, as well mor. The most frequent clinical manifestation of
as the tissues found within Waldeyer's ring. Ap- non-Hodgkin's lymphomas in the nervous system
proximately 20% of patients with non-Hodgkin's involves compression of the spinal cord due to ex-
lymphoma present with palpable splenomegaly; in tradural tumor mass. Involvement of the brain pa-
VOLUME 62 • SUPPLEMENT I CLEVELAND CLINIC JOURNAL OF MEDICINES I - 37
NON-HODGKIN'S LYMPHOMAS • FISHER AND OKEN
TABLE 2
THE ANN ARBOR STAGING CLASSIFICATION*
Stage I Involvement of a single lymph node region (I) or of a single extralymphaticorgan or site (IE)+
Stage II Involvement of two or more lymph node regions on the same side of the diaphragm (li) or localized
involvement of an extralymphatic organ or site and of one or more lymph node regions on the same
side of the diaphragm (HE)
Stage III Involvement of lymph node regions on both sides of the diaphragm (III), which may also be accompanied
by involvement of the spleen (Ills), or by localized involvement of an extralymphatic organ or site (IIIE)
or both (IIISE)
Stage IV Diffuse or disseminated involvement of one or more extralymphatic organs or tissues, with or without
associated lymph node involvement
'Reprinted
f
from Gaynor and Fisher, reference 3, with permission
The subscript E denotes involvement of an extralymphatic site. Asymptomatic patients are denoted by the suffix A; systemic
symptoms (fever > 38°C, night sweats, weight loss > 10% of body weight) are denoted by the suffix b
renchyma has historically been very rare as a site for tuberculosis, acute and chronic leukemia, infectious
primary non-Hodgkin's lymphoma; however, the mononucleosis, cytomegalovirus, infection by hu-
A I D S epidemic may bring about a substantially in- man immunodeficiency virus (HIV), and parasitic
creased frequency of non-Hodgkin's lymphoma as a diseases, as well as other causes of lymphade-
primary brain tumor. Finally, the non-Hodgkin's nopathy. Although it is not possible to establish
lymphomas may present as primary skin neoplasms. conclusively a diagnosis of non-Hodgkin's lym-
Cutaneous T-cell lymphoma represents a malignant phoma in the absence of additional test results,
clonal proliferation of T lymphocytes predomi- some clinical characteristics do suggest this diagno-
nantly of the C D 4 phenotype. T h e principal presen- sis—for example, the involvement of epitrochlear
tations of this disorder are mycosis fungoides, which and mesenteric lymph nodes and Waldeyer's ring.
is a limited or generalized patchy or plaque-associ-
ated illness constituting approximately 90% of all DIAGNOSIS AND CLASSIFICATION
C T C L patients, and Sezary's syndrome, which is a
diffuse erythroderma with atypical circulating cells T h e A n n Arbor staging classification is the most
present in peripheral blood. T h e collective preva- widely used system for staging of non-Hodgkin's
lence of these presentations is approximately 3000 lymphomas (Table 2). Originally developed for use
to 4000 patients in the United States, with approxi- in Hodgkin's disease, the A n n Arbor staging classifi-
mately 600 new cases reported each year. T h e clini- cation effectively provides an anatomic staging sys-
cal course of C T C L is usually indolent, especially for tem in which the diaphragm serves as the principal
patients whose disease is confined to the skin. landmark. T h e system incorporates information on
A s mentioned above, many patients with non- the presence or absence of systemic symptoms such
Hodgkin's lymphoma present with asymptomatic as fever, night sweats, and weight loss with the num-
superficial lymphadenopathy. In comparison with ber of nodal or extranodal sites of tumor involve-
patients with Hodgkin's disease, who typically pre- ment. T h e prognostic value of the A n n Arbor stag-
sent with fever, night sweats, weight loss, and other ing classification system is greater for Hodgkin's
symptoms, it is uncommon for patients with the disease than for the non-Hodgkin's lymphomas. In
non-Hodgkin's lymphomas to exhibit these initial the former, disease typically spreads through con-
clinical signs and symptoms. Nonetheless, fever, tiguous groups of lymph nodes. By contrast, the
night sweats, and weight loss as well as pruritus, non-Hodgkin's lymphomas typically exhibit hema-
anemia, gastrointestinal symptoms, bone pain, pleu- togenous spread; accordingly, this staging system is
ral effusion, and chylous ascites may be present rela- less useful. Ostensibly, the A n n Arbor staging classi-
tively early on, depending on the level of aggressive- fication system is used to identify those patients
ness of the disease. T h e differential diagnosis with suspected non-Hodgkin's lymphoma who can
includes Hodgkin's disease, metastatic carcinoma, be treated with localized therapy, although many
SI-14 CLEVELAND CLINIC JOURNAL OF MEDICINE VOLUME 62 • SUPPLEMENT I
NON-HODGKIIM'S LYMPHOMAS • FISHER AND OKEN
p a t i e n t s with suspected
TABLE 3
low-grade non-Hodgkin's STAGING EVALUATION FOR NON-HODGKIN'S LYMPHOMAS*
lymphoma do not, after ap-
p r o p r i a t e staging proce- Required for all patients
dures have been conducted, Detailed history and physical examination with thorough lymph node evaluation
exhibit only localized dis- Complete blood count, liver and renal function tests, serum protein electrophoresis,
ease. Irrespective, however, actic dehydrogenase, alkaline phosphatase
of any deficiencies in appli- Chest roentgenogram
cation of the A n n Arbor Computed tomography (CT) scan of abdomen and pelvis
staging classification to the Bilateral iliac crest bone marrow biopsies
non-Hodgkin's lymphomas, Required or useful in selected circumstances
a thoroughly organized ap- Thoracic CT scan, if chest roentgenogram abnormal
proach to staging is essen- Liver biopsy
tial for any patient with a Radionuclide scans: bone, gallium, liver, spleen
suspected diagnosis of non- CT scan of head
Hodgkin's lymphoma. Chromosomal analysis
T h e d i a g n o s t i c evalu-Gene rearrangement analysis
ation of patients with sus- Cell surface markers
pected non-Hodgkin's lym- Magnetic resonance imaging
p h o m a is designed to Abdominal ultrasound
establish the stage of the Lymphangiogram
disease and to specify sites
of tumor involvement to 'Adapted from Gaynor and Fisher, reference 3, with permission
best assess the patient's re-
sponse to treatment (Table
3). In addition to the initial excisional biopsy and should be c o n d u c t e d , including bilateral lym-
subsequent documentation of the pathology and im- phangiograms of the lower extremities, bone scans
munology related to that biopsy, the diagnostic and gallium scans, magnetic resonance imaging
evaluation should include the following items: a de- studies, and C T scans of the head, as well as addi-
tailed history and physical examination; complete tional studies of gene rearrangements and cell sur-
blood counts and blood chemistries, including renal face markers. A staging laparotomy is rarely recom-
and liver function tests, serum protein electrophore- mended in non-Hodgkin's lymphoma because of its
sis, serum lactate dehydrogenase, and serum alkaline high morbidity and because other studies should
phosphatase; a chest roentgenogram to rule out the sufficiently reflect the clinical state of the patient.
presence of hilar or mediastinal lymphadenopathy, T h e p a t h o l o g i c classification of the non-
pleural effusions, and other pulmonary involve- Hodgkin's lymphomas has been a source of confusion
ment; a chest computed tomography ( C T ) scan in for clinicians and histopathologists for many years,
the event of an abnormal chest roentgenogram; C T partly because at least six separate classification sys-
scans of the chest, pelvis, and abdomen to assess tems exist for this disease. The Rappaport Classifica-
possible lymphadenopathy in the mesenteric and tion is the most widely used system in the United
retroperitoneal nodes; and bilateral iliac crest bone States and was first published almost 30 years ago. 4
marrow biopsies. In the event of significant hepa- According to the Rappaport Classification system,
tomegaly, a positive liver scan, or abnormally ele- the non-Hodgkin's lymphomas are divided into two
vated liver function test levels, a liver biopsy should principal subtypes: nodular or follicular lymphomas
be carried out. Also, pathology studies involving and diffuse lymphomas. In the former group, the
morphologic evaluation of tissues should be con- lymphomatous tissue retains certain morphologic
ducted by a competent hematopathologist. Addi- characteristics of normal lymph nodes, whereas in
tionally, under certain conditions, for instance, the diffuse lymphomas, the normal cortical and para-
where spread to bone or lower limb lymphatics is cortical lymph node morphology is obliterated. It
suspected, other staging studies based on patient also segments the non-Hodgkin's lymphomas into
symptoms and availability of diagnostic procedures subdivisions based on whether or not the malignant
VOLUME 62 • SUPPLEMENT I CLEVELAND CLINIC JOURNAL OF MEDICINES I - 37
NON-HODGKIN'S LYMPHOMAS • FISHER AND OKEN
cells are well differentiated, poorly differentiated, Hodgkin's lymphoma were reported that did not
histiocytic, or undifferentiated. The Rappaport Clas- appear to fit into the subdivisions of the Working
sification has undeniable merit, not only because it Formulation. These include, for example, mucosa-
was the first established classification system for the associated lymphoid tissue lymphomas (the so-
non-Hodgkin's lymphomas and, as indicated above, called MALTomas), a group of low-grade lym-
the most widely used in the United States today, but phomas commonly involving extranodal tissue such
also because it offers a classification system in which as the gastrointestinal tract, skin, breast, and thyroid
each histologically defined subgroup exhibits a gland. The clinical course of patients with these
unique and characteristic natural history and re- types of non-Hodgkin's lymphoma is typically that
sponse to treatment. Nonetheless, advances in con- of a low-grade lymphoma. The monocytoid B-cell
temporary immunobiology have shown that the lymphomas constitute yet another group.8 Patients
Rappaport Classification system has several defects. afflicted with these types of non-Hodgkin's lym-
For example, the term "histiocytic" cells of the Rap- phoma are typically elderly women who initially
paport Classification is a misnomer because most of present with disseminated disease. By contrast,
the tumors are actually large transformed lympho- mantle cell lymphomas refer to intermediate lym-
cytes. phocytic lymphomas that are of either the diffuse
Less than a decade following introduction of the intermediate or mantle zone types. 9 Anaplastic
Rappaport Classification, the Lukes-Collins 5 and large-cell lymphoma is usually of T-cell origin and,
Kiel 6 classifications for the non-Hodgkin's lym- because of its anaplastic morphology, may be con-
phomas appeared, and by 1980, there were at least a fused with carcinomas. 10 Patients with anaplastic
half dozen separate classification systems. The ac- large-cell non-Hodgkin's lymphoma frequently dis-
companying confusion resulted in development of play the Ki-1 antigen and sometimes exhibit a t(2;5)
the Working Formulation of Non-Hodgkin's Lym- chromosomal translocation. This type of non-
phomas for Clinical Usage, 7 an attempt to provide a Hodgkin's lymphoma appears to be relatively com-
consistent language for classification of the lym- mon in children, who typically present with extra-
phomas. The Working Formulation, introduced in nodal disease, particularly of the skin.
1982, has succeeded as a tool for the correlation of Another non-Hodgkin's lymphoma that, in addi-
several histologic classifications of the non- tion to the mantle cell lymphomas, MALTomas, and
Hodgkin's lymphomas. T h e Working Formulation anaplastic large-cell lymphomas, does not fit well
classifies these diseases by their natural histories and into the Working Formulation is adult T-cell leuke-
responses to treatment. It does not use the term mia/lymphoma, which is associated with infection
"histiocytic," referring instead to "large cells." Both by HTLV-I (human T-cell leukemia/lymphoma type
the Working Formulation and the Rappaport Classi- I). This disease is more common in Japan, the Ca-
fication separate these diseases into groups based on ribbean, and the southeastern United States and is
morphology of the involved lymph nodes. T h e often associated with hypercalcemia and a rapidly
nodular pattern in the Rappaport Classification is progressive clinical course.
referred to as follicular in the Working Formulation, Other non-Hodgkin's lymphomas that are can-
whereas diffuse patterns are described identically (as cers of T-cell origin and do not fit well into the
diffuse) in both systems. Also, both classification Working Formulation include mycosis fungoides
systems segregate the non-Hodgkin's lymphomas ac- and Sezary's syndrome. Collectively, these two dis-
cording to the size of the predominant malignant orders are referred to as the C T C L s . From the stand-
cell. Table 1 compares the Working Formulation and point of immunophenotype, the cancerous cells in
Rappaport Classification and clearly indicates the these two diseases are mature helper (CD4) lympho-
ease of translating one classification system into the cytes. Patients with these diseases do not exhibit
other. In the Rappaport Classification scheme, the symptoms reflecting excessive levels of helper T
term "lymphocytic" is used when the cells of interest cells and are often misdiagnosed because their
are small; in the Working Formulation, by contrast, plaque-like skin lesions, which may be generalized
the straightforward "small" is used to describe such or highly localized, may be misinterpreted as psoria-
cells. sis prior to histologic evaluation. Alternatively, cer-
Not long after publication of the Working For- tain patients have more readily identifiable cutane-
mulation in 1982, several subtypes of non- ous tumors or generalized erythroderma. In the
SI-16 CLEVELAND CLINIC JOURNAL OF MEDICINE VOLUME 62 • SUPPLEMENT I
NON-HODGKIIM'S LYMPHOMAS • FISHER AND OKEN
C T C L s , the cancerous cells are believed initially to with complete responses (CRs). Clinical charac-
colonize skin, with subsequent invasion of lym- teristics associated with overall survival and relapse-
phatic channels and viscera. In patients with very free survival were identified in multivariate analyses
limited focal plaque skin disease, one is less likely to by proportional-hazards regression. Those features
encounter evidence of visceral involvement com- that remained independently significant according
pared with patients who present with generalized to the regression analyses of survival were incorpo-
erythroderma, in which typically there is convinc- rated into models identifying groups of patients of
ing evidence of extracutaneous disease. Patients all ages, as well as groups of patients not more than
who exhibit visceral disease have the worst progno- 60 years old with different risks of death.
sis of patients with C T C L s ; it is rare to encounter The authors developed two models. The first, the
visceral disease in the absence of lymph node in- International Index, is applicable to all the patients
volvement in these patients. In general, the C T C L s studied and incorporates clinical features reflecting
are considered indolent lymphomas, in which for the growth and invasive potential of the tumor (tu-
most patients disseminated disease is the rule at the mor stage, serum LDH level, and number of extra-
time of initial clinical diagnosis. Also, the C T C L s nodal disease sites), the patient's symptoms from the
may be confused with the generalized skin lesions tumor (performance status), and the patient's ability
occurring in adult T-cell leukemia/lymphoma. One to tolerate intensive therapy (age and performance
can usually distinguish between mycosis fun- status). For patients 60 years or younger, an age-ad-
goides/Sezary's syndrome and adult T-cell leuke- justed model was developed and is referred to as the
mia/lymphoma by virtue of the fact that, in the Age-Adjusted International Index. 40 This employs a
latter, hypercalcemia, opportunistic infections, lung subgroup of clinical features including tumor stage,
and bone tumor involvement, and early age of onset serum LDH level, and performance status. Both the
frequently exist, whereas these are seldom seen in International Index and the Age-Adjusted Interna-
the C T C L s . Unfortunately, because adult T-cell leu- tional Index models identified risk groups of pa-
kemia/lymphoma may exhibit a wide variety of his- tients, based on both the rate of C R and the rate of
tologic features, histopathology is often not particu- relapse from C R . In the evaluation of more than
larly useful in establishing an accurate diagnosis. 2000 patients of all ages, the model identified four
As mentioned, the tumor stage of patients with risk groups with predicted 5-year survival rates of
aggressive non-Hodgkin's lymphoma is presently de- 73%, 51%, 43%, and 26%. In the age-adjusted
termined by the A n n Arbor staging classification model (patients 60 years or younger), four other risk
system (originally developed for use in Hodgkin's groups were also identified and had predicted 5-year
disease), even though applying the system to the survival rates of 83%, 69%, 46%, and 32%. The
non-Hodgkin's lymphomas might not provide great authors 40 noted that in both predictive models, the
accuracy in the identification of prognostic sub- increased risk of death was due to a lower rate of C R
groups of patients. T h e International N o n - as well as to a higher rate of relapse from C R . They
Hodgkin's Lymphoma Prognostic Factors Project determined that the two indices were significantly
was conducted to develop a predictive model for more accurate than the A n n Arbor staging classifi-
determining outcome in patients with aggressive cation in predicting long-term survival in patients
non-Hodgkin's lymphoma on the basis of clinical with aggressive non-Hodgkin's lymphoma. T h e
characteristics prior to treatment. 40 Sixteen aca- authors proposed that clinical prognostic factor
demic institutions and oncology cooperative groups models such as the International Index and the
in the United States, Canada, and Europe partici- Age-Adjusted International Index be used to iden-
pated in the project, which involved an evaluation tify specific risk groups and to compare different
of adult patients for clinical features that would pre- treatment modalities in patients with aggressive
dict overall survival and relapse-free survival. The non-Hodgkin's lymphoma. Even though these indi-
patients were treated between 1982 and 1987 with ces were specifically developed for aggressive non-
combination chemotherapy regimens containing Hodgkin's lymphoma, they might have significant
doxorubicin. Step-down statistical regression meth- utility as predictive models for patients with more
ods were employed to develop statistical models for indolent disease. This is exemplified by a report41
the association of prognostic factors with overall from France that evaluated the prognostic factors in
survival and relapse-free survival among patients patients with follicular lymphomas.
VOLUME 62 • SUPPLEMENT I CLEVELAND CLINIC JOURNAL OF MEDICINESI-37
NON-HODGKIN'S LYMPHOMAS • FISHER AND OKEN
Even though the predictive model for aggressive portance of extensive and accurate histologic evalu-
non-Hodgkin's lymphoma proposed by the Interna- ation of patients with non-Hodgkin's lymphoma.
tional Non-Hodgkin's Lymphoma Prognostic Factors Approximately 20% of the aggressive non-
Project Group'10 has been rather widely embraced as a Hodgkin's lymphomas are of T-cell origin. They ex-
meaningful tool in the design of therapeutic trials hibit histologic heterogeneity and, according to the
and in the selection of appropriate treatment mo- Working Formulation, principally comprise the sub-
dalities for individual patients, it has not received divisions of diffuse, mixed small- and large-cell lym-
universal acceptance. For example, it has been criti- phoma, and large-cell immunoblastic lymphoma.
cized because patients with AIDS-associated non- These tumors respond to aggressive chemotherapy
Hodgkin's lymphoma were not included. According and, generally speaking, the response of high-grade
to the authors of the predictive model, patients with T-cell lymphomas is approximately the same as that
AIDS-associated non-Hodgkin's lymphoma were ex- of B-cell lymphomas. As such, immunophenotype
cluded from the International Index because they per se is not particularly useful in predicting whether
have less favorable prognoses and tolerate chemo- or not a patient will respond to aggressive therapy.
therapy poorly because of the presence of cytopenia According to the Working Formulation, 7 the in-
and concurrent infections. Notwithstanding criti- dolent or low-grade lymphomas include the small
cisms in this and other regards, the predictive model lymphocytic lymphomas, follicular small cleaved-
proposed by the International Prognostic Factors cell lymphoma, and follicular mixed small cleaved-
Group appears to represent a considerable improve- and large-cell lymphoma. Almost 100% of the low-
ment over staging alone. grade non-Hodgkin's lymphomas are of B-cell ori-
In contrast with the indolent or low-grade lym- gin. These histologic diagnoses are usually associ-
phomas, the high-grade lymphomas have a clini- ated with an indolent clinical course. Even though
cally aggressive natural history and in the absence of patients typically present with disseminated disease,
treatment commonly cause death in less than 2 the low-grade non-Hodgkin's lymphomas may have
years from initial clinical presentation. Ironically, a comparatively long duration even without institu-
the aggressive, high-grade non-Hodgkin's lym- tion of aggressive chemotherapy. Although chemo-
phomas may offer a better prognosis than the indo- therapy may halt tumor progression in the low-grade
lent lymphomas if they are treated promptly and in non-Hodgkin's lymphomas, it very rarely offers a
an appropriate fashion. Many patients diagnosed cure. In addition to the low-grade non-Hodgkin's
with aggressive non-Hodgkin's lymphoma will be lymphomas mentioned above, other subtypes that
cured of the disease if a complete remission is do not comfortably fit into the subdivisions of the
achieved and sustained for at least 2 years.42 There is Working Formulation and that are more aggressive
considerable heterogeneity from an immunologic than the classic indolent lymphomas include diffuse
and histologic standpoint among the aggressive intermediate lymphocytic lymphoma and its follicu-
non-Hodgkin's lymphomas, which are categorized lar variant, the mantle zone lymphoma.
in the intermediate- and high-grade divisions of the Diffuse intermediate lymphocytic lymphoma ap-
Working Formulation. 43 The majority of these lym- pears to be the equivalent of the centrocytic lym-
phomas appear to be of B-cell origin, and it is likely phoma in the Kiel Classification. 6 Despite its cate-
that many are derived from low-grade B-cell neo- gorization by some investigators as an indolent
plasms. In this regard, it is well known that multi- lymphoma, diffuse intermediate lymphocytic lym-
ple-site biopsies obtained at initial patient presenta- phoma has a poorer prognosis than that seen in the
tion may show more than one histologic low-grade lymphomas described in the Working
appearance. For example, a high-grade lymphoma Formulation. 45,46 Extensive histologic variation may
may be found at one anatomic site while an indolent exist among the indolent lymphomas, and more
lesion may be found at another. 44 Such histologic than one histologic subtype may be found in the
findings may have great clinical significance be- same pathologic specimen or in different specimens.
cause, even though the high-grade lesion may suc- The most frequently encountered discordant pat-
cessfully respond to treatment, the low-grade site tern is the combination of diffuse large-cell lym-
may be more refractory. Thus a patient with these phoma in the diagnostic lymph node biopsy and the
findings may experience relapse with a low-grade presence of small cleaved-cell lymphoma in the
lymphoma. This situation underscores the great im- bone marrow biopsy.47
SI-18 CLEVELAND CLINIC JOURNAL OF MEDICINE VOLUME 62 • SUPPLEMENT I
NON-HODGKIIM'S LYMPHOMAS • FISHER AND OKEN
A c o n s i d e r a b l e number of c l i n i c a l and
TABLE 4
pathologic characteristics have been identified as PROGNOSTIC FACTORS IN THE INDOLENT
prognostic factors in the indolent non-Hodgkin's NON-HODGKIN'S LYMPHOMAS*
lymphomas 48 " 52 (Table 4). T h e strongest predictor of
Feature Prognosis
survival in the low-grade non-Hodgkin's lym-
phomas is the response to initial treatment. 5 2 Other Pathobiological
characteristics associated with a favorable progno- Cytogenetic abnormalities Unfavorable
sis include the extent of helper T-cell host infil- Increased nuclear proliferation Unfavorable
trates, 53 " 55 a normal hemoglobin level, 48 ' 52 and a lim- Helper T-cell infiltrates Favorable
Absence of interfollicular fibrosis Unfavorable
ited A n n Arbor staging classification ( A n n Arbor Mixed pattern (follicular plus diffuse) Equivocal
stage I or II). 48,49,51,52 Other favorable prognostic fac- Number of large cells Equivocal
tors in low-grade lymphomas include the number of Clinical
large cells and the degree of follicularity noted dur- Normal hemoglobin Favorable
ing histopathologic evaluation. Good performance status Favorable
Limited Ann Arbor stage Favorable
There is significant variation among pathologists Age > 60 Unfavorable
in their quantification of large cells in follicular Male Unfavorable
lymphoma and, as a result, many oncologists are not Systemic symptoms Unfavorable
Extranodal sites > 2 Unfavorable
comfortable relying on the number of large cells in Bulky tumor Unfavorable
establishing a prognosis in such patients. Also, the Hepatosplenomegaly Unfavorable
degree of follicularity in the indolent non-Hodgkin's Elevated lactic dehydrogenase
or (32 microglobulin > 3 mg/day Unfavorable
lymphomas at the time of diagnosis is considered to Bone marrow involvement > 20% Unfavorable
be equivocal as a prognostic factor: the determina-
tion of survival differences among patients display- Adapted from Horning, reference 47, with permission
ing predominantly diffuse patterns vs those display-
ing predominantly follicular patterns may depend
substantially on the treatment used. This is exempli- index for all stages, 48 have been proposed. In addi-
fied by the study of Hu et al, 56 which disclosed in a tion, prognostic factors have been described for pa-
retrospective review that predominantly diffuse tients who relapsed during treatment of indolent
mixed lymphomas appear to have a significantly less non-Hodgkin's lymphoma 58 ; the most predictive
favorable prognosis than do predominantly follicu- prognostic factors in these patients were initial re-
lar lymphomas when the treatments involved mild sponse, age, and duration of response.
chemotherapy. Unfavorable prognostic factors in
the indolent lymphomas include, among others, ab- TREATMENT OF THE NON-HODGKIN'S LYMPHOMAS
sence of interfollicular fibrosis 41 and increased ex-
pression of certain nuclear proliferation antigens T h e past decade has witnessed significant ad-
(eg, Ki-67) and the percentage of cells in S phase. 57 vances in our understanding of the biology and
Elevated levels of serum lactic dehydrogenase and treatment of the non-Hodgkin's lymphomas. In a
^-microglobulin, which are established prognostic recent review article on the treatment of these dis-
determinants in aggressive non-Hodgkin's lym- orders, Armitage 5 9 proposes that a physician seeing a
phomas, are also unfavorable prognostic factors in new patient with non-Hodgkin's lymphoma should
the indolent forms of the disease. first consider the diagnosis, then prognosis, choice
Patients with low-grade lymphomas exhibit con- of treatment, and finally treatment itself.
siderable variability in clinical and histopathologic A s a general principle, the physician should be
findings at the time of diagnosis. A predictive model aware of the specific histologic diagnosis, the clini-
for indolent non-Hodgkin's lymphomas, analogous cal extent of the lymphomatous involvement, and
to that described above for aggressive forms of the the patient's age and overall health. T h e great ma-
disease, would benefit the design of future clinical jority of patients with non-Hodgkin's lymphoma
trials in patients with indolent disease and the selec- should receive chemotherapy with or without irra-
tion of appropriate treatments for individual pa- diation, as discussed below. Radiation therapy has
tients. Prognostic factor indices for stage IV follicu- only a very limited value as a primary treatment for
lar low-grade lymphoma, 50 as well as a prognostic most patients with non-Hodgkin's lymphoma. Sur-
VOLUME 62 • SUPPLEMENT I CLEVELAND CLINIC JOURNAL OF MEDICINES I - 37
NON-HODGKIN'S LYMPHOMAS • FISHER AND OKEN
gery is virtually never suggested as the sole treat- non-Hodgkin's lymphoma commonly survive with
ment for patients with these diseases. Ostensibly, multiple episodes of recurrence. A t 5 years, survival
the ultimate treatment outcome is likely determined is approximately 80%, but this value falls to be-
more by the disease stage and other prognostic fac- tween 30% and 50% at 10 years.
tors than by the specific treatment regimen selected. Alkylating agents. Alone or in combination, alkyl-
Nonetheless, the non-Hodgkin's lymphomas in gen- ating a g e n t s h a v e b e e n the standard chemo-
eral are very responsive to chemotherapy and as a therapeutic agents for the treatment of low-grade
group are very radiosensitive. A n accurate his- non-Hodgkin's lymphoma. They have been used for
tologic and clinical evaluation is important to dis- many years in the treatment of patients with ad-
tinguish clearly between indolent and aggressive vanced-stage indolent lymphoma. Chlorambucil
disease so that optimal chemotherapeutic and/or ra- administered at a daily oral dose of between 0.1 and
diation treatment plans can be selected. 0.2 mg/kg or cyclophosphamide at a daily oral dose
of 1.5 to 2.5 mg/kg is commonly used. T h e dose of
Stage I or II low-grade lymphomas each of these agents is titrated to maintain a platelet
Patients with low-grade non-Hodgkin's lym- count greater than 100 000/mm 3 and a white blood
phomas usually present with localized disease only cell count greater than 3000/mm 3 . Such an ap-
after a complete clinical staging is conducted; in proach to treatment may bring about clinical re-
fact, only approximately 10% of patients with indo- sponses in a very slow fashion and, in fact, in some
lent lymphoma will be discovered to have stage I or patients it takes 2 to 3 years in order to achieve a
II disease. 60 Such patients may benefit considerably complete remission. T h e use of pulse chlorambucil
from regional irradiation. While the frequency of in an oral dose of 16 mg/m 2 daily for 5 days may
curative irradiation in the non-Hodgkin's lym- result in a much faster antitumor response compared
phomas is certainly low, it is likely that for selected with the use of daily oral chlorambucil. 61 With this
patients who are accurately diagnosed as stage I or approach, hematologic and other acute toxicities
stage II, with nonbulky, contiguous disease, irradia- are relatively low; however, long-term daily alkylat-
tion as sole therapy may produce a complete remis- ing agent treatment has been associated with an
sion of considerable length. T h e prolonged disease- increased frequency of acute myelogenous leukemia
free survival of patients with stage I or II disease in other disease states.
supports the position that, in the absence of addi- Combination chemotherapy. As an alternative to
tional prospective clinical data, regional irradiation the use of chlorambucil or cyclophosphamide in the
is the standard treatment for such patients. A n ef- stage III or IV indolent non-Hodgkin's lymphomas,
fort is made to limit the irradiation to areas of c o m b i n a t i o n chemotherapy may be used. Two
known disease, thus not damaging normal bone widely employed combinations are the C V P regi-
marrow that may be crucial for the patient's future men and the C - M O P P regimen. T h e C V P regimen
ability to tolerate possible chemotherapy. consists of cyclophosphamide (400 mg/m 2 by mouth
daily for 5 days), vincristine (1.4 mg/m 2 intrave-
Stage III or IV low-grade lymphomas nously on day 1), and prednisone (100 mg/m 2 by
Most patients diagnosed with low-grade lym- mouth daily for 5 days). In this regimen, treatment
phoma have advanced disease at the time of initial is repeated every 21 days and should be continued
clinical presentation (stage III or IV). For such pa- for a minimum of six cycles or, alternatively, for two
tients, there are many acceptable treatment options, cycles following attainment of a complete clinical
although the likelihood of cure is low. Many of the response. T h e C - M O P P regimen consists of cyclo-
treatment regimens produce a 60% to 75% rate of phosphamide (650 mg/m 2 intravenously on days 1
complete remission; however, such remissions are and 8), vincristine ( 1.4 mg/m 2 intravenously on days
typically of short duration and, again, cure is rare. 1 and 8), procarbazine ( 100 mg/m 2 by mouth on days
T h e median disease-free interval following the com- 1 through 14), and prednisone (40 mg/m 2 by mouth
p l e t i o n of treatment is only approximately 17 on days 1 through 14. T h e C - M O P P regimen treat-
months. Following relapse, re-treatment may pro- ment cycle is repeated every 28 days.
vide good results; however, the disease-free interval It is important to underscore that in the treat-
and complete remission rate decline with each re- ment of the indolent non-Hodgkin's lymphomas,
treatment. Patients with stage III or IV indolent complete remissions may be achieved using a variety
SI-20 CLEVELAND CLINIC JOURNAL OF MEDICINE VOLUME 62 • SUPPLEMENT I
NON-HODGKIIM'S LYMPHOMAS • FISHER AND OKEN
of therapeutic regimens. The treating clinician may one fourth of such patients may show evidence of
elect to administer a single alkylating agent, combi- spontaneous disease regression in the absence of
nation chemotherapy utilizing the C V P or C - treatment. However, such an event is usually only a
MOPP regimen or other regimens, or alternative partial regression that is temporary in most cases.
therapy such as total body or total nodal irradiation. The follicular, mixed small cleaved and large-cell
Moreover, in some instances, a watch-and-wait ap- variety of malignant lymphoma (nodular mixed
proach may be preferred. Portlock and Rosenberg 62 lymphocytic-histiocytic cell) is considered by some
at Stanford University have advocated a watch-and- to represent a unique subtype of low-grade non-
wait approach for stages III and IV non-Hodgkin's Hodgkin's lymphoma. Optimal treatment for this
lymphoma of indolent histologic types. A retrospec- variety is unclear at the present time, although it is
tive evaluation of the watch-and-wait approach common for oncologists to treat patients with this
compared with other treatment regimens disclosed subtype in the same fashion as they treat patients
that survival in the watch-and-wait patient group diagnosed as having malignant lymphoma, follicu-
was approximately the same as that for patients who lar, predominantly small cleaved-cell disease (nodu-
had received alternative treatment at the time of lar poorly differentiated lymphocytic lymphoma).
clinical diagnosis. Essentially, they demonstrated Longo et al63 at the National Cancer Institute have
that asymptomatic patients may not need systemic reported that prolonged complete remissions are
treatment for several years following the initial diag- possible in such patients when treated with the C -
nosis. Accordingly, it has been proposed that asymp- MOPP regimen. By contrast, however, Glick et al64
tomatic patients with advanced-stage indolent non- were unable to confirm a prolonged disease-free sur-
Hodgkin's lymphomas be observed and that vival with combination chemotherapy.
treatment be implemented only when clearly indi- In addition to the treatment regimens described
cated from the clinical standpoint. The watch-and- above, some new and promising therapeutic ap-
wait approach to the treatment of advanced-stage proaches have been used for the indolent non-
low-grade non-Hodgkin's lymphomas has been used Hodgkin's lymphomas, including bone marrow
frequently in the United States for the clinical man- transplantation, monoclonal antibody therapy, bio-
agement of such patients. The "watch" component logic therapies such as the use of recombinant hu-
of the watch-and-wait approach is very important. man interferon alfa (rHuIFN-a), and several new
The clinician should evaluate these patients at least chemotherapeutic agents.
every 2 months to be assured that implementation Bone marrow transplantation. Bone marrow trans-
of alternative therapy is not being neglected when plantation has emerged as a useful therapy which
essential. In any case, appropriate therapy involving may lead to extended disease-free survival in a sig-
drugs and/or irradiation should be promptly consid- nificant number of patients with relapsed low-grade
ered if a patient presents with evidence of extensive non-Hodgkin's lymphomas. 65 Allogeneic bone mar-
visceral or bone marrow disease. Total body irradia- row transplantation appears to have a role in the
tion may involve total doses of 150 to 300 Gy at a treatment of patients with small lymphocytic lym-
daily dose of 10 Gy. In such cases, routine monitor- phoma consistent with CLL, and autologous trans-
ing for peripheral cytopenias is essential because plantation appears to have merit in the treatment of
thrombocytopenia is not uncommon. Alternatively, low-grade follicular lymphomas. It is interesting to
total nodal irradiation has been successfully applied note that of the several thousand autologous bone
in patients with stage III indolent disease. In making marrow transplantation procedures conducted
a determination of the optimal approach to treat- worldwide each year, non-Hodgkin's lymphoma is
ment for a given patient with advanced-stage indo- the disease most frequently treated. 66
lent non-Hodgkin's lymphoma, the physician
There has been considerable debate about the
should appreciate that with watchful waiting, the
relative value of allogeneic vs autologous bone mar-
median time before therapy is required is approxi-
row transplantation in the treatment of patients
mately 3 years, and approximately 20% of patients
with indolent lymphoma. Because patients with
do not require therapy for up to 10 years.62 The
small lymphocytic lymphoma/CLL typically exhibit
overall median survival is approximately 11 years
lymphomatous involvement of the bone marrow as
and the median 10-year survival is approximately
well as circulating cancer cells, autologous bone
73%. Interestingly, it has been estimated that up to
marrow transplantation does not appear particularly
VOLUME 62 • SUPPLEMENT I CLEVELAND CLINIC JOURNAL OF MEDICINES I - 37
NON-HODGKIN'S LYMPHOMAS • FISHER AND OKEN
well suited to such patients. By contrast, patients ated total body irradiation with or without addi-
with low-grade follicular lymphomas typically have tional chemotherapy as a preparative regimen. T h e
a lesser incidence of marrow and peripheral blood majority of patients exhibited a strong anticancer
tumor infiltration. Accordingly, an autologous bone effect from the high-dose therapy. T h e authors 70 cite
marrow transplant or autologous peripheral stem- that in two of the patients, molecular biologic ex-
cell transplant appears reasonable for many of these periments disclosed no measurable evidence of re-
patients. This is the case even considering that most sidual disease. Results from the study of Rabinowe et
p a t i e n t s with a d v a n c e d - s t a g e indolent non- al71 also provide optimism. T h a t group reported
Hodgkin's lymphomas do exhibit tumor involve- studies involving allogeneic or autologous bone
ment on bone marrow biopsy. marrow transplantation with purging in patients
There is no universal agreement about the opti- with CLL. T h e patients were pretreated with vari-
mal timing of bone marrow transplantation for pa- ous chemotherapeutic agents to reduce tumor bulk
tients with low-grade non-Hodgkin's lymphoma. A t and then were administered high-dose cyclophos-
present, the use of bone marrow transplantation is phamide and total body irradiation immediately
generally reserved for patients who have not exhib- prior to the bone marrow transplantation. T h e re-
ited a C R to other systemic treatment regimens. sults were positive in that the frequency of complete
Because of the potential merit of this therapy in the remission was high; however, the authors highlight
treatment of indolent lymphomas, studies are being the need for considerably longer patient follow-up
conducted to ascertain the role of bone marrow to determine the outcome of this treatment.
transplantation as primary therapy for such pa- Other reports describe favorable responses in pa-
tients. 67 While there is no clear evidence that bone tients with indolent non-Hodgkin's lymphomas
marrow transplantation cures indolent lymphomas, who receive autologous bone marrow transplanta-
it does provide long disease-free remissions. T h e jus- tion using purged marrow. For example, Freedman
tification for its use as part of primary therapy seems et al 72 at the Dana-Farber Cancer Institute reported
rational when one considers that the histologic 69 patients with low-grade non-Hodgkin's lym-
transformation to diffuse large-cell lymphomas seen phoma who received autologous bone marrow trans-
in patients with indolent disease has commonly been plantation during sensitive relapse or first partial
associated with a very poor prognosis. remission. They found that patients who received
Many issues remain to be resolved in the use of bone marrow transplants during complete remission
bone marrow transplantation for patients with low- had superior clinical outcomes compared with those
grade non-Hodgkin's lymphoma. T h e optimal treat- patients who exhibited active disease at the time of
ment regimen for such patients has not yet been transplantation. Optimistic results with autologous
determined. To date, most high-dose preparative bone marrow transplantation in the indolent non-
chemotherapeutic regimens have been accompa- Hodgkin's lymphomas have also been reported by
nied by total body irradiation due to the high sensi- Colombat et al, 73 Gribben et al, 74 and Schouten et
tivity of follicular non-Hodgkin's lymphomas to to- al. 75 Collectively, the results of these studies are en-
tal body irradiation. 68 In addition to the need to couraging; however, the authors of the reports al-
discover the optimal high-dose preparative regimen, most invariably highlight the fact that many ques-
it will also be crucial to delineate the optimal timing tions remain unanswered about autologous bone
of bone marrow transplantation as part of primary marrow transplantation in this clinical setting.
therapy or following relapse, just as it will be impor- Monoclonal antibodies. During the past 15 years,
tant to discern the best source of hematopoietic clinical investigators have explored the possible use
rescue. Undeniably, the critical question in regard to of monoclonal antibody-based therapies in the
bone marrow transplantation is related to ultimate treatment of non-Hodgkin's lymphomas. 76 To date,
outcome. 69 This question cannot be answered until more than 200 patients with various hematologic
additional clinical trials have been conducted and malignancies have been treated with unconjugated
carefully reviewed. Furthermore, allogeneic bone monoclonal antibodies. A m o n g these, more than 50
marrow transplantation appears to be curative in patients with low-grade B-cell non-Hodgkin's lym-
selected patients with small lymphocytic lym- phomas have received such therapy.77"83 T h e experi-
phoma/CLL. 7 0 In their study, Bandini et al 70 admin- ence with monoclonal antibody-based therapies for
istered high-dose cyclophosphamide and fraction- the indolent lymphomas is relatively limited, but it
SI-22 CLEVELAND CLINIC JOURNAL OF MEDICINE VOLUME 62 • SUPPLEMENT I
NON-HODGKIIM'S LYMPHOMAS • FISHER AND OKEN
does seem plausible that such an approach holds ing G 0 . Interferon alfa also inhibits the expression of
promise for these diseases. Nonetheless, to date it other genes, such as the c-nryc and c-fos oncogenes.
has not yielded strongly positive results. Perhaps an In fact, it has been proposed that I F N - a is a natural
explanation is that most of the patients who have tumor inhibitory agent. 88 Maintenance of the anti-
been treated thus far with monoclonal antibody- tumor effect of I F N - a requires continued drug expo-
based therapies had been enrolled in phase I clinical sure and results in a cytostatic form of tumor inhibi-
trials, had received extensive prior treatments, and tion. Because of the cytostatic-type of tumor
had malignancies that were refractory to conven- inhibition observed, rHuIFN-a is generally not
tional therapies. What has been learned is that curative in malignant diseases; however it does pro-
monoclonal antibodies can generally be adminis- duce prolonged remissions in a relatively safe and
tered safely to patients. Indeed, a number of indi- tolerable fashion in a variety of diseases. Although
viduals did exhibit transient clinical responses, and the role of rHuIFN-a in the treatment of non-
in some cases CRs occurred. Grossbard and Nadler 76 Hodgkin's lymphomas is not completely defined, a
appropriately state that future clinical trials will number of recent studies cited below provide sup-
need to include patients enrolled earlier in the port for its use, particularly in the indolent forms of
course of their disease—that is, before they have the disease.
developed tumor cell resistance to treatment and The earliest clinical trials were conducted before
organ damage from extensive prior chemotherapy the emergence of rHuIFN-a. The "crude" interferon
and/or irradiation. Moreover, the use of monoclonal was obtained from buffy coats of donated blood and
antibodies in patients with bulky tumor masses may therefore lacked the clear advantages of purity and
not be feasible. It is not unrealistic to project that reproducible activity associated with the recombi-
the probable role of monoclonal antibody therapy in nant form. Early on, Merigan's group91 reported fa-
treatment of patients with indolent non-Hodgkin's vorable results in patients with nodular poorly dif-
lymphoma may be to complement existing chemo- ferentiated lymphocytic lymphoma who received
therapy and radiation regimens. As sole therapy, it human leucocyte interferon with an initial dose of
seems rather unlikely that the use of monoclonal 2.5 million units (MU), which was escalated to 5
antibodies will provide cure in these patients. M U twice a day for 30 days. Shortly after that study
Recombinant interferon. Another promising ap- was published, Gutterman et al92 treated 11 lym-
proach to the treatment of low-grade non-Hodgkin's phoma patients with human leucocyte interferon;
lymphomas involves the administration of recombi- the results confirmed those obtained by Merigan et
nant human interferon alfa (rHuIFN-a). Numerous al91 and, more importantly, demonstrated that inter-
clinical and laboratory studies conducted during the feron treatment had obvious merit in patients who
past decade have substantiated the impression that were heavily pretreated and refractory to multiple
rHuIFN-a may be perceived as a mainstay in the chemotherapeutic regimens. Quesada et al93 were
treatment of a number of malignant diseases. 84-88 among the first to document the effects of rHuIFN-
The biologic and clinical effects of the interferons a in non-Hodgkin's lymphoma patients; in their
appear to be mediated through distinct cellular re- clinical study, 17 patients with nodular poorly differ-
ceptors. The overall antitumor efficacy of interferon entiated lymphocytic lymphoma who had received
lies partly in its antiproliferative and immunomodu- prior treatment were given sequentially escalating
latory actions. 89,90 Despite intensive laboratory in- doses of from 3 M U to 50 M U via intramuscular
vestigation during the past 20 years, the precise mo- injection on a daily basis for 8 weeks. Among the
lecular mechanism explaining the antiproliferative patients so treated, two exhibited C R s and four ex-
actions of interferon is unclear. Following internali- hibited partial responses (PRs). The CRs lasted for 6
zation of the interferon-receptor complex, inter- and 10 months, whereas the PRs lasted for 2, 4, 10,
feron present within the cell appears to modulate a and 12 months. Thus the study provided clear docu-
variety of biochemical processes by altering gene mentation of the efficacy of rHuIFN-a in nodular
expression. For instance, I F N - a inhibits expression poorly differentiated lymphocytic lymphoma.
of the gene for the enzyme ornithine decarboxylase. Other clinical trials were carried out with single-
Such an inhibitory effect on this key cellular regula- agent rHuIFN-a. 94 " 98 Collectively among these stud-
tory enzyme may explain the impact of interferon on ies, between 30% and 50% of patients with low-
cell-cycle slowing and arrested cellular division dur- grade non-Hodgkin's lymphoma exhibited an
VOLUME 62 • SUPPLEMENT I CLEVELAND CLINIC JOURNAL OF MEDICINES I - 37
NON-HODGKIN'S LYMPHOMAS • FISHER AND OKEN
objective clinical remission, with response rates ministered during midcycle while not incurring a
slightly higher among previously untreated patients. delay in the i n i t i a t i o n of t h e s u b s e q u e n t
Approximately 8% of all patients treated achieved a chemotherapeutic regimen. Patients were entered
C R . Of particular note, Foon et al95 demonstrated into the trial at three separate r H u I F N - a 2 a dose
that clinical responses to recombinant human inter- levels ranging from 2 MU/m 2 to 12 MU/m 2 . T h e
feron alfa-2a (rHuIFN-a2a) therapy could be ob- r H u I F N - a 2 a was administered during the last quar-
tained in patients with previous extensive treat- ter of the 21-day chemotherapy cycle. T h e authors
m e n t . T h i s suggested t h a t rHuIFN-tx2a is a noted that at the highest dose level of rHuIFN-a2a,
non-cross-resistant agent with chemotherapy drugs. the next cycle of C O P A therapy had to be delayed
O'Connell et al97 evaluated the response to rHuIFN- in six of 10 cycles because of significant neu-
a 2 a treatment in low-grade non-Hodgkin's lym- tropenia. Other than for an increase in the fre-
phoma patients who were previously untreated. quency of anemia noted in patients receiving the
A m o n g the nine patients with nodular poorly differ- combination, compared with historical controls re-
entiated lymphocytic lymphoma, four responses ceiving C O P A alone, there were no reports of un-
were obtained, including one C R , demonstrating anticipated toxicity. Overall, the results of this trial
clear antitumor activity utilizing an rHuIFN-a2a provided clinical support for previous observations
dose that was only 25% of the maximum tolerated on the potential benefit of r H u I F N - a 2 a in combi-
dose in the study. Notwithstanding the high clinical nation chemotherapy in animal models. Nonethe-
response rates associated with rHuIFN-a2a as single less, the work of Hawkins et al 101 could not be
therapy, investigators generally feel that rHuIFN- perceived as definitive because of the broad range
a 2 a alone does not represent optimal therapy in the of malignancies in patients enrolled in the clinical
indolent non-Hodgkin's lymphomas because it is trial as well as the small sample size and nominal
not curative. Accordingly, most recent clinical trials number of dose levels administered.
have focused on interferons in combination with Combination trials of r H u I F N - a and
chemotherapeutic agents. chemotherapeutics subsequent to the phase I and II
T h e pharmacologic rationale for combination studies described a b o v e typically employed
therapy with r H u I F N - a and chemotherapeutic chlorambucil or cyclophosphamide. 102 " 105 T h e study
a g e n t s c o n s t i t u t e s t h r e e e l e m e n t s : first, the by Rohatiner et al104 on administration of chloram-
chemotherapeutic agent's individual anticancer ac- bucil and recombinant human interferon alfa-2b
tivity; second, the seemingly distinct cellular (rHuIFN-a2b) to patients with recurrent low-grade
mechanisms of action of the agents; and third, the non-Hodgkin's lymphoma clearly demonstrated
lack of similar clinical toxicity profiles. T h e bio- that the use of this combination was clinically feasi-
logic rationale for the combination of r H u I F N - a ble; moreover, it provided clinical efficacy in pre-
and chemotherapeutic agents sprang from animal viously treated patients. Clinical responses to ther-
model studies as well as human tumor model sys- apy were observed in 14 of 23 patients enrolled in
tems in which r H u I F N - a was combined with cyclo- the trial; thirteen of these were PRs. In another
phosphamide 9 9 or doxorubicin. 1 0 0 In these studies, study, Chisesi et al103 treated 70 patients with low-
when r H u I F N - a was administered following cyto- grade non-Hodgkin's lymphoma. T h e patients re-
toxic agent-induced remission, prolonged survival ceived either chlorambucil (10 mg/day) or chloram-
was noted. bucil plus rHuIFN-a2b (5 MU/m 2 subcutaneously
Recombinant interferon combined with cKemo- three times per week). A total of 63 patients were
therapeutics. T h e feasibility of c o m b i n i n g a assessable for clinical response, and the study
chemotherapeutic agent with r H u I F N - a was dem- showed that similar response rates (62.1% and
onstrated in an early study by Hawkins et al. 101 64.7%, respectively) were recorded for the two
They conducted a phase I study of rHuIFN-a2a in treatment arms. More specifically, the patients were
combination with a C O P A regimen (cyclophos- randomly assigned to either chlorambucil ( 1 0
p h a m i d e , d o x o r u b i c i n , v i n c r i s t i n e , a n d pred- mg/day for 3 weeks, followed by 1 week of rest, then
nisone). T h e study included 19 patients with a va- resumption of chlorambucil for six additional cy-
riety of malignant diseases, including lymphoma. cles) or chlorambucil at 5 mg/day according to the
This clinical trial was intended to determine the same schedule in combination with rHuIFN-a2b
maximum dose of r H u I F N - a 2 a that could be ad- administered at 5 M U three times weekly. Those
SI-24 CLEVELAND CLINIC JOURNAL OF MEDICINE VOLUME 62 • SUPPLEMENT I
NON-HODGKIIM'S LYMPHOMAS • FISHER AND OKEN
patients who achieved a good PR or a C R were then of remission in patients with follicular lymphoma;
randomized to either no additional treatment or to 2 however, at the time of the report, no difference in
MU/m 2 rHuIFN-a2b for 3 weeks per month for a survival between treatment groups was noticeable.
duration of 6 months. Again, the clinical response The authors appropriately cite that additional ques-
rates were similar between the two arms, and there tions remain regarding the optimal dose and dura-
was no significant difference in the duration of re- tion of administration of maintenance rHuIFN-a2b
sponse. The authors cite that in patients who did in this disease.
respond, the clinical effects were slow but progres- The European Organization for Research and
sive, and toxicity did not increase with cumulative Treatment of Cancer has published its preliminary
doses. The authors noted that, comparing patients findings on 231 patients who responded to induc-
randomized to maintenance rHuIFN-a2b vs those tion C V P chemotherapy. 107 The patients were ran-
randomized to no further treatment, there was a domized to receive either maintenance rHuIFN-a2a
decrease in the relapse rate in the maintenance arm (3 MU/m 2 thrice weekly) or no maintenance
compared with the no-treatment arm. This study rHuIFN-a2a. The progression-free survival of those
would have benefited from a larger number of en- patients who received rHuIFN-a2a maintenance
rolled patients and a longer observation period; was 135 weeks compared with 86 weeks for those
however, it does provide the suggestion that low- patients who did not receive maintenance therapy.
dose maintenance rHuIFN-a might help to delay This was a statistically significant effect, although
relapse in chemotherapy-treated patients with his- the authors also note that there was no difference in
tologically confirmed low-grade non-Hodgkin's survival between treatment groups at the time of
lymphoma. publication of their preliminary report. 107 T h e
Price et al106 have reported their preliminary rHuIFN-a2a maintenance treatment in this study
analysis of the results of a clinical trial carried out at was very well tolerated, with only eight patients
St. Bartholomew's Hospital in London. This clinical having to stop treatment because of adverse reac-
study involved randomization of patients to tions to the rHuIFN-a2a.
chlorambucil alone or chlorambucil and rHuIFN- Several additional studies of combination ther-
a 2 b as primary therapy for stage III or IV follicular apy in patients with indolent non-Hodgkin's lym-
lymphoma. Patients in this trial who exhibited a phoma are noteworthy. The first study108 was con-
response to induction therapy were then rerandom- ducted at the University of Texas M. D. Anderson
ized to either maintenance rHuIFN-a2b therapy or Cancer Center (Houston) and reported 127 patients
no maintenance therapy at all. Of 124 treated pa- who had presented with stage IV low-grade non-
tients, 108 were assessable for clinical response, with Hodgkin's lymphoma. These previously untreated
a median follow-up period of 30 months. T h e patients were treated with cyclophosphamide, dox-
authors noted that myelosuppression was the major orubicin, vincristine, prednisone and bleomycin
toxic side effect and was more frequent with the ( C H O P - B l e o ) for 9 to 18 months (median 13
combination of rHuIFN-a2b and chlorambucil than months), followed by thrice weekly recombinant
it was with chlorambucil alone. During the entire human interferon alfa-nl ( r H u I F N - a n l ) (3
study, there was no treatment-related mortality, nor MU/m 2 ) for 24 months for those patients who had a
was there a statistically significant difference in CR. The authors report an overall response rate for
clinical response rates according to initial therapy. the entire treatment program (including addition of
Of particular interest, among the 60 patients who radiotherapy to residual lymph node masses) of 73%
exhibited a good response to initial therapy and CRs and 23% PRs. The 5-year survival for all 127
entered the second phase of the trial, the authors patients in their study was 74%. Among the group of
report a significant prolongation of the remission 109 patients with follicular histology, the 5-year sur-
period as a result of maintenance rHuIFN-(x2b. The vival of 73% did not significantly differ from the
duration of response was shortest in patients who 63% 5-year survival of the historical control group
had never received rHuIFN-a2b, and the fewest without rHuIFN-anl. The overall failure-free sur-
relapses were reported for those patients who re- vival at 5 years of the study group was 47%, and the
ceived rHuIFN-a2b throughout the study. Based on failure-free survival at 5 years of CRs was 60%. The
this preliminary analysis, the authors concluded that authors note that, compared with the findings in a
maintenance rHuIFN-a2b may extend the duration group of patients with similar pretreatment clinical
VOLUME 62 • SUPPLEMENT I CLEVELAND CLINIC JOURNAL OF MEDICINESI-37
NON-HODGKIN'S LYMPHOMAS • FISHER AND OKEN
features treated with CHOP-Bleo, these findings trial. Importantly, no treatment-related deaths were
represent a significant improvement for both fail- reported, and 71% of patients tolerated the combi-
ure-ffee survival overall as well as the failure-free nation therapy with rHuIFN-a2b well, receiving
survival of CRs. They conclude that the combina- treatment as scheduled. Recombinant human inter-
tion of r H u I F N - a n l and conventional chemother- feron alfa-2b administration had to be discontinued
apy with a CHOP-Bleo regimen is feasible and clini- because of reversible toxicity in approximately 11%
cally e f f e c t i v e . T h e y state t h a t m a i n t e n a n c e of the patients. Finally, the authors suggest that the
r H u I F N - a n l prolongs remission duration for pa- treatment regimen employed in this study should be
tients with stage IV low-grade lymphoma. However, compared with new and promising drugs such as
while these data appear relatively straightforward, fludarabine and 2-chlorodeoxyadenosine.
Coiffier 109 appropriately addresses significant draw- T h e Eastern Cooperative Oncology Group
backs of this study—for example, not all the pa- ( E C O G ) conducted a study 111 to evaluate the effects
tients had follicular lymphoma, and even fewer re- of adding rHuIFN-a2a to cytotoxic chemotherapy
quired treatment at the time of trial enrollment due as induction treatment in patients with clinically
to the absence of adverse prognostic factors. aggressive low-grade non-Hodgkin's lymphoma with
T h e report from the Multicenter Cooperative a poor prognosis, and in certain histologic variants
G r o u p e d'Etude des L y m p h o m e s de l ' A d u l t e of intermediate-grade non-Hodgkin's lymphoma,
(GELA) 1 1 0 is particularly noteworthy. Their study excluding patients with diffuse histiocytic lym-
was an open-label phase III clinical trial with 31 phoma. In this prospective randomized clinical trial,
participating medical centers in Europe. The study the c y t o t o x i c c h e m o t h e r a p e u t i c regimen was
e v a l u a t e d the potential merit of c o m b i n i n g C O P A . T h e patients were randomly assigned to the
rHuIFN-a2b with a regimen containing doxoru- C O P A regimen or a combination of C O P A and
bicin in a homogeneous group of patients with es- rHuIFN-a2a (I-COPA). Patients were to receive
tablished follicular non-Hodgkin's lymphoma and eight cycles of treatment, and those exhibiting a PR
accompanying large tumor burden. More specifi- or a C R during either cycle seven or eight were to
cally, the study involved 242 previously untreated receive two additional cycles. Following completion
patients with advanced low-grade follicular disease of the treatment period, the patients were evaluated
who were then treated with a regimen consisting of every 2 to 4 months for relapse. T h e results of this
cyclophosphamide, doxorubicin, teniposide, and E C O G cooperative trial demonstrated an overall
prednisone ( C H V P ) administered monthly for six response rate of 86% for the C O P A regimen with
cycles and then bimonthly for an additional 12 and without rHuIFN-a2a. Thus the two treatment
months. Following randomization, 119 patients re- regimens produced comparable objective clinical re-
c e i v e d this dose-reduced C H O P (cyclophos- sponses. However, the I-COPA regimen was associ-
p h a m i d e , d o x o r u b i c i n , v i n c r i s t i n e , and pred- ated with a prolongation of the time to treatment
n i s o n e ) - l i k e regimen only, while 123 patients failure and the duration of C R . T h e authors indicate
received the chemotherapeutic regimen plus 5 M U that addition of rHuIFN-a2a to the C O P A regimen
rHuIFN-a2b thrice weekly for 18 months. T h e re- provided an increased overall survival when the re-
sults of this study showed that the patients who were sults were adjusted for "important covariates." 111
administered a c h e m o t h e r a p e u t i c agent plus They conclude that the addition of rHuIFN-a to
rHuIFN-a2b had a significantly higher overall rate the C O P A chemotherapeutic regimen provided ef-
of response (85% vs 69%), a longer median event- fective antitumor activity in patients with clinically
free survival (34 months vs 19 months), and a aggressive low- or intermediate-grade non-
higher rate of survival at 3 years (86% vs 69%). T h e Hodgkin's lymphoma.
C R rate was less than that reported in previous trials
T h e C R rate in the E C O G study (32% for I-
of chemotherapy in the non-Hodgkin's lymphomas,
C O P A ) was actually lower than that obtained in
presumably because of the uniformly high tumor
previously published studies 111 of cytotoxic chemo-
burden and/or the diminished dose-intensity of the
therapy for indolent non-Hodgkin's lymphoma. A
chemotherapeutic regimen employed. Nonetheless,
possible explanation for this is that many of the
this is an important trial and effectively represents
patients had a poor prognosis due to the presence of
the first report of increased overall survival in favor
B symptoms (fever, night sweats, and weight loss)
of rHuIFN-a2b in a prospective randomized clinical
and bulky disease; also, some had intermediate-
SI-26 CLEVELAND CLINIC JOURNAL OF MEDICINE VOLUME 62 • SUPPLEMENT I
NON-HODGKIIM'S LYMPHOMAS • FISHER AND OKEN
grade disease. In a follow-up report, 112 Andersen and fit; in fact, the combination appeared to result only
Smalley indicate that at the 5-year treatment point, in increased toxicity.
81% of the patients assigned to the C O P A regimen A strict comparison of the G E L A , E C O G , and
and 66% of those assigned to the I-COPA regimen C A L G B (Cancer and Leukemia Group B) clinical
had disease progression and that time to treatment trials is complicated by the heterogeneity in trial
failure continued to be significantly prolonged by design. Collectively, more than 1200 assessable pa-
the addition of rHuIFN-a2a. The overall survival tients participated in the studies of rHuIFN-a as a
advantage initially reported, 111 however, diminished component of induction therapy with an established
on extended follow-up, and although the patients in chemotherapeutic regimen for patients with low-
the I-COPA group lived slightly longer than did grade non-Hodgkin's lymphoma. In these studies,
those in the group without interferon treatment, the extent of tumor burden varied, and previous
follow-up disclosed no statistically significant differ- treatment had been received by patients in the
ence between the survival curves in the two treat- C A L G B studies but not in the other two studies.
ment groups. It was concluded at the 5-year point Follow-up periods also varied from 2.7 years
that addition of interferon to induction therapy for ( C A L G B ) to 5.2 years ( E C O G ) , the chemo-
low- or intermediate-grade non-Hodgkin's lym- therapeutic regimens were not identical in the three
phoma does prolong the time to treatment failure; studies, and the rHuIFN-a doses varied consider-
however, it does not provide a significant improve- ably. Notwithstanding the heterogeneity of design
ment in the median 3- or 5-year survivals. among the three trials, however, at doses of 2 to 3
A n intergroup trial that compared cyclophos- MU/m 2 three times per week, rHuIFN-CX was gener-
phamide and cyclophosphamide plus rHuIFN-a2b ally well tolerated, although its addition to chemo-
in patients with follicular low-grade lymphomas in- therapy did increase toxicity. Addition of rHuIFN-a
cluded 581 patients enrolled over approximately 4 to standard chemotherapeutic regimens in the treat-
years.113 Of these, 474 eligible patients with pre- ment of follicular lymphoma is not curative, but it is
viously untreated low-grade stage III or IV follicular, associated with a prolongation of the time to treat-
small cleaved-cell, and follicular mixed lymphoma ment failure, although maximum tumor debulking
were randomized to induction therapy with cyclo- helps achieve optimal results.
phosphamide or cyclophosphamide plus rHuIFN- Interferon alfa does appear to have a significant
a2b. Treatment was administered for 3 months fol- role in maintenance therapy for patients with low-
lowing d o c u m e n t a t i o n of maximum clinical grade non-Hodgkin's lymphoma, as reported by
response (PR or C R ) . The clinical trial was later Price et al106 and Hagenbeek et al.107 There is no
amended to incorporate (for responders) an addi- definitive evidence that rHuIFN-a provides cure for
tional randomization to either 2 years of mainte- patients with low-grade non-Hodgkin's lymphoma,
nance rHuIFN-a2b or no additional treatment. The but prolongation of the time to treatment failure is
median follow-up time was 2.7 years. The prelimi- accomplished. These studies indicate that the ma-
nary data disclosed no significant difference in the jority of patients tolerate rHuIFN-a at doses of be-
overall response, survival, or time to treatment fail- tween 2 and 3 MU/m 2 three times per week. For
ure between the groups. T h e combination of cyclo- those patients with low-grade non-Hodgkin's lym-
phosphamide and rHuIFN-a2b consistently exhib- phoma who do not suffer from toxicity associated
ited greater toxicity than did cyclophosphamide with interferon therapy, therefore, the addition of
alone. Granulocyte counts < 1000 cells/mL occurred rHuIFN-a to the therapeutic armamentarium does
in 29% of patients treated with cyclophosphamide seem reasonable.
and in 57% of patients who received the combina-
tion therapy. Moreover, severe infections were re- New chemotherapeutic agents
ported to occur at twice the rate in the combined Although the indolent B-cell non-Hodgkin's
therapy group, and fever, neurotoxicity, thrombocy- lymphomas are generally responsive to chemother-
topenia, and other side effects were significantly apy, with between 30% and 80% of previously un-
more common with the combination treatment. treated patients achieving PR or C R to therapy, they
Adding rHuIFN-a2b to standard cyclophosphamide are fatal diseases. The median survival for low-grade
for induction therapy in patients with follicular low- non-Hodgkin's lymphoma is 7 to 10 years.114 Most
grade lymphomas had no substantial clinical bene- patients with these diseases will experience relapses
VOLUME 62 • SUPPLEMENT I CLEVELAND CLINIC JOURNAL OF MEDICINE SI-3 7
NON-HODGKIN'S LYMPHOMAS • FISHER AND OKEN
and will die of either an infectious complication synthesis and repair, including D N A polymerase al-
secondary to the disease or its treatment. T h e im- pha, D N A ligase I, and ribonuclease reductase. F-
pact of conventional chemotherapy, radiation ther- ara-A nucleotides are also incorporated into R N A . It
apy, or biologic agents on the low-grade lymphomas is possible that fludarabine incorporation into R N A
is limited by tumor-cell resistance. Although escala- represents a possible m e c h a n i s m of a c t i o n of
tion of chemotherapeutic dose or radiation may in fludarabine in the indolent non-Hodgkin's lym-
some cases overcome tumor-cell resistance, treat- phomas whereby a comparatively smaller proportion
ment-related toxicity may be unacceptable, particu- of cells are present in S phase. Other mechanisms of
larly because the median age of patients at the time action may be involved to explain the effects of
of diagnosis of an indolent lymphoma is greater than fludarabine in the non-Hodgkin's lymphomas as well
50 years, and many of these patients are unwilling to as other hematologic malignancies. 116
accept aggressive therapy. It is now appreciated that, Whelan et al 117 administered fludarabine as sin-
in many patients who achieve a "complete remis- gle-agent therapy to 34 patients with low-grade
sion," highly sensitive laboratory techniques can de- lymphoma and reported that, among these pre-
tect minimal residual disease. Accordingly, although viously treated patients, there were six complete
the initial clinical responses to treatment typically and seven partial responses to fludarabine—an
last for several years, virtually all patients will ulti- overall response rate of 38%. T h e E C O G study
mately relapse, and such relapses are associated with reported by Hochster et al 118 described the results of
a poor prognosis. New approaches to the treatment fludarabine administration to 62 assessable patients
of the indolent non-Hodgkin's lymphomas must be with relapsed and refractory non-Hodgkin's lym-
found. C o m b i n a t i o n therapy involving chemo- phoma, 27 of whom had low-grade histologic fea-
therapeutic agents and r H u I F N - a is encouraging, tures. T h e overall response rate was approximately
but additional studies on such combinations are re- 5 2 % . T h e principal toxicity a s s o c i a t e d with
quired to determine effects on overall survival. In fludarabine administration was myelosuppression.
the interim, much of the commercial focus on the Only six of the total 62 assessable patients exhib-
development of new pharmaceutical agents for the ited grade III or IV myelotoxicity in any treatment
treatment of these diseases has been directed toward cycle; however, six patients also exhibited grade III
developing analogues of existing drugs with en- neurotoxicity. In their phase II trial of fludarabine,
hanced pharmacologic activity, such as modifica- Redman et al 119 treated 38 patients with low-grade
tions of anthracyclines and alkylating agents. Sev- non-Hodgkin's lymphoma with fludarabine at a
eral p r o m i s i n g a g e n t s with apparently n o v e l dose slightly higher on a daily basis than that ad-
mechanisms of action have recently been studied: ministered during the E C O G study.118 T h e overall
fludarabine, 2'-deoxycoformycin (pentostatin), and response rate reported by Redman et al 119 was ap-
2-chlorodeoxyadenosine (cladribine). proximately 55% among patients with low-grade
Fludarabine. Fludarabine monophosphate is an non-Hodgkin's lymphoma. S e v e n of the 38 patients
adenine nucleoside that may have considerable experienced sufficient myelosuppression (after a
value in treating the indolent non-Hodgkin's lym- median treatment duration of five courses) to dis-
phomas. It has been shown to possess activity in continue fludarabine therapy, although, among
multiple animal tumor systems, including C D 8 S , these patients, five had previous bone marrow in-
mammary adenocarcinoma, P388 leukemia, L I 210 volvement. There was no evidence of neurotoxicity
leukemia, and human LX-1 lung tumor xenograft. 115 in this trial.
Following intravenous administration, fludarabine is Taken as a group, the phase I and II studies con-
rapidly dephosphorylated in plasma to form 2-fluoro- ducted to date suggest that fludarabine is a signifi-
arabinofuranosyl-adenine (2-F-ara-A). This dephos- cant new agent in the management of low-grade
phorylated intermediate enters cells via both high- non-Hodgkin's lymphoma. Overall response rates
and low-affinity transport systems, where it is sub- are encouraging, even though myelosuppression en-
sequently phosphorylated by the enzyme deoxycyti- countered even at low doses is a common problem.
dine kinase to fluoro-arabinofuranosyl-adenosine Fludarabine is immunosuppressive, and its use has
triphosphate (F-ara-ATP). T h e F-ara-ATP is incor- been associated with an increased risk of infec-
porated into D N A and inhibits D N A synthesis as tion. 120 Approximately one in five patients receiving
well as a variety of enzymes that have roles in D N A fludarabine exhibits some sign of neurotoxicity,
SI-28 CLEVELAND CLINIC JOURNAL OF MEDICINE VOLUME 62 • SUPPLEMENT I
NON-HODGKIIM'S LYMPHOMAS • FISHER AND OKEN
which is typically mild and reversible. The lack of reported two PRs in the 12-patient group with the
activity of fludarabine in intermediate- and high- low-grade histology, approximately a 17% overall
grade lymphoma is somewhat surprising in view of response rate.
the diversity of key cellular proliferation enzymes To date there have been CRs in 8% and PRs in
that appear to be affected by fludarabine. A recent 20% of patients treated with DCF for low-grade
report from Italy,121 however, suggests that mainte- non-Hodgkin's lymphoma, with a median duration
nance rHuIFN-a may prolong remissions after treat- of 6 months. Myelosuppression with grade IV neu-
ment with fludarabine in patients with low-grade tropenia has been seen in 5%, and grade IV throm-
non-Hodgkin's lymphoma. bocytopenia has been seen in approximately 14% of
2'-Deoxycoformycin. Pentostatin, or 2'-deoxyco- DCF-treated patients. Activity of DCF in previously
formycin (DCF), is a natural product isolated from untreated patients with low-grade non-Hodgkin's
Streptomyces antibioticus. It closely resembles hypox- lymphoma is undefined. In general, DCF has consid-
anthine and is a structural analogue of the purine erably greater activity in hairy cell leukemia than in
adenosine; it is also structurally related to the non-Hodgkin's lymphomas.
fludarabine and 2-chlorodeoxyadenosine. 122 2'-De- 2'Chlorodeoxyadenosine. The molecular structure
oxycoformycin is a very potent, irreversible inhibi- of cladribine, or 2-chlorodeoxyadenosine (2-CdA),
tor of adenosine deaminase ( A D A ) , which catalyzes is identical to that of deoxyadenosine with the ex-
the irreversible deamination of adenosine and de- ception of the substitution of a chlorine atom for a
oxyadenosine to form inosine and deoxyadenosine hydrogen atom at position 2 of the purine ring of
in the purine salvage pathway. Adenosine deami- deoxyadenosine, the natural substrate for ADA. 1 2 5
nase is widely distributed in mammalian tissue with The cellular mechanism of action of 2-CdA is not
particularly high levels in T and B lymphocytes. well understood, although it is believed to cause
Children congenitally deficient in A D A exhibit se- D N A strand breaks that in turn activate
rious defects in lymphocyte function, manifested as poly(adenosine diphosphate-ribose) polymerase, re-
a severe combined immunodeficiency syndrome. sulting in depletion of nicotinamide adenine dinu-
The association of this enzyme deficiency with de- cleotide, with accompanying cell death. T h e en-
fective lymphocyte function led to the development zyme deoxycytidine kinase catalyzes the
of D C F and related compounds as immunosuppres- intracellular phosphorylation of 2-CdA to 2-chlo-
sive and lymphocytotoxic drugs.122 Apparently most rodeoxyadenosine triphosphate, which is known to
of the biochemical effects of DCF that are conse- inhibit D N A synthesis in replicating cells and is also
quences of A D A inhibition are more germane to cytotoxic to lymphocytes and monocytes. 126,127 Evi-
proliferating cells, leaving the mechanistic basis of dence suggests128 that 2-CdA is cytotoxic to nonrep-
DCF in the indolent lymphomas uncertain. 2'-De- licating cells by triggering programmed cell death
oxycoformycin has a variety of actions within the (apoptosis) in malignant lymphocytes. 128
cell, including the inhibition of messenger R N A Clinical experience with 2-CdA in the treatment
synthesis for interleukin-2. It is likely that multiple of patients with low-grade non-Hodgkin's lym-
cell regulatory effects associated with D C F form the phoma is limited. Kay et al129 reported results in 40
basis of its antineoplastic activity. patients who had failed a median of three prior
The first cooperative group study demonstrating standard chemotherapeutic regimens; 20% achieved
activity of D C F in patients with lymphoma was a a CR, and 23% a PR. The median response duration
C A L G B phase II trial reported by Duggen et al.123 was approximately 5 months; however, among the
The efficacy of single-agent DCF in this study was eight patients achieving a C R , four remained in
relatively low ( C R plus PR = 29%); however, toxic- continuous C R at 2, 12, 29, and 33 months. The
ity was acceptable and there was no treatment-re- overall response rate (43%) is encouraging. How-
lated mortality reported. Shortly after, Cummins et ever, side effects were relatively common, with grade
al124 reported on their phase II trial of D C F in refrac- III to IV thrombocytopenia in 30% and grade III to
tory lymphoma and C T C L . This E C O G study in- IV neutropenia in 18% of patients. In patients with
volved the treatment of 22 relapsed and refractory intermediate- and high-grade non-Hodgkin's lym-
patients with various histologic pictures of non- phoma, 130 combinations of 2 - C d A with various
Hodgkin's lymphoma. The D C F dose administered chemotherapeutic agents may result in improved
was 5 mg/m2/day for 3 days every 3 weeks; the study clinical response rates.
VOLUME 62 • SUPPLEMENT I CLEVELAND CLINIC JOURNAL OF MEDICINES I - 37
NON-HODGKIN'S LYMPHOMAS • FISHER AND OKEN
Stage I or II aggressive lymphoma with approximately 30% of all treated patients ex-
According to the Working Formulation, 7 the in- periencing a sustained CR. 3,132
termediate-grade lymphomas comprise four diseases: A s mentioned above, there is no universally ac-
follicular predominantly large-cell, diffuse small cepted treatment regimen for intermediate-grade
cleaved-cell, diffuse mixed small- and large-cell, and non-Hodgkin's lymphomas. Many patients with
diffuse large-cell lymphomas. Although immuno- stage I or II disease have microscopic spread of the
blastic lymphoma is categorized in the Working For- disease to distant sites; therefore, combination che-
mulation as a high-grade neoplasm, it is commonly motherapy is considered standard treatment. Pa-
treated as an intermediate-grade tumor. These five tients who present with regional disease may bene-
diseases have many clinical characteristics in com- fit from combination chemotherapy (eg, C H O P )
mon. Follicular predominantly large-cell tumors be- and regional radiotherapy. It is not known, how-
have clinically in a fashion similar to that of the ever, whether regional radiation therapy is a neces-
diffuse large-cell lymphomas. Many follicular pre- sary adjuvant to multiagent chemotherapy in stage
dominantly large-cell tumors undergo conversion to I or II disease. In the nonrandomized study reported
diffuse large-cell lymphomas in the absence of cura- by Jones et al, 133 8 of 34 patients (24%) treated with
tive treatment. Diffuse small cleaved-cell lym- a C H O P regimen alone relapsed, compared with 15
phomas are problematic for a variety of reasons, of 108 patients (14%) who received C H O P fol-
including the fact that many patients presenting lowed by local radiation therapy. Mauch et al 134 in a
with this form of lymphoma are elderly and com- retrospective study reported improved survival fol-
monly exhibit stage IV disease at initial presenta- lowing c o m b i n e d chemotherapy and radiation
tion; it is not unusual for such patients to present therapy in patients with stage I-II non-Hodgkin's
with extensive bone marrow, liver, spleen, and pul- lymphoma. T h e authors reported a lower freedom-
monary tumor infiltration. T h e diffuse mixed small- ffom-progression rate (43% vs 6 6 % ) and survival
and large-cell variety of intermediate-grade non- rate (56% vs 8 0 % ) in patients treated only with
Hodgkin's lymphoma behaves similarly to the dif- chemotherapy. This was the case even when pa-
fuse large-cell lymphomas and commonly involves tient subgroups were stratified according to histol-
elderly women, who present with extranodal disease ogy, disease stage, and chemotherapy. By contrast,
involvement of the gastrointestinal tract and skin. other studies 135,136 do not disclose a substantial ad-
T h e most commonly encountered intermediate- vantage of radiation therapy to previously involved
grade lymphoma is the diffuse large-cell variety, a sites.
particularly invasive form of lymphoma that may
Tondini et al137 provide encouraging data on the
produce compression of major blood vessels and air-
combination of primary C H O P chemotherapy fol-
ways. Patients typically present with enlarged cervi-
lowed by local irradiation of patients with stage I and
cal lymph nodes or prominent extranodal disease in
II histologically aggressive lesions. This single-cen-
the gastrointestinal tract, skin, bone, brain, and
ter, prospective, nonrandomized clinical study in-
other organs. A t initial presentation, tumor infiltra-
volved 183 patients with stage I or II nodal and
tion of bone marrow occurs in less than 20% of
extranodal lymphomas with no more than three sites
patients; however, its presence is an omen of disease
of disease involvement. Treatment included four cy-
spread to the central nervous system ( C N S ) . Ac-
cles of C H O P chemotherapy (six cycles in partial
cordingly, spinal fluid analysis is important in pa-
responders). Radiation therapy to initial sites of dis-
tients with bone marrow infiltration.
ease involvement and to proximal uninvolved nodal
A wide variety of multiagent chemotherapeutic regions was administered promptly following com-
regimens are available for treatment of intermedi- pletion of administration of the chemotherapeutic
ate-grade lymphomas. 59,131 Little evidence suggests regimen. T h e authors reported a C R rate of 98% at
that any chemotherapeutic regimen is superior to the end of the combined therapy. After a median
the others. T h e C H O P regimen is the most widely follow-up period of more than 4 years, 26 patients
used in the treatment of diffuse large-cell non- had relapsed and 25 had died. The 5-year relapse-free
Hodgkin's lymphoma. Long-term follow-up data and total survival rates were 83%. With the excep-
from the Southwest Oncology Group ( S W O G ) for tion of age greater than 60 years, other factors, in-
several studies employing the C H O P regimen dis- cluding disease stage, histology, presence of extrano-
closed a complete remission rate of more than 50%, dal lesions, bulky lymphoma, or elevated L D H , were
SI-30 CLEVELAND CLINIC JOURNAL OF MEDICINE VOLUME 62 • SUPPLEMENT I
NON-HODGKIIM'S LYMPHOMAS • FISHER AND OKEN
not predictive of treatment outcome. The authors M A C O P - B (methotrexate with leucovorin rescue,
reported a trend toward higher relapse rates for pa- doxorubicin, cyclophosphamide, vincristine, pred-
tients achieving C R at the time of radiation therapy nisone, and bleomycin), and m - B A C O D (methotr-
(31%) compared with those achieving C R with che- exate with leucovorin rescue, bleomycin, doxoru-
motherapy (15%) or with initial surgery (10%). bicin, cyclophosphamide, vincristine, and
They also mentioned that the treatment was well dexamethasone). Some commonly used
tolerated, with no deaths due to acute toxicity. They chemotherapeutic regimens, their typical doses,
concluded that patients who present with limited- routes, and administration schedules are presented
stage aggressive non-Hodgkin's lymphomas may be in Table 5. As a group, these chemotherapy programs
safely and effectively treated with a short course of were associated with approximately 70% to 75% C R
C H O P followed by local radiation therapy; this ap- rates and approximately 50% long-term survival
proach is curative for most such patients and should rates.131 Unfortunately, these regimens were also
be regarded as standard therapy for these patients. commonly associated with greater toxicity, particu-
Although these studies do not provide evidence of larly bone marrow depression and severe mucositis.
the definitive effects of adjuvant radiotherapy fol- In addition, the cost of these treatment regimens is
lowing effective chemotherapy for patients with substantial.
early-stage histologically aggressive non-Hodgkin's Reports from several large lymphoma-referral
lymphoma, randomized clinical trials are in progress centers in the United States indicated that use of
to clarify the impact of combined chemotherapy and second- and third-generation chemotherapeutic
radiation therapy. regimens was accompanied by C R rates of up to 85%
and predicted long-term survival rates as high as
Stage III or IV aggressive lymphoma 65%. 131 Despite enthusiasm, there was concern that
The treatment of choice for all patients with these pilot studies overestimated the relative merit
stage III or IV intermediate-grade non-Hodgkin's of the second- and third-generation regimens. Some
lymphoma is combination chemotherapy. The first- of the studies involved comparison of their clinical
generation chemotherapeutic regimens, developed results with historical data from large cooperative
between 1965 and 1975, typically included four or group studies despite the fact that the study popula-
five chemotherapeutic agents. Their administration tions were heterogeneous. Also, some of the studies
resulted in CRs in 45% to 55% of patients and at single institutions involved short follow-up peri-
achieved cure in approximately 30% to 35%.42,138~140 ods; more extensive follow-up disclosed a substantial
These regimens include CHOP, B A C O P (bleomy- increase in late relapses as well as deaths.
cin, doxorubicin, cyclophosphamide, vincristine, To conduct a valid comparison of these
and prednisone), C-MOPP, and C O M L A (cyclo- chemotherapeutic regimens, the S W O G initiated a
phosphamide, vincristine, methotrexate with leuco- prospective randomized phase III clinical trial com-
vorin rescue, and cytarabine). Of these, C H O P paring CHOP, m-BACOD, ProMACE-CytaBOM,
emerged as standard therapy for patients with ad- and M A C O P - B regimens for the treatment of pa-
vanced-stage intermediate- or high-grade non- tients with intermediate-grade or high-grade non-
Hodgkin's lymphoma. During the late 1970s and Hodgkin's lymphoma. 141 Approximately 2 years after
early-to-mid 1980s, oncologists and hematologists study initiation, the E C O G joined the study, desig-
attempted to improve the C R and cure rates in these nated the N a t i o n a l High-Priority Lymphoma
diseases by administration of more intensive Study.141 The end points of this clinical trial were
chemotherapeutic regimens incorporating between response rate, time to treatment failure, overall sur-
six and eight separate drugs. These second- and vival, and incidence of severe or life-threatening
third-generation regimens include P r o M A C E - toxicity. A total of 1138 patients registered for this
CytaBOM (prednisone, methotrexate, doxorubicin, clinical trial, of whom 899 were determined to be
cyclophosphamide, and etoposide, followed by eligible; each treatment group contained at least
cytarabine, bleomycin, vincristine, and methotr- 218 patients. Randomization was stratified accord-
exate with leucovorin rescue), ProMACE-MOPP ing to several factors, including the presence of bone
(prednisone, methotrexate, doxorubicin, cyclophos- marrow infiltration or bulky disease, L D H levels
phamide, and etoposide alternating with nitrogen above or below 250 U/L, age (< 65 vs > 65 years),
mustard, vincristine, procarbazine, and prednisone), and Working Formulation group. The results of this
VOLUME 62 • SUPPLEMENT I CLEVELAND CLINIC JOURNAL OF MEDICINES I - 37
NON-HODGKIN'S LYMPHOMAS • FISHER AND OKEN
TABLE S
CHEMOTHERAPEUTIC REGIMENS
Regimen Dose and route Day Frequency
CVP Every 21 days
C: Cyclophosphamide 400 mg/m22 PO 1-5
V: Vincristine 1.4 mg/m 1
P: Prednisone 100 mg/m2 PO 1-5
C-MOPP Every 28 days
C: Cyclophosphamide 650 mg/m22 IV 1, 8 days
O: Vincristine 1.4 mg/m 2 IV 1,8
P: Procarbazine 100 mg/m PO 1-14
P: Prednisone 40 mg/m PO 1-14
BACOP Every 28 days
B: Bleomycin 5 mg/m2 IV 15, 22
A: Doxorubicin 25 mg/m2 2IV 1,8
C: Cyclophosphamide 650 mg/m2 IV 1,8
O: Vincristine 1.4 mg/m IV 1,8
P: Prednisone 60 mg/m2 PO 15-28
CHOP 2
Every 21 days
C: Cyclophosphamide 750 mg/m IV 1
H: Doxorubicin 50 mg/m22IV 1
O: Vincristine 1.4 mg/m IV (maximum 2.0 mg) 1
P: Prednisone 100 mg PO 1-5
COMLA 2
Every 91 days
C: Cyclophosphamide 1500 mg/m IV 1
2
O: Vincristine 1.4 mg/m 2 IV (maximum 2.0 mg) 1,8, 15
M: Methotrexate* 120 mg/m IV 36, 43, 50, 57, 64, 71
L: Leucovorin 25 mg/m2 2PO x 4 24 hours after methotrexate
A: Cytarabine 300 mg/m Same as methorexate
COP/BLAM 2
Every 21 days
C: Cyclophosphamide 400 mg/m IV 1
O: Vincristine 1 mg/m2 2IV 1
P: Prednisone 40 mg/m2 PO 1-10
BL: Bleomycin 15 mg/m IV 15
A: Doxorubicin 40 mg/m2 2IV 1
M: Procarbazine 100 mg/m PO 1-10
M-BACOD Every 21 days
M: Methotrexate* 3000 mg/m IV 15
B: Bleomycin 4 mg/m2 2IV 1
A: Doxorubicin 45 mg/m 2IV 1
C: Cyclophosphamide 600 mg/m IV 1
O: Vincristine 1 mg/m22 IV 1
D: Dexamethasone 6 mg/m PO 1-5
m-BACOD Every 21 days
m: Methotrexate* 200 mg/m2 IV 8, 15
B: Bleomycin 4 mg/m2 2IV 1
A: Doxorubicin 45 mg/m 2IV 1
C: Cyclophosphamide 600 mg/m2 IV 1
O: Vincristine 1.0 mg/m IV 1
D: Dexamethasone 6 mg/m2 PO 1-5 Continued
intergroup study demonstrated no significant differ- group at 3 years was 52% ( P r o M A C E - C y t a B O M
ence among the treatment groups in the rates of and M A C O P - B were 50%, C H O P was 54%, and
objective antitumor responses, PRs, or CRs. 1 4 2 A t 3 m - B A C O D was 52%). There was no subgroup of
years, 44% of all patients enrolled in the trial were patients in which survival was improved by admini-
alive without disease (41% for C H O P and MA- stration of a third-generation regimen. T h e inci-
C O P - B , 4 6 % for m - B A C O D and P r o M A C E - dence of fatal toxic reactions was least in the C H O P
C y t a B O M regimens). Overall survival for the entire group (1%). Fatal toxicity associated with admini-
SI-32 CLEVELAND CLINIC JOURNAL OF MEDICINE VOLUME 62 • SUPPLEMENT I
NON-HODGKIIM'S LYMPHOMAS • FISHER AND OKEN
TABLE 5
CHEMOTHERAPEUTIC REGIMENS* (Continued)
Regimen Dose and route* Day Frequency
ProMACE-MOPP Every 28 days
Pro: Prednisone 60 mg/m PO 1-14
M: Methotrexate* 1500/m2 2IV 15
A: Doxorubicin 25 mg/m 2IV 1, 8
C: Cyclophosphamide 650 mg/m IV 1, 8
E: Etoposide 120/mg/^IV 1,8
Followed by MOPP after maximal response
M: Mechlorethamine 6 mg/m IV 1, 8 Every 28 days
O: Vincristine 1.4 mg/m22IV 1, 8
P: Procarbazine 100 mg/m PO 1-14
P: Prednisone 40 mg/m2 PO 1-14
ProMace-CytaBOM Every 21 days
Pro: Prednisone 60 mg/m22 PO 1-14
A: Doxorubicin 25 mg/m 2IV 1
C: Cyclophosphamide 650 mg/m2 IV 1
E: Etoposide 120 mg/m IV 1
Cyta: Cytarabine 300 mg/m2 IV 8
B: Bleomycin 5 mg/m2 IV 8
O: Vincristine 1.4 mg/m22 IV 8
M: Methotrexate* 120 mg/m IV 8
ProMACE dUMOPP d8 Every 28 days
Pro: Prednisone 60 mg/m2 2PO 1-14
M: Methotrexate* 500 mg/m IV 15
A: Doxorubicin 25 mg/m2 2IV 1
C: Cyclophosphamide 650 mg/m2 IV 1
E: Etoposide 120 mg/m IV 1
M: Mechlorethamine 6 mg/m2 IV 8
O: Vincristine 1.4 mg/m22IV 8
P: Procarbazine 100 mg/m POd
MACOP-B 8-14 Every 84 days
2
M: Methotrexate* 400 mg/m IV
A: Doxorubicin 50 mg/m2 2IV 8, 36, 64
C: Cyclophosphamide 350 mg/m IV
O: Vincristine 1.4 mg/m IV (maximum 2.0 mg) 1, 15, 29, 43, 57, 71
P: Prednisone 75 mg/m22 PO 1, 15, 29,43, 57,71
B: Bleomycin 10 mg/m IV 8, 22, 36, 64, 78
1-84
22, 50, 78
Reprinted from Gaynor and Fisher, reference 3, with permission
*IV, intravenous; PO, by mouth; POd, by mouth dally
Leucovorin rescue Is given 24 hours after each methotrexate dose; dose duration and schedule differ in each protocol
stration of ProMACE-CytaBOM, m - B A C O D , and were combined, statistically significant differences
M A C O P - B was 3%, 5%, and 6%, respectively. T h e were found among the regimens, with C H O P and
toxic reactions that were reported were similar to P r o M A C E - C y t a B O M less toxic than m - B A C O D
those documented in previous phase II trials of the and M A C O P - B (P = .01).
same regimens. T h e most severe reactions were asso- T h e National High-Priority Lymphoma Study
ciated with granulocytopenia and resultant infec- was designed to detect a 15% difference in treat-
tion. There was no statistical significance between ment failure rates between C H O P and the third-
the incidence rates of fatal (grade V) toxic reactions generation regimens. Additional follow-up of the
among the treatment groups. In contrast, grade IV patients in this clinical study is unlikely to demon-
(life-threatening) toxic reactions were recorded in strate that any of the third-generation
31% of patients receiving CHOP, 29% of those re- chemotherapeutic regimens included actually re-
ceiving ProMACE-CytaBOM, 43% of those receiv- duces the treatment failure rate by 15% compared
ing M A C O P - B , and 54% of those receiving m-BA- with standard C H O P therapy. T h e authors con-
C O D regimens. When grades IV and V reactions cluded that C H O P remains the best available treat-
VOLUME 62 • SUPPLEMENT I CLEVELAND CLINIC JOURNAL OF MEDICINE SI-3 7
NON-HODGKIN'S LYMPHOMAS • FISHER AND OKEN
ment for patients with advanced-stage intermedi- men is used to identify patients with sensitive vs
ate- or high-grade non-Hodgkin's lymphoma. resistant relapse. Existing data do not indicate
T h e results of the National High-Priority Lym- whether patients with resistant or relapsed aggres-
phoma Study indicate that approximately 55% to sive lymphoma can be cured with the available sal-
65% of patients with advanced-stage intermediate- vage combination regimens. A n ongoing random-
or high-grade non-Hodgkin's lymphoma will be ized prospective multinational clinical trial 142 is
either refractory to multiagent chemotherapeutic studying the potential value of high-dose chemo-
regimens or will relapse following initial combina- therapy followed by bone marrow transplantation
tion chemotherapy. 141 S o m e patients resistant to for relapsed patients responsive to conventional
standard chemotherapeutic or salvage regimens may D H A P salvage therapy.
achieve a complete remission when administered In patients with intermediate- or high-grade non-
very high doses of chemotherapy or combined che- Hodgkin's lymphoma, prolongation of disease-free
m o t h e r a p y and radiation, a l t h o u g h these ap- survival appears to be similar with either autologous
proaches tend to be associated with profound and ( A B M T ) or allogeneic bone marrow transplanta-
life-threatening myelosuppression. Alternative ap- tion. 143 Because A B M T appears to be more advanta-
proaches in refractory or relapsed patients may be geous when the procedure is carried out earlier in
autologous bone marrow transplantation ( A B M T ) the course of the disease, a number of physicians are
or, in applicable cases, transplantation using bone attempting to use high-dose chemotherapy com-
marrow obtained from an HLA-matched relative or bined with A B M T as primary treatment for patients
an identical twin. Complete response or even cure is with intermediate- or high-grade non-Hodgkin's
more likely among patients who exhibit a favorable lymphoma. 144 " 147 Data to date indicate disease-free
response to initial combination chemotherapy and survival of 60% to 90% at 2- or 3-year time points
who, at the time of bone marrow transplantation, for patients with poor prognoses.
possess no residual tumor or minimal residual dis-
ease and have had a favorable response to salvage High-grade lymphoma
chemotherapy. Patients who exhibit progressive dis- According to the Working Formulation, three
ease o n salvage therapy prior to bone marrow trans- diseases constitute the high-grade non-Hodgkin's
plantation are unlikely to benefit, as are patients lymphomas: large-cell immunoblastic, lymphoblas-
who failed or responded poorly to initial therapy. tic, and small noncleaved-cell lymphomas. Im-
Bone marrow transplantation is not universally munoblastic lymphoma (diffuse histiocytic variety
applicable to patients with relapsed or refractory in the R a p p a p o r t C l a s s i f i c a t i o n ) is c o m m o n l y
aggressive non-Hodgkin's lymphoma. Patients with treated as an intermediate-grade lesion. Lym-
bone marrow involvement or of advanced age and phoblastic lymphoma represents a unique subgroup
generally poor medical condition will not be suit- of the non-Hodgkin's lymphomas, exhibiting clini-
able candidates for transplantation. Such patients cal behavior reminiscent of T-cell acute lympho-
are typically administered conventional-dose sal- cytic leukemia, manifesting early and widespread
vage chemotherapy. Objective recommendation of dissemination with frequent bone marrow involve-
a particular salvage regimen is difficult because of ment and C N S metastasis. Although lymphoblastic
the absence of randomized, prospective clinical tri- lymphoma and small noncleaved-cell lymphoma
als in patients with aggressive non-Hodgkin's lym- share a number of similar clinical characteristics,
phoma. Nevertheless, salvage regimens have been virtually all lymphoblastic lymphomas are of the
proposed, incorporating drugs that have for the most T-cell variety, whereas small noncleaved-cell lym-
part not been employed in initial chemotherapy. 131 phoma is a B-cell disorder. T h e high-grade non-
Generally speaking, approximately 20% to 35% of Hodgkin's lymphomas have a very poor prognosis
patients exhibiting an initial C R will achieve a sec- and demand aggressive treatment, most commonly
ond C R with salvage chemotherapy. D H A P (dex- with high-dose combination chemotherapy accom-
amethasone, high-dose ara-C, and cisplatin) has panied by C N S prophylaxis. Irrespective of the par-
consistently been associated with C R rates in 15% ticular chemotherapy regimen employed, it is im-
to 3 0 % of cases. This regimen is commonly used portant for the physician to pay particular attention
before bone marrow transplantation in an attempt to the general clinical care of the patient, renal and
to debulk tumor; the response to the D H A P regi- hepatic function, electrolyte balance, and degree of
SI-34 CLEVELAND CLINIC JOURNAL OF MEDICINE VOLUME 62 • SUPPLEMENT I
NON-HODGKIIM'S LYMPHOMAS • FISHER AND OKEN
hydration. Although drug-related toxicity will vary modified to initiate C N S prophylaxis earlier and
depending upon the selection of the chemo- also to incorporate cranial radiotherapy. Their regi-
therapeutic regimen, the dose-limiting toxicity most men, which involved induction, consolidation, and
commonly encountered is myelosuppression. Pa- maintenance phases in addition to C N S prophylaxis
tients presenting at any time in their disease course with intrathecal methotrexate and cranial radia-
with fewer than 1000 granulocytes/mm 3 and fever tion, produced encouraging results. Of 44 patients
must be immediately hospitalized and treated with assessable for treatment response, two achieved a PR
broad-spectrum antibiotics. When platelet counts and 42 achieved a C R . The studies149,150 carried out
drop below 20 000/mm 3 , platelet transfusion is indi- to date demonstrate that leukemia-like treatment
cated. regimens that involve intensive induction, consoli-
A variety of chemotherapeutic regimens have dation, and maintenance phases in addition to C N S
been employed in the treatment of patients with prophylaxis provide considerable clinical benefit to
lymphoblastic lymphoma 148 " 151 and small non- a substantial number of patients with adult lym-
cleaved-cell lymphoma. 152 " 154 T h e regimen de- phoblastic lymphoma, although the need remains
scribed by Coleman et al150 was associated with the for novel approaches affording even better rates of
highest rate of C R (95%). Their study involved CR, disease-free survival, and overall survival.
induction therapy with a regimen consisting of cy- Studies evaluating various chemotherapeutic
clophosphamide, doxorubicin, vincristine, pred- regimens for the treatment of small noncleaved-cell
nisone, and asparaginase and maintenance therapy lymphoma have provided encouraging results.151"153
involving methotrexate and 6-mercaptopurine. Complete response rates have been approximately
Three-year disease-free survival was 56% in pa- 80%, with disease-free survival rates at 1- to 5-year
tients so treated. The patients in this study also treatment points in the range of 60% to 70%. The
received C N S prophylaxis of intrathecal and high- regimens employed have included, among others,
dose systemic methotrexate and cranial radiother- combinations of cyclophosphamide, vincristine,
apy. Levine et al149 used a more complicated regi- bleomycin, doxorubicin, methotrexate, etoposide,
men involving, for induction, cyclophosphamide, and prednisone, with or without intrathecal
doxorubicin, vincristine, prednisone, cytarabine, methotrexate as C N S prophylaxis, 154 and cyclophos-
thioguanine, asparaginase, and lomustine, and, for phamide, doxorubicin, vincristine, prednisone, and
maintenance, thioguanine, cyclophosphamide, hy- methotrexate, including intrathecal methotrexate
droxyurea, methotrexate, lomustine, doxorubicin, as C N S prophylaxis. 152 In the latter study,152 radia-
cytarabine, and vincristine. Patients received C N S tion therapy was also provided to all bulky unre-
prophylaxis consisting of intrathecal methotrexate sected masses.
and cranial radiotherapy. These patients also re- When patients present with extensive infiltra-
ceived irradiation to the mediastinum. The rate of tion of the bone marrow ( > 2 5 % blasts), it is appro-
C R was 73%, and disease-free survival at 5 years priate to administer acute lymphoblastic leukemia-
was 35%. type chemotherapeutic regimens. 151,155,156 As
The expanded chemotherapeutic regimens em- mentioned, some patients with aggressive non-
ployed by Coleman et al150 and Levine et al149 in Hodgkin's lymphomas also experience metabolic
patients with lymphoblastic lymphoma represent complications—for example, elevated serum uric
considerable improvement over previous attempts acid and increased serum creatinine related to tu-
to use C V P or CHOP-Bleo regimens, frequently in mor lysis syndrome or uric acid nephropathy. The
combination with radiation therapy, by which the tumor lysis syndrome is usually associated with rapid
median survival of patients was only approximately clinical responses in patients exhibiting bulky dis-
15 months. Central nervous system prophylaxis was ease. Adequate hydration, alkalinization of the
included in these studies because of the experience urine, and prophylactic allopurinol are commonly
originally reported by the Stanford group (Coleman used to treat such complications. Metabolic compli-
et al 150 ) in their pilot series, in which 13 patients cations during chemotherapy for aggressive lym-
were treated and achieved C R although four of the phomas may be manifested dramatically. For in-
13 patients exhibited relapse in the C N S . In the stance, rapid killing of large numbers of tumor cells
subsequent and larger study reported by Coleman et by chemotherapy-driven release of cellular phos-
al150 involving 44 patients, the original protocol was phate into the circulation may cause a rapid decline
VOLUME 62 • SUPPLEMENT I CLEVELAND CLINIC JOURNAL OF MEDICINES I - 37
NON-HODGKIN'S LYMPHOMAS • FISHER AND OKEN
in serum calcium levels that, when coupled with able, whereas in other situations a less intense regi-
elevated serum potassium levels, can result in car- men may offer better clinical results.165'166
diac arrest.
Dissemination of tumor to the C N S in patients Treatment of elderly patients
with aggressive non-Hodgkin's lymphoma carries a A g e is an important independent prognostic fac-
very poor prognosis. Nonetheless, some patients will tor for clinical response and survival in patients with
respond well to intensive combination chemother- aggressive non-Hodgkin's lymphoma. 40,167 " 171 Elderly
apy and may achieve increased long-term sur- patients in general have poor clinical outcomes,
vival. 157,158 Primary C N S non-Hodgkin's lymphoma even when adjusted for higher rates of death from
is not frequently encountered in patients who are causes unrelated to the lymphoma. 172 Elderly pa-
not immunocompromised; the accelerating A I D S tients with aggressive non-Hodgkin's lymphoma
epidemic will increase the frequency with which have prognostic factors comparable to those of
oncologists encounter primary C N S lymphoma. A t younger patients. Vose et al167 have reported that the
present, this disorder is treated with intrathecal che- specific causes of death in elderly patients with ag-
motherapy (with or without radiation), systemic in- gressive non-Hodgkin's lymphoma are related to
tensive chemotherapy (with or without radiation), progression of the disease or treatment toxicity, es-
and osmotic blood-brain barrier disruption. 159 " 161 pecially cardiovascular and infectious complica-
A d d i t i o n of r a d i a t i o n therapy to e f f e c t i v e tions. Investigators have attempted to address the
chemotherapeutic regimens significantly improves problem of treatment of elderly patients with aggres-
the median survival in adult primary C N S lym- sive n o n - H o d g k i n ' s lymphoma by d e v e l o p i n g
phoma; local control and overall outcome are im- chemotherapeutic regimens specifically tailored for
proved when the dose is in excess of 40 G y to 50 Gy. these patients. 173 " 177 O'Reilly et al173 reported that
A chemotherapeutic regimen that has shown prom- elderly patients with advanced-stage diffuse large-
ise in the treatment of such patients incorporates cell lymphoma were administered weekly chemo-
vincristine, doxorubicin, cyclophosphamide, and therapy with low-dose A C O P - B (low-dose doxoru-
prednisolone. 159 T h e place of high-dose intravenous bicin, cyclophosphamide, vincristine, prednisone,
methotrexate in treatment of patients with primary and bleomycin) and V A B E (etoposide, doxorubicin,
C N S lymphoma appears to be rather well estab- vincristine, prednisone, and bleomycin). Of 72 pa-
lished. 161 ' 162 tients (ages 65 to 85 years) prospectively adminis-
O n e of the very challenging aspects of lymphoma tered successive A C O P - B and V A B E regimens,
therapy involves treatment of patients with H I V overall response rates ranged between approxi-
infection who present with non-Hodgkin's lym- mately 70% and 90%; however, the V A B E regimen
phoma. Levine 163 has discussed the clinical and bio- was associated with grade IV hematologic toxicity
logic characteristics as well as potential treatment in 58% of patients. T h e low-dose A C O P - B regimen
approaches. Non-Hodgkin's lymphomas in HlV-in- was associated with a 28% overall survival rate at 6
fected patients are typically intermediate-grade dif- years, and the V A B E regimen yielded a 36% overall
fuse large-cell or high-grade small noncleaved-cell survival rate at 4 years.
tumors. Their clinical behavior and response to Gaynor et al 178 have recently reported on their
treatment differ considerably from that of interme- analysis of factors accounting for diminished sur-
diate- and high-grade non-Hodgkin's lymphomas in vival of elderly ( > 60 years) patients participating in
HIV-negative patients, despite considerable similar- the N a t i o n a l High-Priority L y m p h o m a S t u d y
ity in histologic features. Intensive chemotherapeu- ( S W O G - 8 5 1 6 ) . In this randomized prospective
tic regimens have relatively little impact; in the study, patients with intermediate- and high-grade
presence of opportunistic infection, patients exhibit lymphoma were treated with the same initial drug
poor responses to chemotherapy. 164 However, some dose irrespective of age. T h e age-adjusted risk in-
HIV-positive patients with non-Hodgkin's lym- dex 40 indicated a similar risk profile for patients in
phoma may respond to chemotherapy in the ab- the elderly as opposed to nonelderly group. Results
sence of opportunistic infection. A t present, there is showed that elderly patients exhibited a poorer out-
no standard chemotherapeutic regimen for treat- come than did those age 60 or under. T h e incidence
ment of these patients. In some circumstances, in- in each age group of fatal toxicities was similar for
tense chemotherapeutic combinations are prefer- patients in the CHOP, m - B A C O D , and ProMACE-
SI-36 CLEVELAND CLINIC JOURNAL OF MEDICINE VOLUME 62 • SUPPLEMENT I
NON-HODGKIIM'S LYMPHOMAS • FISHER AND OKEN
C y t a B O M treatment arms;
TABLE 6
however, a significantly TREATMENT OF NON-HODGKIN'S LYMPHOMAS
higher incidence was noted
in patients assigned to the Category Option
M A C O P - B treatment arm. Low-grade
The authors concluded that
Stage 1 or II Radiation
the poor survival of elderly Stage III or IV Watch and wait or combination chemotherapy ± interferon-alfa
patients in this trial could
Intermediate-grade
be attributed to treatment
with M A C O P - B , although Stage 1 or II CHOP ± radiation
Stage II, bulky. III, IV CHOP
the survival of elderly pa-
tients receiving full initial High-grade
doses of C H O P , m - B A - Lymphoblastic Combination chemotherapy + CNS prophylaxis ± radiation
COD, or ProMACE- Small noncleaved-cell
C y t a B O M was similar to (Burkitt's) Combination chemotherapy
that of patients age 60 or
under.
Tirelli et al 174 reported
on patients older than 70 years with unfavorable chemotherapy incorporating r H u I F N - a may be
non-Hodgkin's lymphoma who were treated with a successful. T h e intermediate-stage non-Hodgkin's
c h e m o t h e r a p e u t i c r e g i m e n involving V M P lymphomas are treated by combination chemother-
(etoposide, mitoxantrone, and prednimustine). Me- apy with or without radiation, depending upon the
dian survival was approximately 14 months, and the stage and presence or absence of bulky disease. T h e
percentage of patients exhibiting a clinical response high-grade non-Hodgkin's lymphomas present a
was high. In most cases, the lymphoma was the clinical challenge to the treating oncologist; treat-
cause of death. ment options for this category of disease include
combination chemotherapy with C N S prophylaxis,
CONCLUSIONS possible radiation therapy, and, in some cases,
autologous or allogeneic bone marrow transplanta-
A t present, approximately one half of patients tion.
under 70 years of age with aggressive n o n - It is important that an experienced pathologist be
Hodgkin's lymphoma can achieve a complete re- included in the morphologic and laboratory diagno-
mission with a chance for long-term survival and a sis of patients with suspected non-Hodgkin's lym-
reasonable quality of life. During the past 30 years, phoma. In the absence of accurate diagnosis, it is
much has been learned about the genetics, immu- unlikely that optimal treatment plans can be devel-
nology, and basic cellular biology of this diverse oped. T h e treating oncologist must exercise particu-
group of diseases. A recently developed classifica- lar diligence in the physical evaluation of all pa-
tion system 7 has helped to clarify the disease by tients at initial diagnosis and during their
providing a uniform language permitting accurate continuing care. Moreover, the oncologist and the
diagnosis and subsequent treatment. Most of the adjuvant professional team must sufficiently educate
non-Hodgkin's lymphomas are sensitive to chemo- patients about the clinical nature of their disease so
therapy and radiation therapy, but whereas some that situations of great clinical concern may be rap-
varieties are curable, others exhibit a characteristic idly identified, such as fever associated with neu-
pattern of initial clinical response followed by mul- tropenia following combination chemotherapy.
tiple relapses. A tabular presentation of general With the availability of sophisticated laboratory
treatment options presented in Table 6 and sche- techniques and through ongoing clinical trials of
matically represented in the Figure indicates that new agents as well as modifications of existing com-
for early-stage low-grade n o n - H o d g k i n ' s lym- bination chemotherapeutic regimens, new treat-
phomas, radiation is the treatment of choice. For ments will likely be developed to improve the clini-
advanced-stage indolent lymphomas, a watch-and- cal state and extend the survival of non-Hodgkin's
wait approach may be sufficient, or combination lymphoma patients.
VOLUME 62 • SUPPLEMENT I CLEVELAND CLINIC JOURNAL OF MEDICINE SI-3 7
NON-HODGKIN'S LYMPHOMAS • FISHER AND OKEN
globulin and T-cell receptor gene rearrangement and expression
REFERENCES
in human lymphoid leukemia cells arrested at different stages of
maturation. Proc Natl Acad Sei U S A 1986; 83:8759-8763.
1. Wingo PA, Tong T, Bolden S. Cancer statistics, 1995. C A 23. Waldmann TW, Davis MM, Bongiovanni KF, et al. Rearrange-
CancerJ Clin 1995; 45:8-30. ments of genes for the antigen receptor on T-cells as markers of
2. Longo D L , DeVita V T Jr, Jaffe E S , Mauch P, Urba WJ. Lym- lineage and clonality in human lymphoid neoplasms. N Engl ]
phocytic lymphomas. In: De Vita V T Jr, Hellman S, Rosenberg Med 1985; 313:776-783.
S A , editors. Cancer: principles & practice of oncology. Philadel- 24. Bertness V, Kirsch I, Hollis G , et al. T-cell receptor gene
phia: JB Lippincott, 1993:1859-1927. rearrangements as clinical markers of human T-cell lymphomas. N
3. Gaynor E R , Fisher RI. Recent advances in the management of Engl J Med 1985; 313:534-538.
non-Hodgkin's lymphomas. In: Bone RC, Greenberger NJ, Kohler 25. Griesser, H , Feller A, Lennert K, et al. Rearrangement of the B
PO, editors. Disease-a-month. Chicago: Year Book Medical Pub- chain of the T-cell antigen receptor and immunoglobulin genes in
lishers, 1989:35. lymphoproliferative disorders. J Clin Invest 1986; 78:1179-1184.
4. Rappaport H . Tumors of the hematopoietic system. In: Atlas of 26. Tonegawa S. Somatic generation of antibody diversity. Nature
Tumor Pathology, Section III Fascicle 8. Washington DC: Ameri- 1983; 302:575-581.
can Registry of Pathology, Armed Forces Institute of Pathology, 27. Hood L, Kronenberg M, Hunkapiller T. T-cell antigen recep-
1966. tors and the immunoglobulin supergene family. Cell 1985;
5. L u k e s R J , Collins R D . Immunologic characterization of human 40:225-229.
malignant lymphomas. Cancer 1974; 34:1488-1503. 28. Cleary ML, Chao J, Warnke R, et al. Immunoglobulin gene
6. Lennert K , Mohri N . Stein H, Kaiserling E. The histopathology rearrangement as a diagnostic criterion of B-cell lymphoma. Proc
of malignant lymphoma. Br J Haematol 1975; 31(Suppl):193- Natl Acad Sei U S A 1984; 81:593-597.
203. 29. Yunis J J . Chromosomal rearrangements, genes and fragile sites
7. T h e Non-Hodgkin's Lymphoma Pathologic Classification Pro- in cancer: clinical and biological implications. In: DeVita V T Jr,
ject. National Cancer Institute sponsored study of classifications Hellman S, Rosenberg S A , editors. Important advances in oncol-
of non-Hodgkin's lymphomas: summary and description of a work- ogy. Philadelphia: J B Lippincott, 1986:93-128.
ing formulation for clinical usage. Cancer 1982; 49:2112-2135. 30. Yunis J J , Oken MM, Kaplan ME, Ensrud KM, Howe R B ,
8. Sheibani K, Sohn C C , Burke J S , Winberg C D , Wu A M , Rap- Theologides A . Distinctive chromosomal abnormalities in his-
paport H . Monocytoid B-cell lymphoma: a novel B-cell neo- tologic subtypes of non-Hodgkin's lymphoma. N Engl J Med 1982;
plasm. A m J Pathol 1986; 124:310-318. 307:1231-1236.
9. J a f f e ES, Bookman M A , Longo D L . Lymphocytic lymphoma of 31. Yunis J J , Oken MM, Theologides A , Howe R B , Kaplan ME.
intermediate differentiation-mantle zone lymphoma: a distinct Recurrent chromosomal defects are found in most patients with
subtype of B-cell lymphoma. Hum Pathol 1987; 18:877-880. non-Hodgkin's-lymphoma. Cancer Genet Cytogenet 1984;
10. Greer JP, Kinney M C , Collins R D , et al. Clinical features of 31 13:17-28.
patients with Ki-1 anaplastic large-cell lymphoma. J Clin Oncol 32. Manolov G , Manolova Y. Marker band in one chromosome 14
1991; 9:539-547. from Burkitt lymphomas. Nature 1982; 237:33-34.
11. Kemme D J , Bunn PA Jr. State of the art therapy of mycosis 33. Zech L, Hoglund V, Nilsson K, et al. Characteristic chromoso-
fungoides and Sezary syndrome [published erratum appears in mal abnormalities in biopsies and lymphoid-cell lines from pa-
Oncology (Huntingt) 1992; 6(8):41]. Oncology (Huntingt) 1992; tients with Burkitt and non-Burkitt lymphomas. Int J Cancer
6(2):31—48. 1976; 17:47-56.
12. Yunis J J , Frizzera G , Oken MM, et al. Multiple recurrent 34. Fukuhara S, Rowley J D , Variakojis D, et al. Chromosome
genomic defects in follicular lymphoma. N Engl J Med 1987; abnormalities in poorly differentiated lymphocytic lymphoma.
316:79-84. Cancer Res 1979; 39:3119-3128.
13. Magrath IT. Lymphocyte differentiation: an essential base for 35. Taub R , Kirsch I, Morton C , et al. Translocation of the c-myc
the comprehension of lymphoid neoplasia. J Natl Cancer Inst gene into the immunoglobulin heavy chain locus in human
1981;67:501-514. Burkitt's lymphoma and murine plasmacytoma cells. Proc Natl
14. Rowley J D . Chromosome studies in the non-Hodgkin's lym- Acad Sei U S A 1982; 79:7837-7841.
phomas: the role of the 14;18 translocation. J Clin Oncol 1988; 36. Dalla-Favera R, Bregni M, Erickson J , et al. Human c-myc
6:919-925. oncogene is located on the region of chromosome 8 that is translo-
15. Cossman J, Uppenkamp M, Sundeen J, et al. Molecular genet- cated in Burkitt lymphoma cells. Proc Natl Acad Sei U S A 1982;
ics and the diagnosis of lymphoma. Arch Pathol Lab Med 1988; 79:7824-7827.
112:117-127. 37. Tsujimoto Y, Finger L R , Yunis J J , et al. Cloning of the chromo-
16. Weiss IM, Warnke R A , Sklar J, et al. Molecular analysis of the some breakpoint of neoplastic B cells with the t(14;18) chromo-
t(14;18) chromosomal translocation in malignant lymphomas. N some translocation. Science 1984; 226:1098-1099.
Engl J Med 1987; 317:1185-1189. 38. Kaneko Y, Rowley J D , Variakojis D, et al. Prognostic implica-
17. N g a n B , Levy Z C , Weiss I M , et al. Expression in non- tions of karyotype and morphology in patients with non-
Hodgkin's lymphomas of the bcl-2 protein associated with the Hodgkin's lymphoma. Int J Cancer 1983; 32:683-692.
t( 14; 18) chromosome translocation. N Engl J Med 1988; 39. Tsujimoto Y, Yunis J, Onorato-Showe L, et al. Molecular clon-
318:1638-1643. ing of the chromosomal breakpoint of B-cell lymphomas and
18. Levy R, Warnke R, Dorfman RF, et al. The monoclonality of leukemias with the t ( l l ; 1 4 ) chromosome translocation. Science
B-cell lymphomas. J Exp Med 1977; 145:1014-1028. 1984; 224:1403-1406.
19. Flug F, Pellici P-G, Bonetti F, et al. T-cell receptor gene ar- 40. Shipp M A , et al. A Predictive model for aggressive non-
rangements as markers of lineage and clonality in T-cell neo- Hodgkin's lymphoma. The International Non-Hodgkin's Lym-
plasms. Proc Natl Acad Sei U S A 1985; 82:3460-3464. phoma Prognostic Factors Project. N Engl J Med 1993; 3 2 9 : 9 8 7 -
20. Furley A J , Mizutani S, Weilbaecher K, et al. Developmentally 994.
regulated rearrangement and expression of genes encoding the 41. Bastion Y, Berger F, Bryon PA, et al. Follicular lymphomas:
T-cell receptor-T3 complex. Cell 1986; 46:75-87. assessment of prognostic factors in 127 patients followed for 10
21. Arnold A , Cossman J, Bakhshi A , et al. Immunoglobulin-gene years. A n n Oncol 1991; 2(Suppl):123-129.
rearrangements as unique clonal markers in human lymphoid 42. De Vita VT, Canellos GP, Chabner B A , et al. Advanced diffuse
neoplasms. N Engl J Med 1983; 309:1593-1599. histiocytic lymphoma: a potentially curable disease. Lancet 1975;
22. Davey MP, Bongiovanni KF, Kaulfersch W, et al. Immuno- 1:248-250.
SI-38 CLEVELAND CLINIC JOURNAL OF MEDICINE VOLUME 62 • SUPPLEMENT I
NON-HODGKIIM'S LYMPHOMAS • FISHER AND OKEN
43. Cossman J , Jaffe ES, Fisher RI. Immunologic phenotypes of 58:920-925.
diffuse aggressive non-Hodgkin's lymphomas: correlation with 65. Armitage J O . Bone marrow transplantation for indolent lym-
clinical features. Cancer 1984; 54:1310-1317. phomas. Semin Oncol 1993; 20(Suppl 5): 136-142.
44. Fisher RI, Jones R B , DeVita VT, et al. Natural history of 66. Gorin N C , Gale R, Armitage JO, et al. Autologous bone mar-
malignant lymphomas with divergent histologies at staging evalu- row transplants. Different indications in Europe and North Amer-
ation. Cancer 1981; 47:2022-2025. ica. Lancet 1989;2:317-318.
45. Weisenberger D D , D u g g a n M J , Perry D A , et al. Non- 67. Fouillard L, Gorin N C , Laporte JP. Feasibility of autologous
Hodgkin's lymphomas of mantle zone origin. Pathol Annu 1991; bone marrow transplantation for early consolidation of follicular
1:139-158. non-Hodgkin's lymphoma. Eur J Haematol 1991; 46:279-284.
46. Richards M A , Hall PA, Gregory WM, et al. Lymphoplasmacy- 68. Carabell S, Chaffey J, Rosenthal D , et al. Results of total body
toid and small-cell centrocytic non-Hodgkin's lymphoma: a retro- irradiation in the treatment of advanced non-Hodgkin's lym-
spective analysis from St. Bartholomew's Hospital 1972-1986. He- phomas. Cancer 1979; 43:994-1000.
matol Oncol 1989; 7:19-35. 69. Vose JM, Kennedy B C , Bierman PJ, et al. Long-term sequelae
47. Horning SJ. Natural history of and therapy for the indolent of autologous bone marrow or peripheral stem cell transplantation
non-Hodgkin's lymphomas. Semin Oncol 1993; 20(Suppl 5 ) : 7 5 - for lymphoid malignancies. Cancer 1992; 69:784-789.
88. 70. Bandini G , Michallet M, Rosti G, et al. Bone marrow trans-
48. Leonard R C , Hayward R L , Prescott RJ, et al. The identifica- plantation for chronic lymphocytic leukemia. Bone Marrow
tion of discrete prognostic groups in low-grade non-Hodgkin's Transplant 1991; 7:251-253.
lymphoma: The Scotland and Newcastle Lymphoma Group Ther- 71. Rabinowe S N , Soiffer RJ, Gribben J G , et al. Autologous and
apy Working Party. A n n Oncol 1991; 2:655-662. allogenic bone marrow transplantation (BMT) for patients with
49. Soubeyran P, Eghbali H , Bonichon F, et al. Low-grade follicular Binet stage B and C B-cell chronic lymphocytic leukemia (B-
lymphomas: analysis of prognosis in a series of 281 patients. Eur J CLL) [abstract]. Blood 1992; 80(Suppl l):170a.
Cancer 1991; 27:1606-1613. 72. Freedman A, RitzJ, NeubergD, et al. Autologous bone marrow
50. Romaguera JE, McLaughlin P, North L, et al. Multivariate transplantation in 69 patients with a history of low-grade B-cell
analysis of prognostic factors in stage IV follicular low-grade lym- on-Hodgkin's lymphoma. Blood 1991; 77:2524-2529.
phoma: a risk model. J Clin Oncol 1991; 9:762-769. 73. Colombat P, Binet C , Linassier C , et al. High dose chemother-
51. Gospodarowicz MK, Bush R S , Brown T C , et al. Prognostic apy with autologous marrow transplantation in follicular lym-
factors in nodular lymphomas: a multivariate analysis based on the phomas. Leuk Lymphoma 1992; 7(Suppl):3-6.
Princess Margaret Hospital experience. Int J Radiat Oncol Biol 74- Gribben J , Freedman A, Neuberg D , et al. Immunologic purg-
Phys 1984; 10:489-497. ing of marrow assessed by PCR before autologous bone marrow
52. Gallagher C J , Gregory WM, Jones AE, et al. Follicular lym- transplantation for B-cell lymphoma. N Engl J Med 1991;
phoma: prognostic factors for response and survival. J Clin Oncol 325:1525-1533.
1986; 4:1470-1480. 75. Schouten H C , Colombat P, Verdonck LF, et al. Autologous
53. Gelb A B , Davis R, Mo S, et al. Prognostic significance of host bone marrow transplantation ( A B M T ) for low grade non-
"helper" T-cells and proliferating cells in diffuse small lymphocytic Hodgkin's lymphoma (NHL). The European Bone Marrow Trans-
lymphomas: results of a tree-structured survival analysis [abstract]. plant Group ( E B M T ) experience [abstract]. Blood 1992;
Lab Invest 1992; 66:454. 80(Suppl l):67a.
54. Strickier J G , Copenhaver C M , Rojas VA, et al. Comparison of 76. Grossbard ML, Nadler L M . Monoclonal antibody therapy for
"host cell infiltrates" in patients with follicular lymphoma with indolent lymphomas. Semin Oncol 1993; 20(Suppl 5): 118-135.
and without spontaneous regression. A m J Clin Pathol 1988; 77. Nadler LM, Stashenko, P, Hardy R, et al. Serotherapy of a
90:257-261. patient with a monoclonal antibody directed against a human
55. Medeiros LJ, Picker L J , Gelb A B , et al. Numbers of host lymphoma-associated antigen. Cancer Res 1980; 40:3147-3154.
"helper" T-cells and proliferating cells predict survival in diffuse 78. Meeker T C , Lowder J , Maloney D G , et al. A clinical trial of
small-cell lymphomas. J Clin Oncol 1989; 7:1009-1017. anti-idiotype therapy for B-cell malignancy. Blood 1985;
56. H u E, Weiss LM, Hoppe RT, et al. Follicular and diffuse mixed 65:1349-1363.
small-cleaved and large-cell lymphoma: a clinicopathologic study. 79. Scheinberg D A , Straus DJ, Yeh S D , et al. A phase I toxicity,
J Clin Oncol 1985; 3:1183-1187. pharmacology and dosimetry trial of monoclonal antibody OKB7
57. Macartney J C , Camplejohn R S , Morris R , et al. D N A flow in patients with non-Hodgkin's lymphoma. Effects of tumor bur-
cytometry of follicular non-Hodgkin's lymphoma. J Clin Pathol den and antigen expression. J Clin Oncol 1990; 8:792-803.
1991;44:215-218. 80. Hale G, Dyer M J S , Clark M R , et al. Remission induction in
58. Weisdorf DJ, Anderson JW, Glick J H , et al. Survival after non-Hodgkin's lymphoma with reshaped human monoclonal an-
relapse of low-grade non-Hodgkin's lymphoma. Implications for tibody CAMPATH-1H. Lancet 1988; 2:1394-1399.
marrow transplantation. ] Clin Oncol 1992; 10:942-947. 81. Clendeninn N J , Nethersell ABW, Scott JE, et al. Phase I/II trials
59. Armitage J O . Treatment of non-Hodgkin's lymphoma. N Engl J of CAMPATHTM-1H, a humanized anti-lymphocyte mono-
Med 1993; 328:1023-1030. clonal antibody (MoAb), in non-Hodgkin's lymphoma (NHL)
60. Paryani S B , Hoppe R T , C o x R S , et al. Analysis of non- and chronic lymphocytic leukemia (CLL) [abstract]. Blood 1992;
Hodgkin's lymphomas with nodular and favorable histologies, 80(Suppl) :158a.
Stage I and II. Cancer 1983; 52:2300-2307. 82. Grossbard ML, Press OW, Appelbaum F R , et al. Monoclonal
61. Portlock C S , Fischer D S , Cadman E, et al. High dose pulse antibody-based therapies of leukemia and lymphoma. Blood 1992;
chlorambucil in advanced low-grade non-Hodgkin's lymphoma. 80:863-878.
Cancer Treat Rep 1987; 71:1029-1031. 83. Press OW, Appelbaum F, Ledbetter J A, et al. Monoclonal anti-
62. Portlock C S , Rosenberg S A . No initial therapy for Stage III and body 1F5 (anti-CD20) serotherapy of human B-cell lymphomas.
IV non-Hodgkin's lymphoma of favorable histologic types. Ann Blood 1987; 69:584-591.
Intern Med 1979;90:10-13. 84. Hansen RM, Borden E C . Current status of interferons in the
63. Longo DL, Young R C , Hubbard SM, et al. Prolonged initial treatment of cancer. Oncology 1992; 6 ( l l ) : 1 9 - 2 4 .
remission in patients with nodular mixed lymphoma. Ann Intern 85. Bonnem EM. Alpha-interferon: the potential drug of adjuvant
Med 1984; 100:651-656. therapy: past achievements and future challenges. Eur J Cancer
64. Glick J H , Barnes JM, Ezdinli EZ, et al. Nodular mixed lym- 1991; 27(Suppl 4 ) : S 2 - S 6 .
phoma. Results of a randomized trial failing to confirm prolonged 86. Parkinson DR, Sznol M, Cheson B D . Biologic therapies for
disease-free survival with COPP chemotherapy. Blood 1981; low-grade lymphomas. Semin Oncol 1993; 20(Suppl 5)t 111—117.
VOLUME 62 • SUPPLEMENT I CLEVELAND CLINIC JOURNAL OF MEDICINESI-37
NON-HODGKIN'S LYMPHOMAS • FISHER AND OKEN
87. Gaynor E R , Fisher RI. Clinical trials of alpha-interferon in the Hodgkin's lymphoma. Results from a prospective, randomized
treatment of non-Hodgkin's lymphoma. Semin Oncol 1991; phase III clinical trial in 231 patients [abstract]. Blood 1992;
18(Suppl 7):12-17. 80(Suppl 1):287.
88. Dorr RT. Interferon-alpha in malignant and viral diseases: a 108. McLauglin P, Cabanillas F, Hagemeister F B , et al. CHOP-Bleo
review. Drugs 1993; 45(2):177-211. plus interferon or stage IV low-grade lymphoma. A n n Oncol
89. Borden E, Witt P, Paulnock D, et al. Antitumor effects of 1993;4:205-211.
interferons. Mechanisms and therapeutic activity. In: Mitchell M, 109. Coiffier B. Interferon-alpha-recombinant in the treatment of
editor. The biomodulation of cancer. New York: McGraw Hill, follicular lymphoma patients [editorial]. Ann Oncol 1993; 4 : 1 8 2 -
1992:440-476. 183.
90. Shearer M, Taylor-Papadimitriou J . Regulation of cell growth 110. Solal-Celigny P, Lepage E, Brousse N , et al. Recombinant IFN-
by interferon. Cancer Metastasis Rev 1987; 6:199-221. alpha-2b combined with a regimen containing doxorubicin in
91. Merigan T C , Sikora K, Breeden J H , et al. Preliminary observa- patients with advanced follicular lymphoma. N Engl J Med 1993;
tions on the effect of human leukocyte interferon in non- 329:1608-1614.
Hodgkin's lymphoma. N Engl J Med 1978; 299:1449-1453. 111. Smalley RV, Andersen JW, Hawkins MJ, et al. Interferon-alfa
92. Gutterman J U , Blumenschein G R , Alexanian R , et al. Leuko- combined with cytotoxic chemotherapy for patients with non-
cyte interferon-induced tumor regression in human metastatic Hodgkin's lymphoma. N Engl J Med 1992; 327:1336-1341.
breast cancer, multiple myeloma and malignant lymphoma. Ann 112. Andersen JW, Smalley RV. Interferon-alfa plus chemotherapy
Intern Med 1980; 93:399-406. for non-Hodgkin's lymphoma. Five-year follow-up [letter]. N Engl
93. Q u e s a d a J R , Hawkins M, Horning S, et al. Collaborative J Med 1993; 329(24):1821-1822.
phase I-II study of recombinant DNA-produced leukocyte inter- 113. Peterson B A , Petroni G , Oken MM, Ozer H . Cyclophos-
feron (clone A ) in metastatic breast cancer, malignant lymphoma phamide versus cyclophosphamide plus interferon-alfa-2b in folli-
and multiple myeloma. A m J Med 1984; 77:427-432. cular low-grade lymphomas. A preliminary report of an intergroup
94. Louie A C , Gallagher J G , Sikora K , et al. Follow-up observa- trial ( C A L G B 8691 and E S T 7486) [abstract]. Proc A m Soc Clin
tions on the effect of human leukocyte interferon in non- Oncol 1993; 12:1240.
Hodgkin's lymphoma. Blood 1981; 58:712-718. 114. Cheson B D . New chemotherapeutic agents for the treatment of
95. Foon K A , Sherwin S A , Abrams P G , et al. Treatment of ad- low-grade non-Hodgkin's lymphomas. S e m i n Oncol 1993;
vanced non-Hodgkin's lymphoma with recombinant leukocyte A 20(Suppl 5):96—110.
interferon. N Engl J Med 1984; 311:1148-1152. 115. Chun H G , Leyland-Jones B , Cheson B D . Fludarabine phos-
96. Horning SJ, Merigan T C , Krown SE, et al. Human interferon- phate. A synthetic purine antimetabolite with significant activity
alpha in malignant lymphoma and Hodgkin's disease. Results of against lymphoid malignancies. J Clin Oncol 1991; 9:175-188.
the American Cancer Society trial. Cancer 1985; 56:1305-1310. 116. Keating MJ, O'Brien SO, Plunkett W, et al. Fludarabine phos-
97. O'Connell M J , Colgan JP, Oken MM, et al. Clinical trial of phate. A new active agent in hematologic malignancies. Semin
recombinant leukocyte A interferon as initial therapy for favor- Hematol 1994; 3 1 ( l ) : 2 8 - 3 9 .
able histology non-Hodgkin's lymphoma and chronic lympho- 117. Whelan J S , Davis C L , Rule S, et al. Fludarabine phosphate for
cytic leukemia. A n Eastern Cooperative Oncology Group pilot the treatment of low-grade lymphoid malignancy. Br J Cancer
study. J Clin Oncol 1986; 4:128-136. 1991;64:120-123.
98. Wagstaff J , Loynds P, Crowther D . A phase II study of human 118. Hochster H S , Kim K , Green M D , et al. Activity of fludarabine
r D N A alpha-2 interferon in patients with low-grade non- in previously treated non-Hodgkin's low-grade lymphoma. Results
Hodgkin's lymphoma. Cancer Chemother Pharmacol 1986; of an Eastern Cooperative Oncology Group study. J Clin Oncol
18:54-58. 1992; 10:28-32.
99. Gresser I, Maury C , Tovey M. Efficacy of combined interferon 119. Redman J R , Cabanillas F, Velasquez WS, et al. Phase II trial of
and cyclophosphamide therapy after diagnosis of lymphoma in fludarabine phosphate in lymphoma. A n effective new agent in
A K R mice. Eur J Cancer 1978; 14:97-99. low-grade lymphoma. J Clin Oncol 1992; 10:790-794.
100. Balkwill F R , Moodie EM. Positive interactions between human 120. Schilling PJ, Vadhan-Raj S. Concurrent cytomegalovirus and
interferon and cyclophosphamide or Adriamycin in a human tu- Pneumocystis pneumonia after fludarabine therapy for chronic
mor model system. Cancer Res 1984; 44:904-908. lymphocytic leukemia. N Engl J Med 1990; 323:833-834.
101. Hawkins MJ, O'Connell M J , Schiller J H , et al. Phase I evalu- 121. Zinzani PL, Levrero M G , Lauria F, et al. Alpha-interferon as
ation of recombinant A interferon-alpha in combination with maintenance drug after initial fludarabine therapy for patients
C O P A chemotherapy [abstract]. Proc A m Soc Clin Oncol 1985; with chronic lymphocytic leukemia and low-grade non-Hodgkin's
4:229. lymphoma. Haematol 1994; 79:55-60.
102. Chisesi T, Capnist G , Vespignani M, et al. Interferon alfa-2b 122. Dillman, R O . A new chemotherapeutic agent. Deoxycoformy-
and chlorambucil in the treatment of non-Hodgkin's lymphoma. cin (Pentostatin). Semin Hematol 1994; 3 1 ( l ) : 1 6 - 2 7 .
Invest New Drugs 1987; 5(Suppl):35-40. 123. Duggan D B , Anderson J R , Dillman R, et al. 2-deoxycoformy-
103. Chisesi T, Congiu M, Contu A , et al. Randomized study of cin (Pentostatin) for refractory non-Hodgkin's lymphoma. A
chlorambucil in low-grade non-Hodgkin's lymphoma: an interim C A L G B phase II study. Med Pediatr Oncol 1990; 18:203-206.
report of a randomized study. Eur J Cancer 1991; 27(Suppl 124. Cummings FJ, Kim K, Neiman R S , et al. Phase II trial of
4):S31-S33. Pentostatin in refractory lymphomas and cutaneous T-cell disease.
104. Rohatiner A Z S , Richards M A , Barnett N J , et al. Chloram- J Clin Oncol 1991; 9:565-571.
bucil and interferon for low-grade non-Hodgkin's lymphoma. Br J 125. Beutler E. New chemotherapeutic agent. 2-chlorodeoxyadenos-
Cancer 1987; 55:225-226. ine. Semin Hematol 1994; 3 1 ( l ) : 4 0 - 4 5 .
105. Ozer H , Anderson J R , Peterson B A , et al. Combination trial of 126. Seto S, Carrera C J , Kubota M, et al. Mechanism of deoxyade-
subcutaneous interferon-alfa-2b and oral cyclophosphamide in nosine and 2-chlorodeoxyadenosine toxicity to nondividing hu-
favorable histology, non-Hodgkin's lymphoma. Invest New Drugs man lymphocytes. J Clin Invest 1985; 75:377-383.
1987; 5(Suppl):S27-S33. 127. Carrera C J , Terai C , Lotz M, et al. Potent toxicity of 2-chlo-
106. Price C G A , Rohatiner A Z S , Steward W, et al. Interferon-al- rodeoxyadenosine toward human monocytes in vitro and in vivo.
pha-2b in the treatment of follicular lymphoma. Preliminary re- J Clin Invest 1990; 86:1480-1488.
sults of a trial in progress. A n n Oncol 1991; 2(Suppl 2):141—145. 128. Carrera C J , Piro L D , Saven A , et al. 2-chlorodeoxyadenosine
107. Hagenbeek A , Carde P, Somers R, et al. Maintenance of remis- chemotherapy triggers programmed cell death in normal and ma-
sion with human recombinant alpha-2 interferon (Roferon-A) in lignant lymphocytes. In: Harkness RA, Elion TB, Zollner N,
patients with stages III and IV low-grade malignant non- editors. Purine and pyrimidine metabolism in man VII, part A.
SI-40 CLEVELAND CLINIC JOURNAL OF MEDICINE VOLUME 62 • SUPPLEMENT I
NON-HODGKIIM'S LYMPHOMAS • FISHER AND OKEN
New York: Plenum, 1991:15-18. plantation as consolidation therapy during first complete remis-
129. Kay A C , Saven A , Carrera C J , et al. 2-chlorodeoxyadenosine sion in adult patients with poor-risk aggressive lymphoma: a pilot
treatment of low-grade lymphomas. J Clin Oncol 1992; 10:371- study. Blood 1992; 80:1130-1134.
377. 148. Voskes J B , Jones SE, McKelvey EM. The chemotherapy of
130. Beutler E, Piro L D , Saven A , et al. 2-chlorodeoxyadenosine lymphoblastic lymphoma. Blood 1981; 57:186-188.
(2-CdA). A potent chemotherapeutic and immunosuppressive 149. Levine AM, Forman SJ, Meyer P R , et al. Successful therapy of
nucleoside. Leuk Lymphoma 1991; 5:1-8. convoluted T-lymphoblastic lymphoma in the adult. Blood 1983;
131. Salles G , Shipp M A , C o i f f i e r B . Chemotherapy of non- 61:92-98.
Hodgkin's aggressive lymphomas. S e m i n Hematol 1994; 150. Coleman C N , Picozzi V J Jr, Cox R S , et al. Treatment of lym-
31(l):46-69. phoblastic lymphoma in adults. J Clin Oncol 1986; 4:1628-1637.
132. Fisher R I , Miller T B , Dana BW, et al. Southwest Oncology 151. Slater D E , Mertelsmann R, Koziner B , et al. Lymphoblastic
Group clinical trials for intermediate and high-grade non- lymphoma in adults. J Clin Oncol 1986; 4:57-67.
Hodgkin's lymphoma. Semin Hematol 1984; 24(Suppl 1):21—25. 152. Bernstein J I , Coleman C N , Strickler J G , et al. Combined mo-
133. Jones SE, Miller TP, Connors J M . Long-term follow-up and dality therapy for adults with small non-cleaved-cell lymphoma
analysis for prognostic factors for patients with limited-stage dif- (Burkitt's and non-Burkitt's types). J Clin Oncol 1986; 4 : 8 4 7 -
fuse large-cell lymphoma treated with initial chemotherapy with 858.
or without adjuvant radiotherapy. J Clin Oncol 1989; 7:1186— 153. Lopez T M , Hagenmeister FB, McLaughlin P, et al. Small non-
1191. cleaved-cell lymphoma in adults: superior results for stages I-II
134. Mauch P, Leonard R , Skarin A , et al. Improved survival follow- disease. J Clin Oncol 1990; 8:615-622.
ing combined radiation therapy and chemotherapy for unfavor- 154- McMaster ML, Greer JP, Greco FA, et al. Effective treatment
able prognosis stage I-II non-Hodgkin's lymphoma. J Clin Oncol of small-non-cleaved-cell lymphoma with high-density, brief-du-
1985;3:1301-1308. ration chemotherapy. J Clin Oncol 1991; 9:941-946.
135. Shipp M A , Matt MM, Yeap B, et al. Patterns of relapse in 155. Morel P, Lepage E, Brice P, et al. Prognosis and treatment of
large-cell lymphoma patients with bulk disease. Implications for lymphoblastic lymphoma in adults. A report on 80 patients. J Clin
the use of adjuvant radiation therapy. J Clin Oncol 1989; 7 : 6 1 3 - Oncol 1992; 7:1078-1085.
618. 156. Straus D J , Wong GY, Liu J, et al. Small non-cleaved-cell lym-
136. Longo D L , Glatstein B, Duffey P L , et al. Treatment of local- phoma (undifferentiated lymphoma, Burkitt's type) in American
ized aggressive lymphoma with combination chemotherapy fol- adults. Results with treatment designed for acute lymphoblastic
lowed by involved-field radiation therapy. ] Clin Oncol 1989; leukemia. A m J Med 1991; 90:328-337.
9:1295-1302. 157. Haddy T B , Adde MA, Magrath IT. C N S involvement in small
137. Tondini C , Zanini M, Lombardi C , et al. Combined modality non-cleaved-cell lymphoma. Is C N S disease per se a poor prognos-
treatment with primary C H O P chemotherapy followed by locore- tic sign? J Clin Oncol 1991; 9:1973-1982.
gional irradiation in stage I or II histologically aggressive non- 158. Coiffier B , Gisselbrecht C , Herbrecht R, et al. LNH-84 regi-
Hodgkin's lymphomas. J Clin Oncol 1993; l l ( 4 ) : 7 2 0 - 7 2 5 . men. A multicenter study of intensive chemotherapy in 737 pa-
138. Schein P S , DeVita V T Jr., Hubbard S, et al. Bleomycin, tients with aggressive malignant lymphoma. J Clin Oncol 1989;
Adriamycin, cyclophosphamide, vincristine and prednisone (BA- 7:1018-1026.
C O P ) combination chemotherapy in the treatment , of advanced 159. Shibamato Y, Tsutsui K , Dodo Y, et al. Improved survival rate
diffuse histiocytic lymphoma. Ann Intern Med 1976; 8 5 : 4 1 7 - in primary intracranial lymphoma treated by high-dose radiation
422. and systemic vincristine-doxorubicin-cyclophosphamide-pred-
139. Fisher R I , DeVita V T Jr, Johnson B L , et al. Prognostic factors nisolone chemotherapy. Cancer 1990; 65:1907-1912.
for advanced diffuse histiocytic lymphoma following treatment 160. Neuwelt E A , Goldman D L , Dahlborg S A , et al. Primary C N S
with combination chemotherapy. A m J Med 1977; 63:177-182. lymphoma treated with osmotic blood-brain barrier disruption.
140. Gaynor E R , Ultmann J E , Golomb H M , Sweet D L . Treatment Prolonged survival and preservation of cognitive function. J Clin
of diffuse histiocytic lymphoma (DHL) with C O M L A (cyclophos- Oncol 1991; 9:1580-1590.
phamide, oncovin, methotrexate, leucovorin, cytosine arabi- 161. DeAngelis L M , Yahalom J , Thaler H T , et al. Combined modal-
noside): a 10-year experience in a single institution. J Clin Oncol ity therapy for primary C N S lymphoma. J Clin Oncol 1992;
1985; 3:1596-1604. 10:635-643.
141. Fisher R I , Gaynor E R Dahlberg S, et al. Comparison of a 162. Blay JY, Lasset C , Carrie C , et al. Multivariate analysis of
standard regimen ( C H O P ) with three intensive chemotherapy prognosis factors in patients with non HIV-related primary cere-
regimens for advanced non-Hodgkin's lymphoma. N Engl J Med bral lymphoma. A proposal for a prognostic scoring. Br J Cancer
1993; 328:1002-1006. 1993;67:1136-1141.
142. Philip T, Chauvin F, Armitage J , et al. Parma international 163. L e v i n e A M . Acquired immunodeficiency syndrome-related
protocol. Pilot study of D H A P followed by involved-field radio- lymphoma. Blood 1992; 80:8-20.
therapy and B E A C with autologous bone marrow transplantation. 164. Kaplan L D , Kahn J O , Crowe S, et al. Clinical and virologic
Blood 1991; 77:1587-1592. effects of recombinant human granulocyte-macrophage colony
143. Armitage J O . Bone marrow transplantation. N Engl J Med 1994; stimulating factor in patients receiving chemotherapy for human
330:827-838. immunodeficiency virus-associated non-Hodgkin's lymphoma.
144. Gulati S C , Shank B , Black P, et al. Autologous bone marrow Results of a randomized trial. J Clin Oncol 1991; 9:929-940.
transplantation for patients with poor-prognosis lymphoma. J Clin 165. Levine AM, Sullivan-Halley J , Pike M C , et al. Human immu-
Oncol 1988; 6:1303-1313. nodeficiency virus-related lymphoma: prognostic factors predic-
145. Milpied N , Ifrah N , Kuentz M, et al. Bone marrow transplanta- tive of survival. Cancer 1991; 68:2466-2472.
tion for adult poor prognosis lymphoblastic lymphoma in first 166. Bermudez M A , G r a n t K M , Rodvien R , Mendes F. Non-
complete remission. Br J Haematol 1989; 73:82-87. Hodgkin's lymphoma in a population with or at risk for acquired
146. Santini G , Coser P, Chisesi T, et al. Autologous bone marrow immunodeficiency syndrome: indications for intensive chemo-
transplanatation for advanced stage adult lymphoblastic lym- therapy. A m J Med 1989; 86:71-76.
phoma in first complete remission. A pilot study of the Non- 167. Vose J M , Armitage J O , Weisenberger D D , et al. The impor-
Hodgkin's Lymphoma Cooperative Study Group ( N H L C S G ) . tance of age in survival of patients treated with chemotherapy for
Bone Marrow Transplant 1989; 4:399-404. aggressive non-Hodgkin's lymphoma. J Clin Oncol 1988,-6:1838-
147. Nademanee A , Schmidt G M , O'Donnell M R , et al. High-dose 1844.
chemoradiotherapy followed by autologous bone marrow trans- 168. Dixon D O , Neilan B , Jones SE, et al. Effect of age on therapeu-
VOLUME 62 • SUPPLEMENT I CLEVELAND CLINIC JOURNAL OF MEDICINESI-37
NON-HODGKIN'S LYMPHOMAS • FISHER AND OKEN
tic outcome in advanced diffuse histiocytic lymphoma: the South- 70 years with unfavorable non-Hodgkin's lymphoma. J Clin On-
west Oncology Group experience. J Clin Oncol 1986; 4:295-305. col 1992; 10:228-236.
169. Coiffier B, Gisselbrecht C, Vose JM, et al. Prognostic factors in 175. Coiffier B, Gisselbrecht C , Bosly A , et al. Treatment of aggres-
aggressive malignant lymphomas. Description and validation of a sive lymphomas in patients older than 69 years. First interim
prognostic index that could identify patients requiring a more report of a randomized study from the GELA. Proceeding of the
intensive therapy. J Clin Oncol 1991; 9:211-219. Fourth International Conference on Malignant Lymphoma. June
170. Danieu L, Wong G , Koziner B , et al. Predictive model for 6-9, 1990; Lugano, Switzerland [abstract 82].
prognosis in advanced diffuse histiocytic lymphoma. Cancer Res 176. McMaster ML, Johnson D H , Greer JP, et al. A brief-duration
1986; 46:5372-5379. combination chemotherapy for elderly patients with poor-progno-
171. Velasquez WS, Jagannath S, Tucker SL, et al. Risk classifica- sis non-Hodgkin's lymphoma. Cancer 1992; 67:1487-1492.
tion as the basis for clinical staging of diffuse large-cell lymphoma 177. Sonneveld P. Michiels JJ. Full dose chemotherapy in elderly
derived from 10-year survival data. Blood 1989; 74:551-557. patients with non-Hodgkin's lymphoma. A feasibility study using
172. Dumontet C , Anderson J R , Sebban C , et al. Elderly non- a mitoxantrone containing regimen. Br J Cancer 1990; 6 2 : 1 0 5 -
Hodgkin's lymphoma patients have comparable prognostic factors 108.
but a poorer outcome than younger patients, [abstract] Proc A m 178. Gaynor E R , Dahlberg S, Fisher RI. Factors affecting reduced
Soc Clin Oncol 1992; 11:328. survival of the elderly with intermediate and high-grade lym-
173- O'Reilly SE, Klimo P, Connors JM. Low-dose ACOP-B and phoma; an analysis of S W O G 8516 (INT 0067)—The National
VABE weekly chemotherapy for elderly patients with advanced- High- Priority Lymphoma Study—a randomized comparison of
stage diffuse large-cell lymphoma. J Clin Oncol 1991; 9:741-747. CHOP vs m-BACOD vs ProMACE-CytaBOM vs MACOP-B
174. Hrelli U , Zagonel V, Errante D , et al. A prospective study of a [abstract]. Proc A m Soc Clin Oncol 1994; 13:1250.
new combination chemotherapy regimen in patients older than
SI-42 CLEVELAND CLINIC JOURNAL OF MEDICINE VOLUME 62 • SUPPLEMENT I
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5814)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (845)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- 4 Meconium Aspiration SyndromeDocument30 pages4 Meconium Aspiration SyndromeRana Vandana100% (2)
- 2020-11-25 New Enzyplex - Prof. Marcel - The Role of Digestive Enzymes Supplement in FunctionalDocument54 pages2020-11-25 New Enzyplex - Prof. Marcel - The Role of Digestive Enzymes Supplement in Functionalgraha internaNo ratings yet
- DRUG STUDY (FLUoxetine)Document2 pagesDRUG STUDY (FLUoxetine)Diana Villanueva100% (1)
- Infants With Motor DelaysDocument42 pagesInfants With Motor Delaysdona saputriNo ratings yet
- Ava Paravati Paradigm Shift PaperDocument15 pagesAva Paravati Paradigm Shift Paperapi-607803514No ratings yet
- CHAPTER 2 Infectious EpidemiologyDocument89 pagesCHAPTER 2 Infectious EpidemiologyteklayNo ratings yet
- Visual Concept MappingDocument2 pagesVisual Concept MappingMaria Ellah C. BELASOTONo ratings yet
- Pir June 2015, Volume 36, Issue 6Document55 pagesPir June 2015, Volume 36, Issue 6Angie LuperdiNo ratings yet
- .Document33 pages.3bdullah al3yuniNo ratings yet
- 6 Endometrial Polyp - Libre PathologyDocument4 pages6 Endometrial Polyp - Libre PathologyfadoNo ratings yet
- Multiple Sclerosis (MS)Document15 pagesMultiple Sclerosis (MS)Arianna Jasmine MabungaNo ratings yet
- Páginas Desde A Stepwise Approach To The Interpretation of Pulmonary Function Tests-4Document1 pagePáginas Desde A Stepwise Approach To The Interpretation of Pulmonary Function Tests-4Sotfonic SotfonicNo ratings yet
- NCP Proper 1Document6 pagesNCP Proper 1Noreen PinedaNo ratings yet
- Drugs Used in The Treatment of CoughDocument12 pagesDrugs Used in The Treatment of CoughMaryam NisaNo ratings yet
- Acute Pain Nursing Care PlanDocument3 pagesAcute Pain Nursing Care PlanSiafei RabeNo ratings yet
- Quiz 2 Obstetrics Nursing: Untitled SectionDocument11 pagesQuiz 2 Obstetrics Nursing: Untitled SectionBeverly DatuNo ratings yet
- Magnesium Chloride Hex A Hydrate TherapyDocument2 pagesMagnesium Chloride Hex A Hydrate TherapyDora L. Gutierrez100% (1)
- El PsaDocument2 pagesEl PsaMaherNo ratings yet
- ChondroblastomaDocument19 pagesChondroblastomaronnyNo ratings yet
- Acute Subdural Hematoma Because of Boxing.2Document6 pagesAcute Subdural Hematoma Because of Boxing.2Mon ChávezNo ratings yet
- Safety SbmaDocument12 pagesSafety SbmaDlraje DlrajeNo ratings yet
- Prostate CancerDocument6 pagesProstate CancerfheisanzNo ratings yet
- Total Anomalous Pulmonary Venous Connection (TAPVC)Document2 pagesTotal Anomalous Pulmonary Venous Connection (TAPVC)Tri RachmadijantoNo ratings yet
- NCG Guidelines 2020: Paediatric Hematolymphoid and Solid TumoursDocument46 pagesNCG Guidelines 2020: Paediatric Hematolymphoid and Solid TumoursSudipto BhattacharyaNo ratings yet
- Basic of Ophthalmology ExaminationsDocument47 pagesBasic of Ophthalmology ExaminationsAnonymous iy7I3o100% (2)
- Learning Material RLE NCM 112Document5 pagesLearning Material RLE NCM 112shiro the catNo ratings yet
- TYPES Khushi PatelDocument17 pagesTYPES Khushi PatelMeet PatelNo ratings yet
- CestodesDocument4 pagesCestodesJurel GaoatNo ratings yet
- Cancer ClassificationDocument10 pagesCancer ClassificationMuhamad Asymawi SuhaiminNo ratings yet
- Spinal Surgery Laminectomy Fusion AHM 1Document14 pagesSpinal Surgery Laminectomy Fusion AHM 1Rashmi ShriNo ratings yet