You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5819)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (845)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- Cycles For Pennies - DoggCrapp (DC) TrainingDocument698 pagesCycles For Pennies - DoggCrapp (DC) Traininggiantslor93% (15)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Rabisanto Trishviola Joy C. CHAPTER 9 EXERCISESDocument6 pagesRabisanto Trishviola Joy C. CHAPTER 9 EXERCISESLiza Aingelica100% (1)
- NLP ComprehensiveDocument6 pagesNLP Comprehensivesam_bhopNo ratings yet
- Guidelines For Social Work Case Management DocumentationDocument10 pagesGuidelines For Social Work Case Management DocumentationBetty Weese Holdread100% (2)
- DraftDocument6 pagesDraftLiza AingelicaNo ratings yet
- ResearchDocument2 pagesResearchLiza AingelicaNo ratings yet
- Concepts and Pattern of Human BehaviorDocument59 pagesConcepts and Pattern of Human BehaviorLiza AingelicaNo ratings yet
- A. Definition: Santos, Jianne Kyra E. BSN Iii-BDocument5 pagesA. Definition: Santos, Jianne Kyra E. BSN Iii-BLiza AingelicaNo ratings yet
- IVF: What Does It Involve?Document29 pagesIVF: What Does It Involve?Liza AingelicaNo ratings yet
- Highly Potent Heavy Chain Only Antibodies Protect Against Mers-Cov InfectionDocument1 pageHighly Potent Heavy Chain Only Antibodies Protect Against Mers-Cov InfectionLiza AingelicaNo ratings yet
- Bio Begavioral Interventions and Holistic Care For Individuals and Family With Specific Problems in Oxygenation, Fluid and Electrolyte Balance, Metabolic and Endocrine FuntionDocument16 pagesBio Begavioral Interventions and Holistic Care For Individuals and Family With Specific Problems in Oxygenation, Fluid and Electrolyte Balance, Metabolic and Endocrine FuntionLiza AingelicaNo ratings yet
- TFN 11-12-18 LectureDocument1 pageTFN 11-12-18 LectureLiza AingelicaNo ratings yet
- Sexually Transmitted Diseases: Jasmin P. EgargueDocument33 pagesSexually Transmitted Diseases: Jasmin P. EgargueLiza AingelicaNo ratings yet
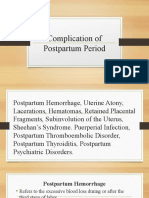
- Complication of Postpartum PeriodDocument115 pagesComplication of Postpartum PeriodLiza Aingelica100% (1)
- Ethico-Legal Issues in The Care of Mother On Reproductive TechniquesDocument2 pagesEthico-Legal Issues in The Care of Mother On Reproductive TechniquesLiza AingelicaNo ratings yet
- Drug StudyDocument1 pageDrug StudyLiza AingelicaNo ratings yet
- Evaluation of Progress and Outcome of Care: SERRANO, Jimuel FDocument29 pagesEvaluation of Progress and Outcome of Care: SERRANO, Jimuel FLiza AingelicaNo ratings yet
- Communication Processes Principles and EthicsDocument27 pagesCommunication Processes Principles and EthicsLiza AingelicaNo ratings yet
- Basketball HandoutsDocument18 pagesBasketball HandoutsLiza AingelicaNo ratings yet
- Laguna State Polytechnic University: Final Requirements 1. Study The Basic Basketball Referee Hand Signals Posted BelowDocument3 pagesLaguna State Polytechnic University: Final Requirements 1. Study The Basic Basketball Referee Hand Signals Posted BelowLiza AingelicaNo ratings yet
- Clinical Analysis REDUTADocument1 pageClinical Analysis REDUTALiza AingelicaNo ratings yet
- Factors Affecting Students Preference of Nursing Education in SiDocument104 pagesFactors Affecting Students Preference of Nursing Education in SiLiza AingelicaNo ratings yet
- DRL Annual Report Fy2021Document143 pagesDRL Annual Report Fy2021nischal mathurNo ratings yet
- ARC-GEN-FM-14 - Daily Sanitation Audit FormDocument4 pagesARC-GEN-FM-14 - Daily Sanitation Audit FormRizwan SiddiqiNo ratings yet
- KIM ABP Awkward Body PosturesDocument4 pagesKIM ABP Awkward Body PosturesJerra Belle C. AtasNo ratings yet
- Marketing Management Department Unilab Sales Management Procedure (Sales Management Procedure)Document36 pagesMarketing Management Department Unilab Sales Management Procedure (Sales Management Procedure)Jan AcostaNo ratings yet
- Monroe County Migrant Housing State of EmergencyDocument2 pagesMonroe County Migrant Housing State of EmergencyTyler DiedrichNo ratings yet
- TASK 1 (A)Document13 pagesTASK 1 (A)double keatNo ratings yet
- Jsa Micet FypDocument22 pagesJsa Micet FypAmirou RaizoNo ratings yet
- S - Aicte Activity PointsDocument9 pagesS - Aicte Activity Pointsvjy stvkbNo ratings yet
- Molecular Laboratory: Philippine Red CrossDocument4 pagesMolecular Laboratory: Philippine Red CrossVianne MagsinoNo ratings yet
- Abela - Adult Learning PDFDocument7 pagesAbela - Adult Learning PDFDhiaul IzzahNo ratings yet
- Limited F2F Contingency Plan - SanLuisNHSDocument35 pagesLimited F2F Contingency Plan - SanLuisNHSRuel Gonzales Jr.No ratings yet
- Goto 2019Document6 pagesGoto 2019Marmox Lab.No ratings yet
- Curriculum Mapping T.L.E7SJBPSDocument11 pagesCurriculum Mapping T.L.E7SJBPSKevin SenoNo ratings yet
- Listening Exercises: A. She Crashed Her Bicycle B. She Crashed Her Car C. She Crashed Her Mother's CarDocument2 pagesListening Exercises: A. She Crashed Her Bicycle B. She Crashed Her Car C. She Crashed Her Mother's CarSilvia CanoNo ratings yet
- Vet Radiology Ultrasound - 2020 - Lin - Computed Tomographic Lymphangiography Via Intra Metatarsal Pad Injection IsDocument9 pagesVet Radiology Ultrasound - 2020 - Lin - Computed Tomographic Lymphangiography Via Intra Metatarsal Pad Injection IsCésar Sa JimNo ratings yet
- Novy 2019Document7 pagesNovy 2019Gabriela Marie CruzNo ratings yet
- Radically Open Dialectical Behavior Therapy Theory and Practice For Treating Disorders of OvercontrolDocument553 pagesRadically Open Dialectical Behavior Therapy Theory and Practice For Treating Disorders of OvercontrolClarisse Pamplona Garcia100% (1)
- TLE Nutri-QuizDocument8 pagesTLE Nutri-QuizmeasdfNo ratings yet
- أثر ضغوط العمل على أداء العاملينDocument32 pagesأثر ضغوط العمل على أداء العاملينMr. SalahNo ratings yet
- Pedendo Proceedings Book Foutput Ok 2019 Permasalahan Dalam Skrining Hipotiroid Kongenital DiDocument186 pagesPedendo Proceedings Book Foutput Ok 2019 Permasalahan Dalam Skrining Hipotiroid Kongenital DiDamar Prasetya, Sp.ANo ratings yet
- References: Technostress: How Does It Affect You?Document2 pagesReferences: Technostress: How Does It Affect You?coconutcrabNo ratings yet
- Behavior Modification Treatment PhaseDocument5 pagesBehavior Modification Treatment PhaseMeredith EckardNo ratings yet
- Duncan - 2003 - SHELLFISHCommercially Important MolluscsDocument7 pagesDuncan - 2003 - SHELLFISHCommercially Important MolluscsDaniel OviedoNo ratings yet
- Principles and Practices of Palliative CareDocument19 pagesPrinciples and Practices of Palliative CareDisala RanaweeraNo ratings yet
- Charles DissertationDocument81 pagesCharles DissertationMhlanga Bridget TanyaradzwaNo ratings yet
- Benefits of SMART Therapy For Asthma ManagementDocument4 pagesBenefits of SMART Therapy For Asthma ManagementREDANo ratings yet
- StanCo Resouces - 2011Document26 pagesStanCo Resouces - 2011MariaCQNo ratings yet