You might also like
- Essentials of Dentistry PDFDocument327 pagesEssentials of Dentistry PDFdianelsbth100% (4)
- Midline Diastema PDFDocument33 pagesMidline Diastema PDFheycoolalex100% (1)
- Open Bite, A Review of Etiology and Manageme PDFDocument8 pagesOpen Bite, A Review of Etiology and Manageme PDFVieussens JoffreyNo ratings yet
- Differential Diagnosis of Tongue LesionsDocument12 pagesDifferential Diagnosis of Tongue LesionsKartikakhairaniNo ratings yet
- Oral Medicine & Pathology from A-ZFrom EverandOral Medicine & Pathology from A-ZRating: 5 out of 5 stars5/5 (9)
- Diastema Closure With Direct Composite Architectural Gingival Contouring.20150306122816Document6 pagesDiastema Closure With Direct Composite Architectural Gingival Contouring.20150306122816Rossye MpfNo ratings yet
- Clinical Case Presentation Sample McqsDocument10 pagesClinical Case Presentation Sample McqsDr.yamini Nag Kantipudi100% (2)
- Crestal Bone Changes On Platform - Switched Implants and Adjacent Teeth When The Tooth-Implant Distance Is Less Than 1.5 MMDocument10 pagesCrestal Bone Changes On Platform - Switched Implants and Adjacent Teeth When The Tooth-Implant Distance Is Less Than 1.5 MMJuanOso Gutierrez ArayaNo ratings yet
- FCMFOS (SA) Final Past Papers - 2016 2nd Semester 19-4-2018Document1 pageFCMFOS (SA) Final Past Papers - 2016 2nd Semester 19-4-2018Isak Isak IsakNo ratings yet
- Diagnosis Dilemmas in Vital Pulp Therapy Treatment For The Toothache Is Changing.Document10 pagesDiagnosis Dilemmas in Vital Pulp Therapy Treatment For The Toothache Is Changing.khawla boukhNo ratings yet
- Management of Midline DiastemaDocument20 pagesManagement of Midline DiastemaHitesh ChopraNo ratings yet
- Etiology and Treatment of Midline DiastemaDocument3 pagesEtiology and Treatment of Midline DiastemaPuteri NazirahNo ratings yet
- EMS Dentistry Journal: Maxillary Midline Diastema: A Contemporary ReviewDocument12 pagesEMS Dentistry Journal: Maxillary Midline Diastema: A Contemporary ReviewMutiaRamadhantiiNo ratings yet
- Direct CompositDocument8 pagesDirect CompositJulianna BartalusNo ratings yet
- Huang 17 03 PDFDocument9 pagesHuang 17 03 PDFZita AprilliaNo ratings yet
- 24-Article Text-69-2-10-20170727Document5 pages24-Article Text-69-2-10-20170727Monwarul AzizNo ratings yet
- Anagement of Space Problems in The Primary and Mixed DentitionsDocument10 pagesAnagement of Space Problems in The Primary and Mixed Dentitionsjing.zhao222No ratings yet
- Midline Diastema Treatment OptionsDocument6 pagesMidline Diastema Treatment OptionsnandaNo ratings yet
- Mesiodens Etiology, Prevalence, Diagnosis and ManagementDocument4 pagesMesiodens Etiology, Prevalence, Diagnosis and ManagementsyedNo ratings yet
- Mesiodens PDFDocument5 pagesMesiodens PDFSamNo ratings yet
- Mesiodens PDFDocument5 pagesMesiodens PDFNishtha KumarNo ratings yet
- DiastemaDocument29 pagesDiastemaPZNo ratings yet
- Midline DiastemaDocument4 pagesMidline DiastemasmritiNo ratings yet
- Periodontal Treatment of Excessive Gingival Display: Ramzi V. Abou-Arraj, DDS, MS, and Nada M. Souccar, DDS, MSDocument12 pagesPeriodontal Treatment of Excessive Gingival Display: Ramzi V. Abou-Arraj, DDS, MS, and Nada M. Souccar, DDS, MSvaleriaNo ratings yet
- Article 1525485399Document4 pagesArticle 1525485399anisah fadilahNo ratings yet
- Orthodontic Approach To Mid-Line DiastemaDocument33 pagesOrthodontic Approach To Mid-Line DiastemaNikola DerebanNo ratings yet
- JCPD 32 4 j087t33221771387Document8 pagesJCPD 32 4 j087t33221771387Anuette Mayoral GarciaNo ratings yet
- Canine Impaction A Review of The Prevalence, Etiology, Diagnosis and TreatmentDocument7 pagesCanine Impaction A Review of The Prevalence, Etiology, Diagnosis and TreatmentFadiShihabNo ratings yet
- Dent Update 2008 35 636-641 PDFDocument5 pagesDent Update 2008 35 636-641 PDFbkprosthoNo ratings yet
- Dent Update 2008 35 636-641Document5 pagesDent Update 2008 35 636-641bkprosthoNo ratings yet
- Pugliese2019 Black Triangles - Preventing Their Occurrence, Managing Them When Prevention Is Not PracticalDocument12 pagesPugliese2019 Black Triangles - Preventing Their Occurrence, Managing Them When Prevention Is Not Practicalsolodont1No ratings yet
- 740 Mac NamaraDocument7 pages740 Mac NamaraAnamerc LanderNo ratings yet
- Post RetentionDocument7 pagesPost RetentionGieh SyafitriNo ratings yet
- Dental Twinning in Primary Dentition A Case ReportDocument4 pagesDental Twinning in Primary Dentition A Case ReporthaidirNo ratings yet
- Differential Diagnosis of Tongue Lesions: Quintessence International June 2003Document13 pagesDifferential Diagnosis of Tongue Lesions: Quintessence International June 2003Sidney QuinceNo ratings yet
- Ijcmr Jul Sep 5 2014Document16 pagesIjcmr Jul Sep 5 2014Kimberly Zeña MadridNo ratings yet
- Jurnal SP KTK 2Document4 pagesJurnal SP KTK 2thasya sumerahNo ratings yet
- 5-Management of Space ProblemsDocument10 pages5-Management of Space ProblemsMuhammad UzairNo ratings yet
- Marschall Pediatric TraumaDocument7 pagesMarschall Pediatric TraumaRicardo GrilloNo ratings yet
- VanderwoudesyndromeDocument3 pagesVanderwoudesyndromeDrSharan AnatomistNo ratings yet
- Sindrome Desostose Cleidocraniana-Trat OrtodDocument8 pagesSindrome Desostose Cleidocraniana-Trat Ortodbeh.chaves16No ratings yet
- Bimaxilary ProtrusionDocument7 pagesBimaxilary ProtrusionD YasIr MussaNo ratings yet
- Resume InggrisDocument2 pagesResume InggrisGurnitaswastiNo ratings yet
- Conservative ManagementDocument4 pagesConservative ManagementFatima AliNo ratings yet
- Ipdoaj MS Id 000113Document3 pagesIpdoaj MS Id 000113Ayu DamayNo ratings yet
- DR Sadia Article 2003 VERSIONDocument5 pagesDR Sadia Article 2003 VERSIONMahnoor ShafiqNo ratings yet
- Woodworth1985 PDFDocument14 pagesWoodworth1985 PDFacevariel5851No ratings yet
- Midline ShiftDocument6 pagesMidline ShiftMaiush JbNo ratings yet
- Digital Smile Design ConceptDocument19 pagesDigital Smile Design ConceptDiego GomesNo ratings yet
- Lib BumpersDocument3 pagesLib BumpersDaniel Garcia von BorstelNo ratings yet
- Shamita Sivarajoo d21100770Document19 pagesShamita Sivarajoo d21100770bdsaimstb17No ratings yet
- Management of Midline Facial CleftsDocument8 pagesManagement of Midline Facial CleftsBeatriz ChilenoNo ratings yet
- 2015 DU - Consv Managment of MacrodontiaDocument4 pages2015 DU - Consv Managment of MacrodontiaGeorge JoseNo ratings yet
- OrthodonticDocument3 pagesOrthodonticFirma Nurdinia DewiNo ratings yet
- The Acrocallosal Syndrome: A Case Report and Literature SurveyDocument9 pagesThe Acrocallosal Syndrome: A Case Report and Literature SurveyScott LoveNo ratings yet
- Peds Oral MedDocument18 pagesPeds Oral MedrossaNo ratings yet
- Jurnal LBM 4 1Document18 pagesJurnal LBM 4 1viral newNo ratings yet
- Articol EPRDocument7 pagesArticol EPRIoana MurariuNo ratings yet
- Sajnani, 2015Document7 pagesSajnani, 2015Julio AbarzuaNo ratings yet
- Case Report: Deema Alshammery and Hanan AlghmadiDocument2 pagesCase Report: Deema Alshammery and Hanan AlghmadiGieh SyafitriNo ratings yet
- Case Report: Ramachandra Jaya Agali, Nidhi.K.Nihal Miloni S VoraDocument3 pagesCase Report: Ramachandra Jaya Agali, Nidhi.K.Nihal Miloni S VoraWafa FoufaNo ratings yet
- DiastemaDocument14 pagesDiastemaPutri Morteza0% (1)
- Prosthetic Treatments For Patients With Ectodermal DysplasiaDocument5 pagesProsthetic Treatments For Patients With Ectodermal DysplasiaJawad TariqNo ratings yet
- 22 Accidental Periapical Extrusion of Non-Setting Calcium Hydroxide Unusual Bone Response and ManagementDocument6 pages22 Accidental Periapical Extrusion of Non-Setting Calcium Hydroxide Unusual Bone Response and ManagementbradbiancaionelaNo ratings yet
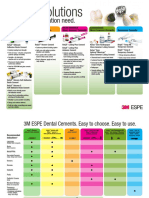
- Relyx Product ChartDocument2 pagesRelyx Product ChartRicardo Cenicante0% (1)
- 18 Lower Left First Molar Case Study PDFDocument3 pages18 Lower Left First Molar Case Study PDFAndreea GramaNo ratings yet
- Erythematous Candidiasis PDFDocument2 pagesErythematous Candidiasis PDFPatrickNo ratings yet
- Tooth Numbering SystemDocument19 pagesTooth Numbering Systemحسين الفلاحNo ratings yet
- Critters Table MannersDocument3 pagesCritters Table Mannersapi-248006371No ratings yet
- Perawatan Saluran Akar Gigi Desidui DanDocument14 pagesPerawatan Saluran Akar Gigi Desidui DanPipin HeryantoNo ratings yet
- Scaling and Root Planing - WikipediaDocument6 pagesScaling and Root Planing - WikipediaSadia ArovaNo ratings yet
- New Microsoft Office Word DocumentDocument3 pagesNew Microsoft Office Word DocumentAtulsanapNo ratings yet
- ECOHISDocument8 pagesECOHISNguyễn Hồng HạnhNo ratings yet
- Esthetic Approaches in RPD: 1. Gingival Approaching RetainerDocument2 pagesEsthetic Approaches in RPD: 1. Gingival Approaching Retainereili1No ratings yet
- Full Ebook of Contemporary Fixed Prosthodontics 6Th Edition Stephen F Rosenstiel Online PDF All ChapterDocument69 pagesFull Ebook of Contemporary Fixed Prosthodontics 6Th Edition Stephen F Rosenstiel Online PDF All Chaptercordyaloce722100% (4)
- DappusDocument2 pagesDappusAdzra Shafwa NabilaNo ratings yet
- Articulador Manual IngDocument8 pagesArticulador Manual IngIlich GarayNo ratings yet
- Casebook IconVE 07022019 enDocument45 pagesCasebook IconVE 07022019 envanity fairNo ratings yet
- Three-Dimensional Assessment of Virtual Bracket Removal For Orthodontic Retainers: A Prospective Clinical StudyDocument10 pagesThree-Dimensional Assessment of Virtual Bracket Removal For Orthodontic Retainers: A Prospective Clinical StudyAndré DrumondNo ratings yet
- GTPTDocument5 pagesGTPTNelly SuriamahNo ratings yet
- Assigned by Plan Named in #3Document2 pagesAssigned by Plan Named in #3olimaziNo ratings yet
- 4.2 Prosthetic Management of Implants in The Esthetic Zone: General Principles and Scientific DocumentationDocument37 pages4.2 Prosthetic Management of Implants in The Esthetic Zone: General Principles and Scientific DocumentationJennifer ChenNo ratings yet
- Andersson 2003Document6 pagesAndersson 2003IngrydCamposNo ratings yet
- Orthognathic Surgery Correction of Dentofacial DeformitiesDocument14 pagesOrthognathic Surgery Correction of Dentofacial Deformitiesmarina.huppiNo ratings yet
- Journal Club I: Methods To Check Occlusal Clearance During Tooth PreparationDocument16 pagesJournal Club I: Methods To Check Occlusal Clearance During Tooth Preparationshaikhhumaira08No ratings yet
- Dental Hygiene: Healthy Smiles Lesson PlanDocument3 pagesDental Hygiene: Healthy Smiles Lesson PlangggregorieNo ratings yet
- 10 Brook Shaw 1989 IOTN EvaluationDocument12 pages10 Brook Shaw 1989 IOTN EvaluationSankhyaNo ratings yet
- Komatsu Hydraulic Excavator Pc4000 11 t4 Deu Gzeam08246 1 Shop ManualDocument22 pagesKomatsu Hydraulic Excavator Pc4000 11 t4 Deu Gzeam08246 1 Shop Manualmorganthomas160591ekr100% (65)
- Orthodontic Treatment of Anterior Open Bite: Chui Shan Teresa NG, Wing Kit Ricky Wong & Urban HaggDocument6 pagesOrthodontic Treatment of Anterior Open Bite: Chui Shan Teresa NG, Wing Kit Ricky Wong & Urban HaggLAINo ratings yet