You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (843)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5809)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (346)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Clinical Assessment of Self-InjuryDocument13 pagesClinical Assessment of Self-InjuryAdriana Marcela Rogelis PradaNo ratings yet
- IPIECA - IOGP - Oil Spill Response Introduction - GPGDocument24 pagesIPIECA - IOGP - Oil Spill Response Introduction - GPGseawolf50No ratings yet
- Medical AbbreviationsDocument7 pagesMedical AbbreviationsBilly Braine Kho BanlatNo ratings yet
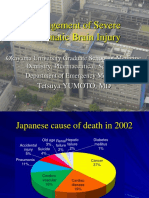
- Management of Severe Traumatic Brain InjuryDocument29 pagesManagement of Severe Traumatic Brain InjuryAndi Upik FathurNo ratings yet
- Acute Coronary Syndrome NCP 01Document5 pagesAcute Coronary Syndrome NCP 01AgronaSlaughter0% (1)
- Intranatal Assessment FormatDocument10 pagesIntranatal Assessment FormatAnnapurna Dangeti100% (1)
- Diabetes MellitusDocument64 pagesDiabetes MellitusCris Tine67% (6)
- 2021 Global Korea Scholarship: Application ChecklistDocument12 pages2021 Global Korea Scholarship: Application ChecklisttemesgenNo ratings yet
- Haccpfinalplan 190318173536Document81 pagesHaccpfinalplan 190318173536sutharitessh100% (1)
- GVPIH VisakhapatnamDocument7 pagesGVPIH VisakhapatnamManoj KashyapNo ratings yet
- Flaws Diagnosis 171 178Document8 pagesFlaws Diagnosis 171 178mamun31No ratings yet
- SEATWORK - Recommended Energy and Nutrient Intakes (RENI) (GARBOSA, RM)Document1 pageSEATWORK - Recommended Energy and Nutrient Intakes (RENI) (GARBOSA, RM)Rej GarbosaNo ratings yet
- Nselkirk Learning PlanDocument7 pagesNselkirk Learning Planapi-313720439No ratings yet
- Imprafix 2582 06354947 EN GBDocument13 pagesImprafix 2582 06354947 EN GBregNo ratings yet
- 100 Benefits of MeditationDocument5 pages100 Benefits of MeditationYogesh ThakkarNo ratings yet
- Drugs Against SARS-CoV-2: What Do We Know About Their Mode of Action?Document10 pagesDrugs Against SARS-CoV-2: What Do We Know About Their Mode of Action?Jorge Lopez C.No ratings yet
- Surgeon Should Learn Not Just How To Operate But How To Create System of CareDocument14 pagesSurgeon Should Learn Not Just How To Operate But How To Create System of Careamal.fathullahNo ratings yet
- 11 Core Elements of Evidence - Based Gerontological Nursing PracticeDocument29 pages11 Core Elements of Evidence - Based Gerontological Nursing PracticeSteffiNo ratings yet
- BSMMU Result July 2013Document33 pagesBSMMU Result July 2013Toufiq HassanNo ratings yet
- Who DMP RGS 98 5 RDocument208 pagesWho DMP RGS 98 5 Rtamara_0021No ratings yet
- Caring For A ColostomyDocument16 pagesCaring For A ColostomyElaine Frances IlloNo ratings yet
- Dehumanization Is The Worst Impact. Berube Explains. This Means-Ends Dispute Is at The Core ofDocument4 pagesDehumanization Is The Worst Impact. Berube Explains. This Means-Ends Dispute Is at The Core ofdeankiesermanNo ratings yet
- Patient Recruitment Workshop: Global Issues in Patient Recruitment and Retention: Challenges and SolutionsDocument54 pagesPatient Recruitment Workshop: Global Issues in Patient Recruitment and Retention: Challenges and SolutionsKrishnaNo ratings yet
- Patient Release Form ("Release")Document2 pagesPatient Release Form ("Release")Junizar fzNo ratings yet
- Gul Et Al (2017) - Body-Image-Self-Esteem-And-Quality-Of-Life-In-Vitiligo-PatientsDocument6 pagesGul Et Al (2017) - Body-Image-Self-Esteem-And-Quality-Of-Life-In-Vitiligo-PatientsCarlos RodriguezNo ratings yet
- Alcohol Binge Drinking in OCDDocument2 pagesAlcohol Binge Drinking in OCDSuyash DwivediNo ratings yet
- dm2020 0186 Interim Guidelines On Operations of Converted P and P Spaces Into TTMF PDFDocument27 pagesdm2020 0186 Interim Guidelines On Operations of Converted P and P Spaces Into TTMF PDFSeriel TismoNo ratings yet
- Emerging Theories Into The Social Determinants of Health: Implications For Oral Health PromotionDocument7 pagesEmerging Theories Into The Social Determinants of Health: Implications For Oral Health PromotionEmmanuel PìnheiroNo ratings yet
- Deans Honors Program 2006 - XiaoChuanGuo As AssocProfDocument11 pagesDeans Honors Program 2006 - XiaoChuanGuo As AssocProfYingjie XuNo ratings yet
- 207 Research Proposal 1Document10 pages207 Research Proposal 1Jana WeshahiNo ratings yet