You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (120)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Occupational Therapy Assessments Quick TableDocument5 pagesOccupational Therapy Assessments Quick Tableredsmartie100% (3)
- Wellness ExamDocument6 pagesWellness ExamRUTH MAE GULENG100% (8)
- Wab ScreenerDocument3 pagesWab Screenerapi-2728164200% (1)
- Defining The Role of Social Workers in Diabetes CareDocument3 pagesDefining The Role of Social Workers in Diabetes CareLiliana RicoNo ratings yet
- UK Info & LabelDocument28 pagesUK Info & LabelJenn LamNo ratings yet
- NCP Ineffective CopingDocument3 pagesNCP Ineffective CopingAqua RentoNo ratings yet
- Treatment of Striae Distensae Using Needling TherapyDocument6 pagesTreatment of Striae Distensae Using Needling TherapyludyNo ratings yet
- Apta Membership CertificateDocument1 pageApta Membership Certificateapi-371785797No ratings yet
- Gradereport 2019-20 SummerDocument1 pageGradereport 2019-20 Summerapi-468018392No ratings yet
- Esophageal Cancer InserviceDocument18 pagesEsophageal Cancer Inserviceapi-371785797No ratings yet
- GradereportDocument1 pageGradereportapi-371785797No ratings yet
- Post Print Score ReportDocument1 pagePost Print Score Reportapi-371785797No ratings yet
- Gradereport 1Document1 pageGradereport 1api-371785797No ratings yet
- Exit Interview QuestionsDocument3 pagesExit Interview Questionsapi-371785797No ratings yet
- Gradereport 5Document1 pageGradereport 5api-371785797No ratings yet
- Mental Health Conference Series Cognitive and Behavioral Sequelae of Covid-19 InfectionDocument1 pageMental Health Conference Series Cognitive and Behavioral Sequelae of Covid-19 Infectionapi-371785797No ratings yet
- Part 1 Task A Field Observation - OsantowskiDocument6 pagesPart 1 Task A Field Observation - Osantowskiapi-371785797No ratings yet
- Case Report 1 Final Draft 12Document65 pagesCase Report 1 Final Draft 12api-371785797No ratings yet
- Greatest Moment Slide - Osantowski and SlocumDocument1 pageGreatest Moment Slide - Osantowski and Slocumapi-371785797No ratings yet
- Group PresentationDocument13 pagesGroup Presentationapi-371785797No ratings yet
- Self Assessment - Second Year 2019-2020Document4 pagesSelf Assessment - Second Year 2019-2020api-371785797No ratings yet
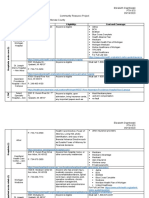
- Community Resource ProjectDocument9 pagesCommunity Resource Projectapi-371785797No ratings yet
- Gradereport 3Document1 pageGradereport 3api-371785797No ratings yet
- Jennifer Exercise ListDocument1 pageJennifer Exercise Listapi-371785797No ratings yet
- Updated Game PlanDocument3 pagesUpdated Game Planapi-371785797No ratings yet
- Reflective JournalDocument26 pagesReflective Journalapi-371785797No ratings yet
- Gradereport 2Document1 pageGradereport 2api-371785797No ratings yet
- Final Ethics Paper - OsantowskiDocument10 pagesFinal Ethics Paper - Osantowskiapi-371785797No ratings yet
- GradereportDocument1 pageGradereportapi-467445554No ratings yet
- Case Report - Osantowski and AyacheDocument14 pagesCase Report - Osantowski and Ayacheapi-371785797No ratings yet
- Ptso Leadership 2018-2019Document1 pagePtso Leadership 2018-2019api-371785797No ratings yet
- Exam 4 Study Guide - Eo JTZDocument16 pagesExam 4 Study Guide - Eo JTZapi-371785797No ratings yet
- Ptso Certification 2018-2019Document1 pagePtso Certification 2018-2019api-371785797No ratings yet
- Citi - OsantowskiDocument1 pageCiti - Osantowskiapi-371785797No ratings yet
- Osantowski Rolling-Teaching Activity Paper 1Document11 pagesOsantowski Rolling-Teaching Activity Paper 1api-371785797No ratings yet
- Osantowski Pre 2019 2Document7 pagesOsantowski Pre 2019 2api-371785797No ratings yet
- Adls Final Research PosterDocument1 pageAdls Final Research Posterapi-453651228No ratings yet
- 15 PharmaDocument32 pages15 PharmaGilbert OfeiNo ratings yet
- Issue On HazingDocument4 pagesIssue On HazingBeverly TalaugonNo ratings yet
- Critical Limb IschemiaDocument11 pagesCritical Limb IschemiaAmalia Hendar PangestutiNo ratings yet
- Kratom PosterDocument1 pageKratom Poster4pavlikNo ratings yet
- Chapter 1 - The Nature and Content of General Practice: DefinitionsDocument9 pagesChapter 1 - The Nature and Content of General Practice: Definitionsprofarmah6150No ratings yet
- Periodontal Research PaperDocument8 pagesPeriodontal Research Paperapi-279944111No ratings yet
- Geriatric RehabilitationDocument31 pagesGeriatric RehabilitationsmrutiptNo ratings yet
- Assisting IV BTDocument89 pagesAssisting IV BTmhelshy villanuevaNo ratings yet
- Understanding Burn Injury 508 - 0Document6 pagesUnderstanding Burn Injury 508 - 0Thanujaa UvarajNo ratings yet
- Respiratory Failure (Aan) PDFDocument19 pagesRespiratory Failure (Aan) PDFYudionoNo ratings yet
- Manda Rag atDocument6 pagesManda Rag atlapNo ratings yet
- Miguez & Laborda (2015, Exposure and Response Prevention)Document9 pagesMiguez & Laborda (2015, Exposure and Response Prevention)Sebastian ChaconNo ratings yet
- WJCP 5 143Document9 pagesWJCP 5 143BudiNo ratings yet
- ACLS ScenarioDocument21 pagesACLS Scenariomarves15No ratings yet
- Assignment 1Document13 pagesAssignment 1林佑邦No ratings yet
- Dance Movement Therapy PDFDocument7 pagesDance Movement Therapy PDFanaghaNo ratings yet
- CV Format AimeeDocument4 pagesCV Format Aimeeapp_12003100% (9)
- Preparation & Evaluation of Silver Sulfadiazine (SSD) Loaded Liposomal Topical GelsDocument3 pagesPreparation & Evaluation of Silver Sulfadiazine (SSD) Loaded Liposomal Topical Gelsakedia1No ratings yet
- Formulating A Dental Treatment Plan: DR Tashnim BagusDocument33 pagesFormulating A Dental Treatment Plan: DR Tashnim BagustarekrabiNo ratings yet
- Asuhan KefarmasianDocument45 pagesAsuhan Kefarmasiankamar obat pkm tamanNo ratings yet
- Cardiorenal SyndromeDocument18 pagesCardiorenal SyndromefelipetheNo ratings yet
- PerdevDocument33 pagesPerdevBatchie Bugs StuartNo ratings yet