You might also like
- Naplex Complete Study Outline A Topic-Wise Approach DiabetesFrom EverandNaplex Complete Study Outline A Topic-Wise Approach DiabetesRating: 4 out of 5 stars4/5 (2)
- Derosa 2010 InfDocument5 pagesDerosa 2010 InfJuan Carlos FloresNo ratings yet
- Complementary and Alternative Medical Lab Testing Part 18: PsychiatryFrom EverandComplementary and Alternative Medical Lab Testing Part 18: PsychiatryRating: 5 out of 5 stars5/5 (1)
- Jurnal 333Document11 pagesJurnal 333Friska Rachmanita PrayogoNo ratings yet
- Khowaja2018 Article GlycemicControlInHospitalizedP PDFDocument9 pagesKhowaja2018 Article GlycemicControlInHospitalizedP PDFMade Dedy KusnawanNo ratings yet
- Shirure Et AlDocument7 pagesShirure Et AleditorijmrhsNo ratings yet
- Roberto Fogari, MD Annalisa Zoppi, MD Amedeo Mugellini, MD Paola Preti, MD Maurizio Destro, MD Andrea Rinaldi, MD and Giuseppe Derosa, MDDocument15 pagesRoberto Fogari, MD Annalisa Zoppi, MD Amedeo Mugellini, MD Paola Preti, MD Maurizio Destro, MD Andrea Rinaldi, MD and Giuseppe Derosa, MDdini hanifaNo ratings yet
- Effect of The GLP-1 Receptor Agonist Lixisenatide On Counter-Regulatory Responses To Hypoglycemia in Subjects With Insulin-Treated Type 2 DiabetesDocument8 pagesEffect of The GLP-1 Receptor Agonist Lixisenatide On Counter-Regulatory Responses To Hypoglycemia in Subjects With Insulin-Treated Type 2 DiabetestarietarooNo ratings yet
- Effectiveness and Metabolic Effects of Perindopril and Diuretics Combination in Primary HypertensionDocument5 pagesEffectiveness and Metabolic Effects of Perindopril and Diuretics Combination in Primary Hypertensionguugle gogleNo ratings yet
- Jurnal DMDocument5 pagesJurnal DMratihparmadiniNo ratings yet
- HypertensionDocument7 pagesHypertensionrohayatjohnNo ratings yet
- A Comparison of The Efficacy and Safety of irbesartan/HCTZ Combination Therapy With Irbesartan and HCTZ Monotherapy in The Treatment of Moderate HypertensionDocument9 pagesA Comparison of The Efficacy and Safety of irbesartan/HCTZ Combination Therapy With Irbesartan and HCTZ Monotherapy in The Treatment of Moderate HypertensionBarbara Sakura RiawanNo ratings yet
- VHRM 9 711 2Document7 pagesVHRM 9 711 2fenniebubuNo ratings yet
- Anethum Graveolens and Hyperlipidemia: A Randomized Clinical TrialDocument13 pagesAnethum Graveolens and Hyperlipidemia: A Randomized Clinical TrialYuliantikha Nurul QomariahNo ratings yet
- Amlodipine AtenololDocument7 pagesAmlodipine AtenololBidhur Chakma 1935371673No ratings yet
- 1395 13 6177 1 10 20171021Document11 pages1395 13 6177 1 10 20171021Dr. RajibNo ratings yet
- Alasan Ke ManusiaDocument12 pagesAlasan Ke ManusiaafiwahyuNo ratings yet
- A Nutraceutical Combination Improves Insulin Sensitivity in Patients With Metabolic SyndromeDocument7 pagesA Nutraceutical Combination Improves Insulin Sensitivity in Patients With Metabolic SyndromegiannidietNo ratings yet
- Insulin resistance icuDocument18 pagesInsulin resistance icuLucero GutierrezNo ratings yet
- Dietary protein restriction improves outcomes in diabetic nephropathyDocument9 pagesDietary protein restriction improves outcomes in diabetic nephropathyJose J.No ratings yet
- Assessment and Treatment of Hyperglycemia in Critically IllDocument6 pagesAssessment and Treatment of Hyperglycemia in Critically IllYousif ElmasryNo ratings yet
- NONE BDocument11 pagesNONE BPincelito21No ratings yet
- Dislipidemia en Pacientes TargaJIAS-17-19004Document5 pagesDislipidemia en Pacientes TargaJIAS-17-19004angelvpsNo ratings yet
- Effect of 1 Years Orlistat Treatment Compared To Placebo On Insulin Resistance Parameter in Patients With Type 2 DiabetesDocument9 pagesEffect of 1 Years Orlistat Treatment Compared To Placebo On Insulin Resistance Parameter in Patients With Type 2 Diabetesmuhammad ricky kurniawanNo ratings yet
- Amlodipine-10mg TabletDocument7 pagesAmlodipine-10mg TabletMd. Abdur RahmanNo ratings yet
- DEPICT 1 - T1D StudyDocument13 pagesDEPICT 1 - T1D StudyGVRNo ratings yet
- Indikasi Insulin InfusionDocument7 pagesIndikasi Insulin InfusionnikeNo ratings yet
- Accepted For Publication October 14, 2017. 0149-2918/$ - See Front Matter & 2017 Elsevier HS Journals, Inc. All Rights ReservedDocument14 pagesAccepted For Publication October 14, 2017. 0149-2918/$ - See Front Matter & 2017 Elsevier HS Journals, Inc. All Rights ReservedDianne GalangNo ratings yet
- Gracia Ramos2016Document8 pagesGracia Ramos2016Rahmanu ReztaputraNo ratings yet
- Metildopa NifedipinDocument3 pagesMetildopa NifedipinDendyNo ratings yet
- Combined: Therapy With Vasodilator Drugs and Beta-Adrenergic Blockade in HypertensionDocument13 pagesCombined: Therapy With Vasodilator Drugs and Beta-Adrenergic Blockade in Hypertensionshen6678No ratings yet
- Assessment of The Prevalence and Risk Factors Associated With Glucocorticoid-Induced Diabetes Mellitus in Pemphigus Vulgaris PatientsDocument6 pagesAssessment of The Prevalence and Risk Factors Associated With Glucocorticoid-Induced Diabetes Mellitus in Pemphigus Vulgaris PatientsRahma BachriNo ratings yet
- 10 Glycemic Control in Perioperative PeriodDocument5 pages10 Glycemic Control in Perioperative PeriodAna-Maria CroitoruNo ratings yet
- Arterioscler Thromb Vasc Biol-2000-Vehkavaara-545-50Document7 pagesArterioscler Thromb Vasc Biol-2000-Vehkavaara-545-50popopioNo ratings yet
- Noninsulin-Dependent Diabetes: Effects of Insulin Peripheral Splanchnic Glucose Metabolism in 11)Document7 pagesNoninsulin-Dependent Diabetes: Effects of Insulin Peripheral Splanchnic Glucose Metabolism in 11)agiekNo ratings yet
- Effects of Olanzapine and Haloperidol On The Metabolic Status of Healthy MenDocument8 pagesEffects of Olanzapine and Haloperidol On The Metabolic Status of Healthy MenBenjamin paulNo ratings yet
- Effect of Chlorpromazine and Haloperidol Combination on Lipid LevelsDocument10 pagesEffect of Chlorpromazine and Haloperidol Combination on Lipid LevelstrianaamaliaNo ratings yet
- Disease The British Journal of Diabetes & VascularDocument6 pagesDisease The British Journal of Diabetes & VascularEstiPramestiningtyasNo ratings yet
- Sitagliptin vs. Pioglitazone As Add-On Treatments in Patients With Uncontrolled Type 2 Diabetes On The Maximal Dose of Metformin Plus SulfonylureaDocument9 pagesSitagliptin vs. Pioglitazone As Add-On Treatments in Patients With Uncontrolled Type 2 Diabetes On The Maximal Dose of Metformin Plus SulfonylureaFebi FernandaNo ratings yet
- Gliclazide Metformin Study Type 2 Diabetes PatientsDocument7 pagesGliclazide Metformin Study Type 2 Diabetes PatientsLyka MahrNo ratings yet
- Hiperglucemia TX en HospitalDocument4 pagesHiperglucemia TX en HospitalAmado OrozcoNo ratings yet
- j3 2010Document12 pagesj3 2010Taha FransNo ratings yet
- Contraindications To Vasoconstrictors in Dentistry: Part IIDocument5 pagesContraindications To Vasoconstrictors in Dentistry: Part IIBunga Erlita RosaliaNo ratings yet
- Aqua AhfDocument8 pagesAqua AhfRinzyNo ratings yet
- Efficacy and Safety of Amlodipine Versus Captopril and Their Combination Inhypertensive Urgency A Randomized Controlled Trial 2329 9126 1000274 PDFDocument7 pagesEfficacy and Safety of Amlodipine Versus Captopril and Their Combination Inhypertensive Urgency A Randomized Controlled Trial 2329 9126 1000274 PDFMaya sariNo ratings yet
- Metformin and insulin combo may help type 1 diabetesDocument6 pagesMetformin and insulin combo may help type 1 diabetescarlos garridoNo ratings yet
- CLC 4960230910Document7 pagesCLC 4960230910walnut21No ratings yet
- Diabetic Nephropathy: Landmark Clinical TrialsDocument45 pagesDiabetic Nephropathy: Landmark Clinical TrialsTRP TSYONo ratings yet
- Eficiencia y Tolerabilidad Glimepirida y MetfomrinaDocument7 pagesEficiencia y Tolerabilidad Glimepirida y MetfomrinaMarioA.VelascoCórdobaNo ratings yet
- Bantuan Hidup Dasar SDKDocument22 pagesBantuan Hidup Dasar SDKghea_86No ratings yet
- Randomized Evaluation of A Novel, Fixed-Dose Combination of Perindopril 3.5 Mg/amlodipine 2.5 MG As A First-Step Treatment in HypertensionDocument10 pagesRandomized Evaluation of A Novel, Fixed-Dose Combination of Perindopril 3.5 Mg/amlodipine 2.5 MG As A First-Step Treatment in HypertensionVu ChuNo ratings yet
- Sulodexide For Kidney Protection in Type 2 Diabetes PatientsDocument8 pagesSulodexide For Kidney Protection in Type 2 Diabetes PatientsFerdinand YuzonNo ratings yet
- Efficacy and Safety Comparison of Liraglutide, Glimepiride, and Placebo, All in Combination With Metformin, in Type 2 DiabetesDocument7 pagesEfficacy and Safety Comparison of Liraglutide, Glimepiride, and Placebo, All in Combination With Metformin, in Type 2 DiabetesOzi ThingkingandactionNo ratings yet
- VHRM 5 1043Document16 pagesVHRM 5 1043AldiKurosakiNo ratings yet
- A Pilot Study On The Effect of Telmisartan & Ramipril On 24 H Blood Pressure Profile & Dipping Pattern in Type 1 Diabetes Patients With NephropathyDocument6 pagesA Pilot Study On The Effect of Telmisartan & Ramipril On 24 H Blood Pressure Profile & Dipping Pattern in Type 1 Diabetes Patients With Nephropathydini hanifaNo ratings yet
- Ruilope-2015-The Journal of Clinical HypertensionDocument8 pagesRuilope-2015-The Journal of Clinical HypertensionMiriam BlejerNo ratings yet
- Surpass 1Document13 pagesSurpass 1Fernando DominguezNo ratings yet
- Why Hard To Control Blood Pressure ?: Atma GunawanDocument35 pagesWhy Hard To Control Blood Pressure ?: Atma GunawanLies Pramana SariNo ratings yet
- English JournalDocument4 pagesEnglish JournalRamya HarlistyaNo ratings yet
- Hormone Therapy in Postmenopausal WomenDocument8 pagesHormone Therapy in Postmenopausal WomenChyntia Pramita SariNo ratings yet
- 13463-Article Text-25834-1-10-20210103Document3 pages13463-Article Text-25834-1-10-20210103Melly SyafridaNo ratings yet
- Coronary Atery Disease-Htn-Thrombo QuestionsDocument38 pagesCoronary Atery Disease-Htn-Thrombo Questionssrivari sriniNo ratings yet
- Medical AbbreviationDocument37 pagesMedical AbbreviationJessica QueNo ratings yet
- Journal Reading DementiaDocument17 pagesJournal Reading DementiaAtayaNo ratings yet
- Warning Signs of Problem PregnancyDocument1 pageWarning Signs of Problem PregnancyZarmayana Nur KhairunniNo ratings yet
- Fletcher 2016Document10 pagesFletcher 2016Christina Putri BongzueNo ratings yet
- Clinical Manifestations and Diagnosis of Turner Syndrome PDFDocument50 pagesClinical Manifestations and Diagnosis of Turner Syndrome PDFcesar chiangNo ratings yet
- IFOMPT Cervical Framework Final September 2020Document41 pagesIFOMPT Cervical Framework Final September 2020Maximiliano LabraNo ratings yet
- Antihypertensive Effect of Celery Seed On Rat Blood Pressure in Chronic AdministrationDocument6 pagesAntihypertensive Effect of Celery Seed On Rat Blood Pressure in Chronic AdministrationHapsah FarmasiNo ratings yet
- Blaylock Hypertension 13Document16 pagesBlaylock Hypertension 13mohanp71No ratings yet
- Cardiology. Scheme ..Dof3tna - Net... EgyDrDocument4 pagesCardiology. Scheme ..Dof3tna - Net... EgyDrJilan El SherBiny100% (1)
- Stroke Conference PDFDocument729 pagesStroke Conference PDFgelvin27No ratings yet
- Unit 7 Preventive PediatricsDocument16 pagesUnit 7 Preventive PediatricsSanthosh.S.U58% (12)
- A Lecture Schedule, July 2015-June 2016Document12 pagesA Lecture Schedule, July 2015-June 2016Shahriar Kabir DaneNo ratings yet
- PART TWO - Preferred Practice PatternsDocument272 pagesPART TWO - Preferred Practice PatternsCherrie Anne MiguelNo ratings yet
- Hypertension in PregnancyDocument29 pagesHypertension in PregnancyArchana KumariNo ratings yet
- Yoga and LifestyleDocument13 pagesYoga and LifestylelohotaNo ratings yet
- Why Do Anti Hypertensives Cause CoughDocument2 pagesWhy Do Anti Hypertensives Cause CoughArleen Devita100% (1)
- Dietary Management of GI DiseasesDocument12 pagesDietary Management of GI DiseasesMiguel Cuevas DolotNo ratings yet
- Chronic Kidney DiseaseDocument22 pagesChronic Kidney DiseaseAchmad ZainudinNo ratings yet
- Stress ManagementDocument85 pagesStress ManagementAnonymous MhCdtwxQINo ratings yet
- Kidney DiseasesDocument22 pagesKidney Diseasesphoto copyhemnNo ratings yet
- Ref Case 1 - PSAP Combining ALL Guideline For HT PDFDocument22 pagesRef Case 1 - PSAP Combining ALL Guideline For HT PDFYunistya Dwi CahyaniNo ratings yet
- The Nutraceutical Role of Pumpkin Seed and Its Health Eff Ect - A ReviewDocument6 pagesThe Nutraceutical Role of Pumpkin Seed and Its Health Eff Ect - A ReviewTULLIMILLI CHANIKYA VENKAT KRISHNA SAI 2200268No ratings yet
- 38 Health Benefits of YogaDocument19 pages38 Health Benefits of YogaumaNo ratings yet
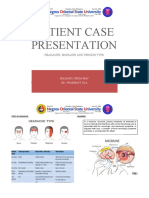
- Patient Case Presentation: Headache: Migraine and Tension TypeDocument31 pagesPatient Case Presentation: Headache: Migraine and Tension TypeKathleen B Baldado100% (4)
- Congenital Diaphragmatic Hernia in The Neonate - UpToDate PDFDocument38 pagesCongenital Diaphragmatic Hernia in The Neonate - UpToDate PDFJosé Abraham Amaya DuarteNo ratings yet
- Makalah Trauma KepalaDocument39 pagesMakalah Trauma KepalalaudyaNo ratings yet
- Full Download Test Bank For Gerontological Nursing 3 Edition Patricia A Tabloski PDF Full ChapterDocument23 pagesFull Download Test Bank For Gerontological Nursing 3 Edition Patricia A Tabloski PDF Full Chapterroamerempyemax4n5100% (15)
- Health HistoryDocument8 pagesHealth HistoryQurrat Ul Ain FaizanNo ratings yet
- Find Your Path: Honor Your Body, Fuel Your Soul, and Get Strong with the Fit52 LifeFrom EverandFind Your Path: Honor Your Body, Fuel Your Soul, and Get Strong with the Fit52 LifeRating: 4 out of 5 stars4/5 (3)
- Summary: Fast Like a Girl: A Woman’s Guide to Using the Healing Power of Fasting to Burn Fat, Boost Energy, and Balance Hormones: Key Takeaways, Summary and AnalysisFrom EverandSummary: Fast Like a Girl: A Woman’s Guide to Using the Healing Power of Fasting to Burn Fat, Boost Energy, and Balance Hormones: Key Takeaways, Summary and AnalysisRating: 3 out of 5 stars3/5 (2)
- Body Love Every Day: Choose Your Life-Changing 21-Day Path to Food FreedomFrom EverandBody Love Every Day: Choose Your Life-Changing 21-Day Path to Food FreedomRating: 4 out of 5 stars4/5 (1)
- The Diabetes Code: Prevent and Reverse Type 2 Diabetes NaturallyFrom EverandThe Diabetes Code: Prevent and Reverse Type 2 Diabetes NaturallyRating: 5 out of 5 stars5/5 (1)
- Forever Strong: A New, Science-Based Strategy for Aging WellFrom EverandForever Strong: A New, Science-Based Strategy for Aging WellNo ratings yet
- Secrets From the Eating Lab: The Science of Weight Loss, the Myth of Willpower, and Why You Should Never Diet AgainFrom EverandSecrets From the Eating Lab: The Science of Weight Loss, the Myth of Willpower, and Why You Should Never Diet AgainRating: 3.5 out of 5 stars3.5/5 (38)
- Sugar Crush: How to Reduce Inflammation, Reverse Nerve Damage, and Reclaim Good HealthFrom EverandSugar Crush: How to Reduce Inflammation, Reverse Nerve Damage, and Reclaim Good HealthRating: 4 out of 5 stars4/5 (6)
- Happy Gut: The Cleansing Program to Help You Lose Weight, Gain Energy, and Eliminate PainFrom EverandHappy Gut: The Cleansing Program to Help You Lose Weight, Gain Energy, and Eliminate PainRating: 3.5 out of 5 stars3.5/5 (6)
- Allen Carr's Easy Way for Women to Lose Weight: The original Easyway methodFrom EverandAllen Carr's Easy Way for Women to Lose Weight: The original Easyway methodRating: 4.5 out of 5 stars4.5/5 (18)
- Instant Loss On a Budget: Super-Affordable Recipes for the Health-Conscious CookFrom EverandInstant Loss On a Budget: Super-Affordable Recipes for the Health-Conscious CookRating: 3.5 out of 5 stars3.5/5 (2)
- Glucose Goddess Method: A 4-Week Guide to Cutting Cravings, Getting Your Energy Back, and Feeling AmazingFrom EverandGlucose Goddess Method: A 4-Week Guide to Cutting Cravings, Getting Your Energy Back, and Feeling AmazingRating: 5 out of 5 stars5/5 (59)
- Keto Friendly Recipes: Easy Keto For Busy PeopleFrom EverandKeto Friendly Recipes: Easy Keto For Busy PeopleRating: 3.5 out of 5 stars3.5/5 (2)
- The Food Lover's Cleanse: 140 Delicious, Nourishing Recipes That Will Tempt You Back into Healthful EatingFrom EverandThe Food Lover's Cleanse: 140 Delicious, Nourishing Recipes That Will Tempt You Back into Healthful EatingRating: 4 out of 5 stars4/5 (3)
- The Beck Diet Solution Weight Loss Workbook: The 6-Week Plan to Train Your Brain to Think Like a Thin PersonFrom EverandThe Beck Diet Solution Weight Loss Workbook: The 6-Week Plan to Train Your Brain to Think Like a Thin PersonRating: 3.5 out of 5 stars3.5/5 (33)
- Proteinaholic: How Our Obsession with Meat Is Killing Us and What We Can Do About ItFrom EverandProteinaholic: How Our Obsession with Meat Is Killing Us and What We Can Do About ItRating: 4.5 out of 5 stars4.5/5 (19)
- The Arm: Inside the Billion-Dollar Mystery of the Most Valuable Commodity in SportsFrom EverandThe Arm: Inside the Billion-Dollar Mystery of the Most Valuable Commodity in SportsRating: 4 out of 5 stars4/5 (49)
- The Fast800 Diet: Discover the Ideal Fasting Formula to Shed Pounds, Fight Disease, and Boost Your Overall HealthFrom EverandThe Fast800 Diet: Discover the Ideal Fasting Formula to Shed Pounds, Fight Disease, and Boost Your Overall HealthRating: 5 out of 5 stars5/5 (37)
- Foods That Cause You to Lose Weight: The Negative Calorie EffectFrom EverandFoods That Cause You to Lose Weight: The Negative Calorie EffectRating: 3 out of 5 stars3/5 (5)
- Metabolism Revolution: Lose 14 Pounds in 14 Days and Keep It Off for LifeFrom EverandMetabolism Revolution: Lose 14 Pounds in 14 Days and Keep It Off for LifeNo ratings yet
- How to Be Well: The 6 Keys to a Happy and Healthy LifeFrom EverandHow to Be Well: The 6 Keys to a Happy and Healthy LifeRating: 5 out of 5 stars5/5 (1)
- Hungry for Change: Ditch the Diets, Conquer the Cravings, and Eat Your Way to Lifelong HealthFrom EverandHungry for Change: Ditch the Diets, Conquer the Cravings, and Eat Your Way to Lifelong HealthRating: 4 out of 5 stars4/5 (7)
- The Candida Cure: The 90-Day Program to Balance Your Gut, Beat Candida, and Restore Vibrant HealthFrom EverandThe Candida Cure: The 90-Day Program to Balance Your Gut, Beat Candida, and Restore Vibrant HealthNo ratings yet
- The Complete Beck Diet for Life: The 5-Stage Program for Permanent Weight LossFrom EverandThe Complete Beck Diet for Life: The 5-Stage Program for Permanent Weight LossRating: 3.5 out of 5 stars3.5/5 (6)
- Eat to Lose, Eat to Win: Your Grab-n-Go Action Plan for a Slimmer, Healthier YouFrom EverandEat to Lose, Eat to Win: Your Grab-n-Go Action Plan for a Slimmer, Healthier YouNo ratings yet
- Summary of Mary Claire Haver's The Galveston DietFrom EverandSummary of Mary Claire Haver's The Galveston DietRating: 5 out of 5 stars5/5 (1)
- The Volumetrics Eating Plan: Techniques and Recipes for Feeling Full on Fewer CaloriesFrom EverandThe Volumetrics Eating Plan: Techniques and Recipes for Feeling Full on Fewer CaloriesNo ratings yet
- The Whole Body Reset: Your Weight-Loss Plan for a Flat Belly, Optimum Health & a Body You'll Love at Midlife and BeyondFrom EverandThe Whole Body Reset: Your Weight-Loss Plan for a Flat Belly, Optimum Health & a Body You'll Love at Midlife and BeyondRating: 4.5 out of 5 stars4.5/5 (28)
- The Longevity Plan: Seven Life-Transforming Lessons from Ancient ChinaFrom EverandThe Longevity Plan: Seven Life-Transforming Lessons from Ancient ChinaNo ratings yet