You might also like
- Cengage Advantage American Foreign Policy and Process 6th Edition McCormick Test Bank DownloadDocument8 pagesCengage Advantage American Foreign Policy and Process 6th Edition McCormick Test Bank DownloadBen Flott100% (24)
- Motions, Affidavits, Answers, and Commercial Liens - The Book of Effective Sample DocumentsFrom EverandMotions, Affidavits, Answers, and Commercial Liens - The Book of Effective Sample DocumentsRating: 4.5 out of 5 stars4.5/5 (14)
- pHILHEALTH cLAIM sIGNATURE fORMDocument1 pagepHILHEALTH cLAIM sIGNATURE fORMBellezrah100% (4)
- PhilHealth Member Registration Form (PMRF)Document2 pagesPhilHealth Member Registration Form (PMRF)Vinson Gabato78% (9)
- Auto Loan For Individual and Single Proprietorship - Application FormDocument2 pagesAuto Loan For Individual and Single Proprietorship - Application FormEymard Siojo67% (3)
- CSFDocument1 pageCSFChristopher Garrata Galano Jr.50% (2)
- Claimsignatureform PDFDocument1 pageClaimsignatureform PDFClaire VillanuevaNo ratings yet
- Important Reminders:: (Claim Form)Document1 pageImportant Reminders:: (Claim Form)abejhieNo ratings yet
- Philippine Health Insurance Corporation: Part I - Member InformationDocument1 pagePhilippine Health Insurance Corporation: Part I - Member InformationjhunNo ratings yet
- Pag Ibig 1Document2 pagesPag Ibig 1Fervi Louie Jalop Bongco0% (1)
- Sido Benita Chomacog 0 5 1 1 1 9 5 3 X: Poblacion Mankayan Benguet PhilippinesDocument1 pageSido Benita Chomacog 0 5 1 1 1 9 5 3 X: Poblacion Mankayan Benguet PhilippinesPrinston Del CampoNo ratings yet
- Phil Health ClaimForm GuidelinesDocument7 pagesPhil Health ClaimForm GuidelinesFerdinand CordovizNo ratings yet
- PhilHealth ClaimForm1 GuidelinesDocument4 pagesPhilHealth ClaimForm1 GuidelinesAsh CampiaoNo ratings yet
- (Claim Signature Form) : Business Name of EmployerDocument2 pages(Claim Signature Form) : Business Name of EmployerVirgilioNo ratings yet
- (176736967) PMRF - RevisedDocument3 pages(176736967) PMRF - Revisedanon_902897556No ratings yet
- Philippine Health Insurance Corporation: Part I - Member and Patient Information and CertificationDocument2 pagesPhilippine Health Insurance Corporation: Part I - Member and Patient Information and CertificationLGU-SUAL MTONo ratings yet
- Deped Cabuyao: (Claim Form 1) Revised November 2013 Series #Document1 pageDeped Cabuyao: (Claim Form 1) Revised November 2013 Series #Wehn LustreNo ratings yet
- ClaimSignatureForm PDFDocument1 pageClaimSignatureForm PDFMuli MJNo ratings yet
- Philippine Health Insurance Corporation: Part I - Member InformationDocument1 pagePhilippine Health Insurance Corporation: Part I - Member InformationSnyrah AmbagNo ratings yet
- Membership Update FormDocument4 pagesMembership Update FormbmapiraNo ratings yet
- Philhealth ClaimForm1 SignedDocument1 pagePhilhealth ClaimForm1 Signedjobelyn calaudNo ratings yet
- CSF PDFDocument1 pageCSF PDFGin ArienzaNo ratings yet
- Claim Signature Form (CSF)Document2 pagesClaim Signature Form (CSF)hrgailarceta22No ratings yet
- CF1 JabasDocument1 pageCF1 JabasqarlbalongNo ratings yet
- Special Form of Request For Payment of United States Savings and Retirement Securities Where Use of A Detached Request Is AuthorizedDocument4 pagesSpecial Form of Request For Payment of United States Savings and Retirement Securities Where Use of A Detached Request Is AuthorizedMalika Shamsid-deenNo ratings yet
- This Form Is Not For SaleDocument2 pagesThis Form Is Not For Saletheia28No ratings yet
- Ssa 7050Document4 pagesSsa 7050tobehode100% (1)
- Claim Form - 2018Document2 pagesClaim Form - 2018Ronaldo De MesaNo ratings yet
- M1AFDocument2 pagesM1AFkrystaliciousNo ratings yet
- NPSLite Subscriberr Registration FormDocument4 pagesNPSLite Subscriberr Registration FormSubhash Tantuvay DhavaryaNo ratings yet
- IRS Form F3949ADocument2 pagesIRS Form F3949APolarik100% (1)
- I-730, Refugee/Asylee Relative Petition: Do Not Write in This Block - For Uscis Office OnlyDocument4 pagesI-730, Refugee/Asylee Relative Petition: Do Not Write in This Block - For Uscis Office Onlycarmenperez084No ratings yet
- OCC Complaint FormDocument5 pagesOCC Complaint FormTim BryantNo ratings yet
- Consent For Release of Information: WWW - Ssa.gov/online/ssa-7050 PDFDocument2 pagesConsent For Release of Information: WWW - Ssa.gov/online/ssa-7050 PDFlaucanelosNo ratings yet
- Application For Financial Assistance For Undergraduate Studies in 2013Document6 pagesApplication For Financial Assistance For Undergraduate Studies in 2013211505006No ratings yet
- Uhip Claim Form July 2006-1-40Document1 pageUhip Claim Form July 2006-1-40CollinNo ratings yet
- Sec 1014Document2 pagesSec 1014Michael100% (1)
- Application Form For Reviewer: Part I: Basic InformationDocument2 pagesApplication Form For Reviewer: Part I: Basic InformationKrushnasamy SuramaniyanNo ratings yet
- I 134instructivoDocument7 pagesI 134instructivorosita camejoNo ratings yet
- Proforma of ApplicationDocument3 pagesProforma of ApplicationJeshiNo ratings yet
- New Starter FormDocument5 pagesNew Starter FormRajagopal BojanapalliNo ratings yet
- Sss 10Document2 pagesSss 10Aila ReoptaNo ratings yet
- 2018 Claim Signature FormDocument1 page2018 Claim Signature FormLorence VillaceranNo ratings yet
- SSSForms UMID ApplicationDocument2 pagesSSSForms UMID ApplicationRomer Bryan De Castro100% (1)
- Blue Card Volunteer FormDocument4 pagesBlue Card Volunteer FormWednesday FelodeseNo ratings yet
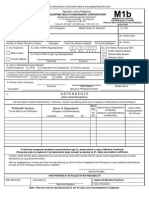
- Philhealth m1bDocument2 pagesPhilhealth m1bJuan Luis Lusong50% (2)
- Social Security: The New Rules, Essentials & Maximizing Your Social Security, Retirement, Medicare, Pensions & Benefits Explained In One PlaceFrom EverandSocial Security: The New Rules, Essentials & Maximizing Your Social Security, Retirement, Medicare, Pensions & Benefits Explained In One PlaceNo ratings yet
- Get Approved: Grant Writing Secrets Most Grant Givers Do Not Want You To Know – Even In a Bad EconomyFrom EverandGet Approved: Grant Writing Secrets Most Grant Givers Do Not Want You To Know – Even In a Bad EconomyRating: 5 out of 5 stars5/5 (3)
- Credit Report Secrets: How to Understand What Your Credit Report Says About You and What You Can Do About It!From EverandCredit Report Secrets: How to Understand What Your Credit Report Says About You and What You Can Do About It!Rating: 1 out of 5 stars1/5 (2)
- How to Enroll in Medicare Health Insurance: Choose a Medicare Part D Drug Plan and a Medicare Supplement PlanFrom EverandHow to Enroll in Medicare Health Insurance: Choose a Medicare Part D Drug Plan and a Medicare Supplement PlanNo ratings yet
- Health Care Reform Act: Critical Tax and Insurance RamificationsFrom EverandHealth Care Reform Act: Critical Tax and Insurance RamificationsNo ratings yet
- The Evolution of Irregular War PDFDocument15 pagesThe Evolution of Irregular War PDFAnonymous mfgFBX9X100% (1)
- PPTDocument19 pagesPPTShivika Chanda100% (1)
- Ravindra V Parmar Vs All India Radio On 16 April 2019Document10 pagesRavindra V Parmar Vs All India Radio On 16 April 2019Asokaraj SubbiahNo ratings yet
- WWW Azerbaijanvisa OrgDocument3 pagesWWW Azerbaijanvisa OrgAzerbaijan VisaNo ratings yet
- Lease DeedDocument3 pagesLease Deedvineeth babuNo ratings yet
- Ifsc Code PDFDocument5 pagesIfsc Code PDFZahid MushtaqNo ratings yet
- TimesofindiaDocument30 pagesTimesofindiaGopi GopinathanNo ratings yet
- Ramos v. ImbangDocument1 pageRamos v. ImbangCamille BugtasNo ratings yet
- General Knowledge For CompetitiveDocument593 pagesGeneral Knowledge For CompetitiveBrijesh VermaNo ratings yet
- Affidavit of Loss TemplateDocument1 pageAffidavit of Loss TemplatefirstnamezaplanNo ratings yet
- Test Bank For Cengage Advantage Books American Government and Politics Today Brief Edition 2012 2013 7th Edition by Schmidt Shelley and Bardes ISBN 1111832935 9781111832933Document36 pagesTest Bank For Cengage Advantage Books American Government and Politics Today Brief Edition 2012 2013 7th Edition by Schmidt Shelley and Bardes ISBN 1111832935 9781111832933mrjamesjohnsondvmagojbfemnc100% (19)
- 1897 The Constitution of Biak-Na-BatoDocument16 pages1897 The Constitution of Biak-Na-BatoririNo ratings yet
- Template of SB Resolution Adopting Brgy Road Clearing Action PlanDocument2 pagesTemplate of SB Resolution Adopting Brgy Road Clearing Action PlanJonathanNo ratings yet
- Christian Citizens in Islamic State .The Pakistan ExperienceDocument133 pagesChristian Citizens in Islamic State .The Pakistan ExperienceSyedAmirShah100% (1)
- GST Update 14.10.2017Document35 pagesGST Update 14.10.2017dipaliNo ratings yet
- Order of RecusalDocument2 pagesOrder of RecusalLindsey BasyeNo ratings yet
- Craneveyor Corp. v. City of Rancho Cucamonga, No. 22-55435 (9th Cir. Apr. 20, 2023) (Mem.)Document5 pagesCraneveyor Corp. v. City of Rancho Cucamonga, No. 22-55435 (9th Cir. Apr. 20, 2023) (Mem.)RHTNo ratings yet
- Jinnah Creator of Pakistan by Hector BolithoDocument268 pagesJinnah Creator of Pakistan by Hector BolithoSarfarazDurrani100% (3)
- Mock QuestionsDocument9 pagesMock QuestionsNguyễn Chí DũngNo ratings yet
- Diversity in Health Conference.2010.Tpch MWGDocument17 pagesDiversity in Health Conference.2010.Tpch MWGSharon A StockerNo ratings yet
- 011-Franklin Baker Company v. Trajano G.R. No. 75039 January 28, 1988Document2 pages011-Franklin Baker Company v. Trajano G.R. No. 75039 January 28, 1988Janeen ZamudioNo ratings yet
- Consti2Digest - Gonzales Vs Comelec, 21 SCRA 774, G.R. No. L-28196 (9 Nov 1967)Document2 pagesConsti2Digest - Gonzales Vs Comelec, 21 SCRA 774, G.R. No. L-28196 (9 Nov 1967)Lu Cas0% (1)
- Join Indian Army: Indian Army Directorate General of Recruiting CHE/TAM/COI/SGD/2017/125783Document2 pagesJoin Indian Army: Indian Army Directorate General of Recruiting CHE/TAM/COI/SGD/2017/125783Kamesh coolNo ratings yet
- Sardar PatelDocument32 pagesSardar PatelPranoy BaishyaNo ratings yet
- ChecklistDocument2 pagesChecklistJames Brian Garcia GarayNo ratings yet
- 2378group2 Economy II Section III Unit II APlo Praja Pampini Vyavastha Panitheeru VivaranaDocument9 pages2378group2 Economy II Section III Unit II APlo Praja Pampini Vyavastha Panitheeru VivaranaphaniNo ratings yet
- UPSC Civil Services Exam 2023Document21 pagesUPSC Civil Services Exam 2023Amrish TrivediNo ratings yet
- Santos SR Vs CaDocument2 pagesSantos SR Vs CaFoo BarNo ratings yet
- 2016 Complete Allied Political Law NotesDocument49 pages2016 Complete Allied Political Law Notesalyza burdeosNo ratings yet