You might also like
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Ocampo - v. - Arcaya-ChuaDocument42 pagesOcampo - v. - Arcaya-ChuaChristie Joy BuctonNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Assets Book Value Estimated Realizable ValuesDocument3 pagesAssets Book Value Estimated Realizable ValuesEllyza SerranoNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Land Laws (MOHD AQIB SF)Document18 pagesLand Laws (MOHD AQIB SF)Mohd AqibNo ratings yet
- Sally Tour: TOUR ITINRARY With QuoteDocument2 pagesSally Tour: TOUR ITINRARY With QuoteGuillermo Gundayao Jr.No ratings yet
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Literature Component SPM'13 Form 4 FullDocument12 pagesLiterature Component SPM'13 Form 4 FullNur Izzati Abd ShukorNo ratings yet
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- 1 Summative Test in Empowerment Technology Name: - Date: - Year & Section: - ScoreDocument2 pages1 Summative Test in Empowerment Technology Name: - Date: - Year & Section: - ScoreShelene CathlynNo ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Quality Audit Report TemplateDocument3 pagesQuality Audit Report TemplateMercy EdemNo ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Ethical Dilemma Notes KiitDocument4 pagesEthical Dilemma Notes KiitAritra MahatoNo ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Text and Meaning in Stanley FishDocument5 pagesText and Meaning in Stanley FishparthNo ratings yet
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- 26candao Vs People of The Philipines, 664 SCRA 769, G.R. No. 186659-710, February 1, 2012Document5 pages26candao Vs People of The Philipines, 664 SCRA 769, G.R. No. 186659-710, February 1, 2012Gi NoNo ratings yet
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Entrepreneurship: The Entrepreneur, The Individual That SteersDocument11 pagesEntrepreneurship: The Entrepreneur, The Individual That SteersJohn Paulo Sayo0% (1)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Authors & Abstract Guideline V-ASMIUA 2020Document8 pagesAuthors & Abstract Guideline V-ASMIUA 2020tiopanNo ratings yet
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Morals and Dogma of The Ineffable DegreesDocument134 pagesMorals and Dogma of The Ineffable DegreesCelephaïs Press / Unspeakable Press (Leng)86% (7)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
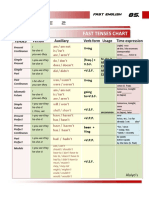
- Table 2: Fast Tenses ChartDocument5 pagesTable 2: Fast Tenses ChartAngel Julian HernandezNo ratings yet
- 4th Exam Report - Cabales V CADocument4 pages4th Exam Report - Cabales V CAGennard Michael Angelo AngelesNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Baggage Handling Solutions LQ (Mm07854)Document4 pagesBaggage Handling Solutions LQ (Mm07854)Sanjeev SiwachNo ratings yet
- PDF Issue 1 PDFDocument128 pagesPDF Issue 1 PDFfabrignani@yahoo.comNo ratings yet
- Iraq-A New Dawn: Mena Oil Research - July 2021Document29 pagesIraq-A New Dawn: Mena Oil Research - July 2021Beatriz RosenburgNo ratings yet
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Annaphpapp 01Document3 pagesAnnaphpapp 01anujhanda29No ratings yet
- 1 Rodney Britton v. Apple Inc. Job Descrimination, Sexual HarrassmentDocument8 pages1 Rodney Britton v. Apple Inc. Job Descrimination, Sexual HarrassmentJack PurcherNo ratings yet
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- People Vs Gonzales-Flores - 138535-38 - April 19, 2001 - JDocument10 pagesPeople Vs Gonzales-Flores - 138535-38 - April 19, 2001 - JTrexPutiNo ratings yet
- B. Contract of Sale: D. Fraud in FactumDocument5 pagesB. Contract of Sale: D. Fraud in Factumnavie VNo ratings yet
- A#2 8612 SehrishDocument16 pagesA#2 8612 SehrishMehvish raniNo ratings yet
- Things Fall ApartDocument4 pagesThings Fall ApartJack ConnollyNo ratings yet
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Second Grading Science 6 Worksheet 16 Code: S6Mtiii-J-5Document3 pagesSecond Grading Science 6 Worksheet 16 Code: S6Mtiii-J-5Catherine Lagario RenanteNo ratings yet
- The Holy Rosary 2Document14 pagesThe Holy Rosary 2Carmilita Mi AmoreNo ratings yet
- Fundamentals of Product and Service CostingDocument28 pagesFundamentals of Product and Service CostingPetronella AyuNo ratings yet
- Slavfile: in This IssueDocument34 pagesSlavfile: in This IssueNora FavorovNo ratings yet
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Catalog - Focus ElectronicDocument14 pagesCatalog - Focus ElectronicLi KurtNo ratings yet
- Account Number:: Rate: Date Prepared: RS-Residential ServiceDocument4 pagesAccount Number:: Rate: Date Prepared: RS-Residential ServiceAhsan ShabirNo ratings yet
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)